




We are writing this letter in relation to the article published in January 2022 by Bueno-Lledo et al.1 “Negative pressure therapy in abdominal wall surgery”, which we read with great interest. With regard to this paper, we would like to address a number of considerations.
As described by Bueno-Lledo et al., the management of complex abdominal wounds through the use of negative pressure systems (NPWT) has improved greatly in the last decade.1 Thus, the potential indications for this therapy have multiplied and this is reflected in the exponential increase in publications in recent years.
The therapy can be applied in multiple surgical scenarios (support of surgical wound closure by secondary intention, management of the open abdomen with fascial traction, prosthetic infections in order to save the surgical mesh, among many others). Thanks to the experience gained in the management of adult patients, there is an increasing literature on the use of NPT in paediatrics. Currently, it is even possible to adapt the system for application in complex abdominal wounds in newborns, as well as in premature or underweight children.2 (Fig. 1)
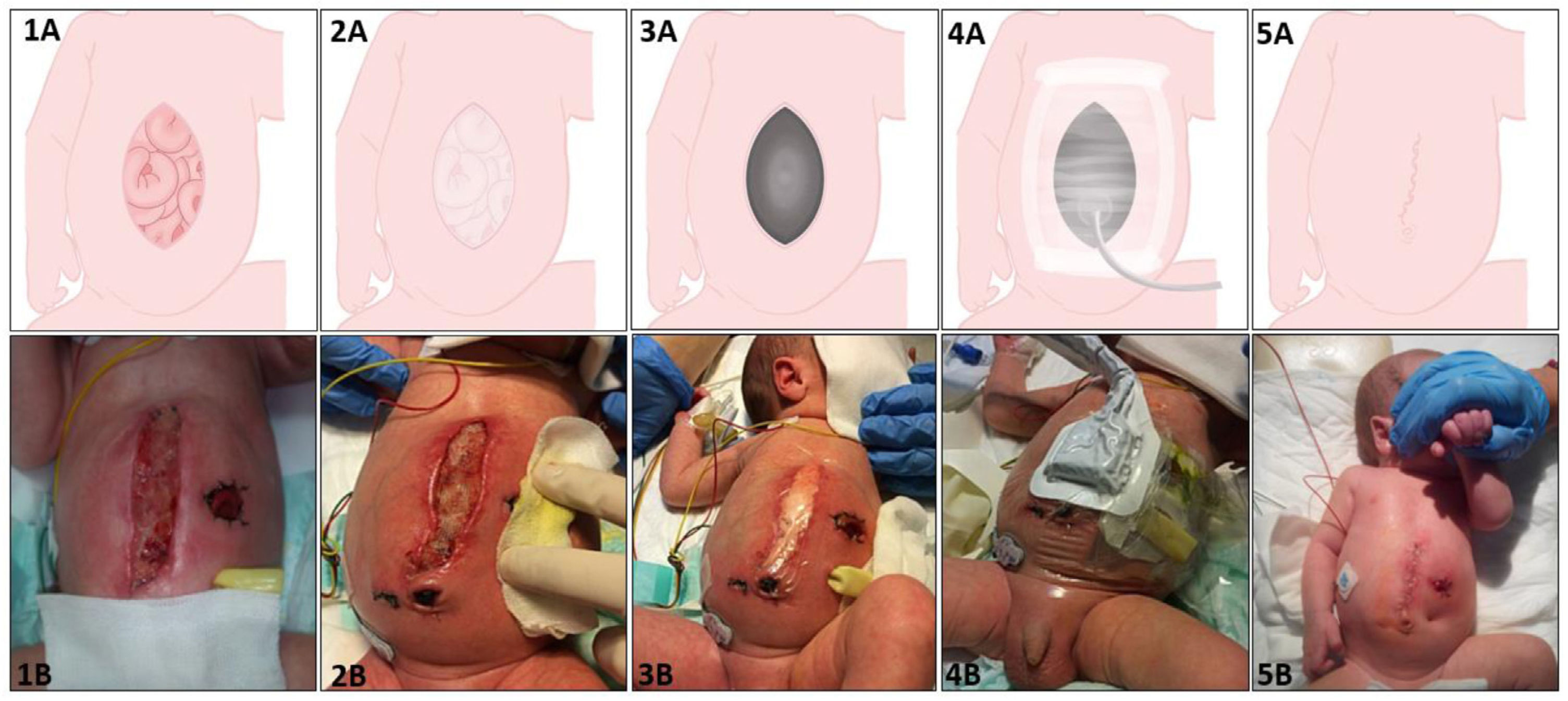
. 1A–B) Peritoneal or intestinal exposure of the surgical wound. 2A–B) Placement of the non-adherent abdominal viscera protection sheet. In neonates we use a Linitul® sheet as protection. 3A–B) Placement of the polyurethane sponge covering the abdominal defect. In neonates, we use wet gauze because it is easy to adapt to the shape of the surgical wound. 4A–B) Placement of the suction system. In neonates we use an initial pressure of −10 to −20 mmHg (intermittent), with progressive elevation according to the haemodynamic tolerance of the patient, with a maximum of −50 mmHg. 5A–B) Final result after application of negative pressure therapy.")
Placement of staged abdominal negative pressure therapy (correlation between graphical representation and representation in a neonate with interventional necrotising enterocolitis). 1A–B) Peritoneal or intestinal exposure of the surgical wound. 2A–B) Placement of the non-adherent abdominal viscera protection sheet. In neonates we use a Linitul® sheet as protection. 3A–B) Placement of the polyurethane sponge covering the abdominal defect. In neonates, we use wet gauze because it is easy to adapt to the shape of the surgical wound. 4A–B) Placement of the suction system. In neonates we use an initial pressure of −10 to −20 mmHg (intermittent), with progressive elevation according to the haemodynamic tolerance of the patient, with a maximum of −50 mmHg. 5A–B) Final result after application of negative pressure therapy.
Despite all these advantages, the use of this therapy entails a number of risks that should be known. One of the main complications of abdominal NPT is the development of secondary enterocutaneous fistulas.3 The occurrence of these lesions due to the pressure-aspiration exerted by the system is controversial. However, erroneous placement and application of the NPT system is one of the main factors that lead to the occurrence of these lesions. A common error is the application of the polyurethane sponge in direct contact with the intestinal loops or peritoneum, which causes direct damage to the loops and promotes the development of intestinal fistula. However, the interposition of a non-adherent sheet between the abdominal contents and the sponge protects the intestinal bundle and prevents or greatly minimises the occurrence of this potentially serious complication (Fig. 1). Therefore, as stated in the main worldwide guidelines, the use of abdominal NPT should be coordinated by qualified personnel trained in the specific management of this type of therapy.4,5
FundingThere was no grant support for this manuscript.
