




The annual incidence of gastric cancer in our country is estimated at 6.6 cases/100 000 inhabitants. It is associated with high mortality rates due to its biological aggressiveness and its diagnosis in advanced stages in our setting.
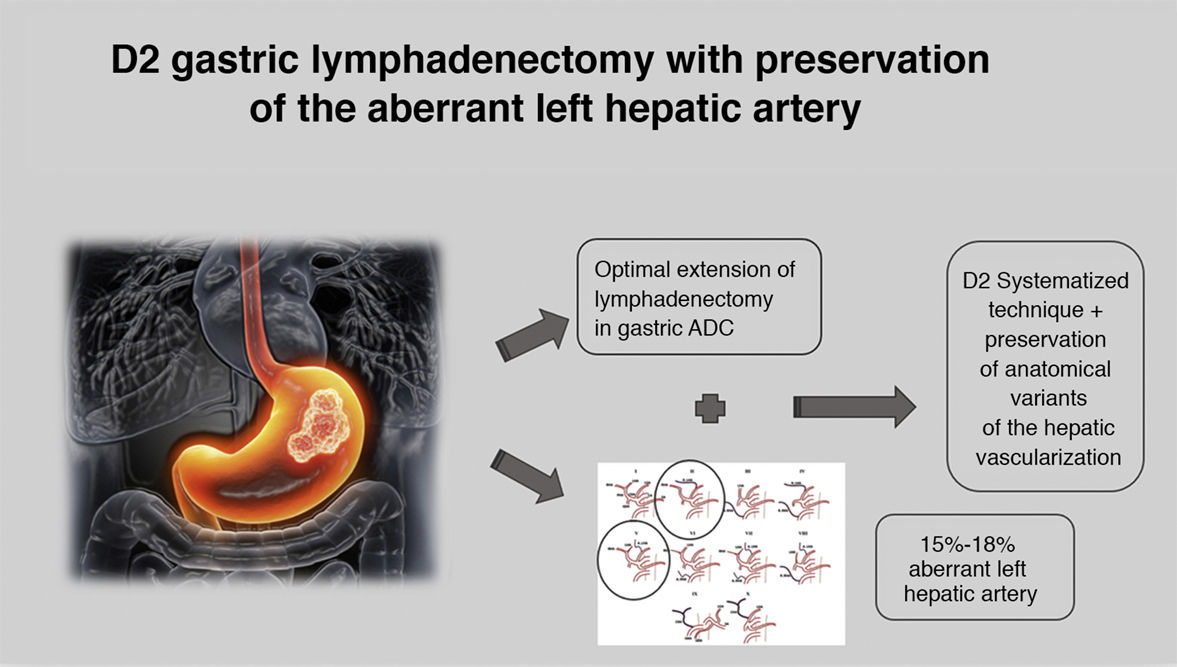
The number of affected lymph nodes is one of the main prognostic factors. The most recent clinical guidelines (5th Edition) by the Japanese Gastric Cancer Association define D2 lymph node dissection (D2: D1 + 8a, 9, 11p, 11d, 12a) as the optimal extension of the lymphadenectomy associated with total gastrectomy for gastric cancer, excluding group 10.
Variations in the hepatic arterial anatomy are not uncommon, and an aberrant left hepatic artery appears in up to 15%–18% of cases.
To avoid alterations in hepatic perfusion, it is important to identify and preserve these arterial branches.
Video: standard laparoscopic D2 lymphadenectomy.
Please cite this article as: Puerta A, Cuadrado M, Vilar JA, Priego P. Linfadenectomía gástrica D2 con preservación de arteria hepática izquierda aberrante. Cir Esp. 2021;99:539.
