




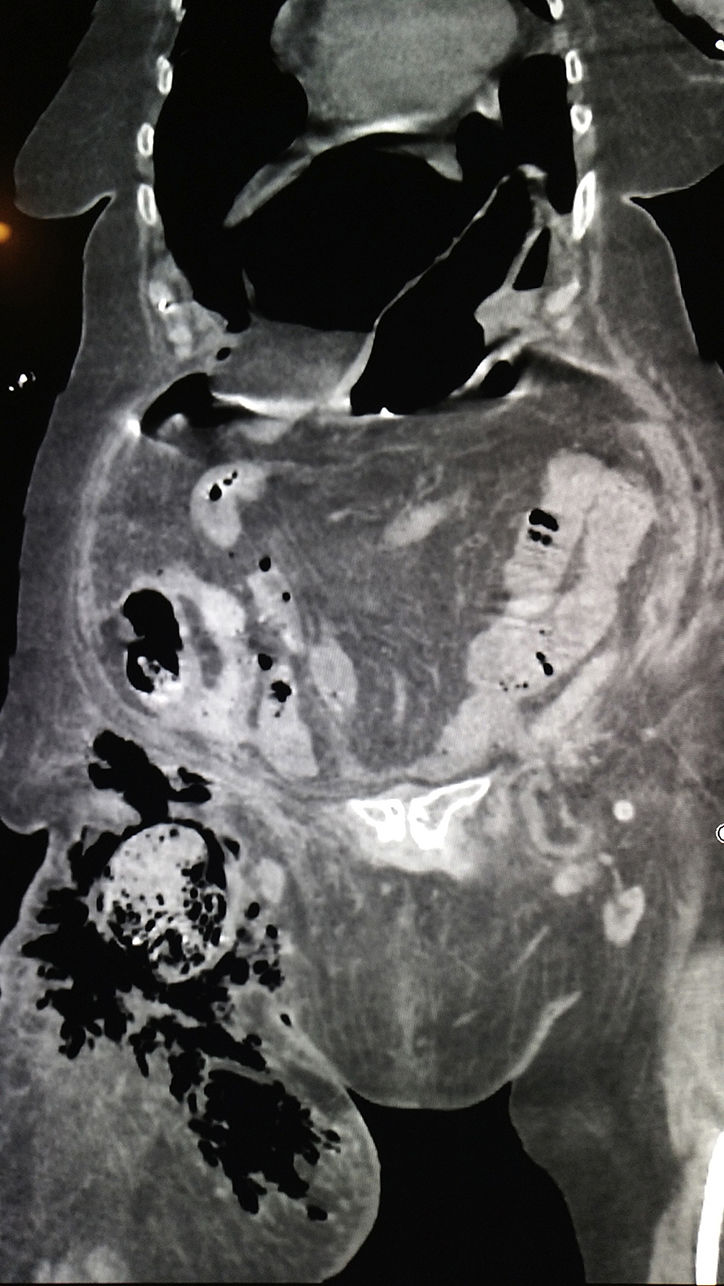

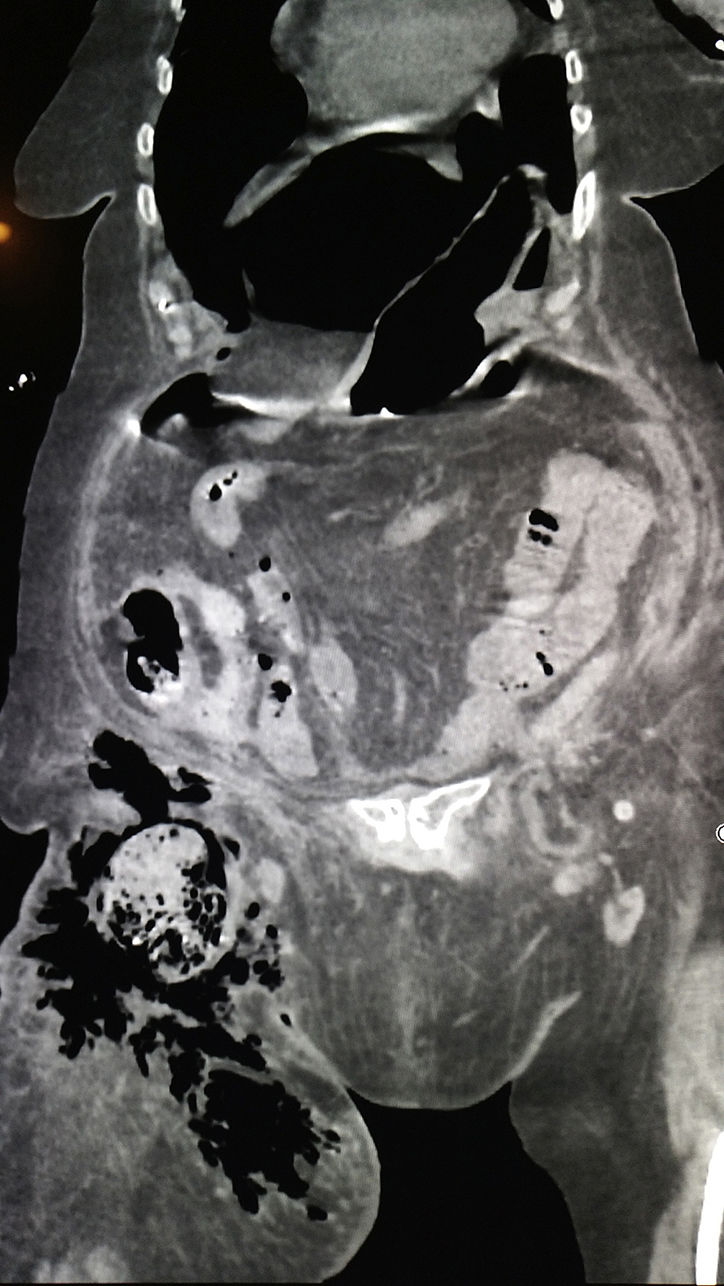
An 82-year-old woman came to the emergency room for cellulitis of the right thigh that had been progressing over the past 12 days and had not responded to treatment with oral amoxicillin-clavulanate. Her medical history included: hypertension, appendectomy, atrial fibrillation treated with rivaroxaban, and right inguinal hernia that had not been treated per the patient's decision. In the emergency department, septic shock was observed with abdominal guarding but no signs of compartment syndrome. Lab work showed: leukocytes 22,500 and C-reactive protein 271mg/L. CT scan detected abundant pneumoperitoneum and the presence of a strangulated right inguinal hernia with intestinal contents, pneumatosis and extraluminal air dissecting the anterior subcutaneous tissue of the right thigh (Figs. 1 and 2). Resuscitation with fluids and broad-spectrum antibiotic therapy were initiated. Emergency surgery revealed a strangulated right inguinal hernia with a necrotic, perforated right colon in its interior. Right hemicolectomy was performed with an ileostomy, mucous fistula and extensive abdominal cavity washing, as well as a debridement of the anterior compartment of the right thigh. The patient presented poor postoperative progress with refractory septic shock and subsequent multiple organ failure on postoperative day 3.

Please cite this article as: Simó Alari F, Durigon G, Molina González E, Gutierrez I. Hernia inguinal perforada con extenso enfisema en el compartimento anterior del muslo. Cir Esp. 2018;96:118.
