






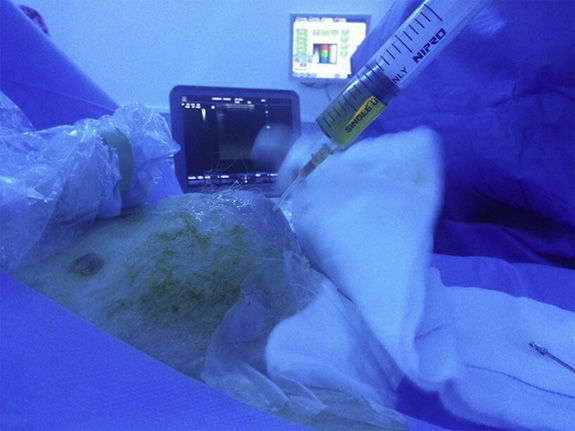
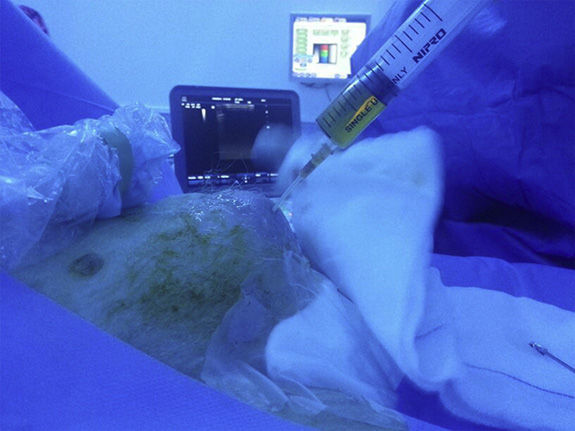
A 76-year-old woman, with a medical history of HTN, stable angina and infrarenal aortic aneurysm, underwent surgery in March 2012 for right endovascular aortoiliac graft and femoro-femoral bypass. She came to our emergency room due to a painful left inguinal mass that had been progressing over the past month, which had grown considerably in the previous 10 days after exertion (Fig. 1). Physical examination showed a painful, non-reducible mass, with no signs of inflammation. Lab workup and abdominal radiography showed no findings of interest. With the diagnostic suspicion of incarcerated crural hernia, an abdominal CT scan was ordered, which revealed a cystic lesion measuring 98mm at its largest diameter that was related with the femoro-femoral bypass. It presented thin walls, no adjacent inflammatory changes, and no contrast extravasation, all of which was suggestive of a seroma (Fig. 2). With this diagnosis, percutaneous drainage was performed and 400cc of clear serous liquid was obtained; cultures were negative (Fig. 3). Progress was satisfactory, and there has been no evidence of recurrence to date.


Diagnosis: perigraft seroma.
Please cite this article as: Romera Barba E, Gálvez Pastor S, Castañer Ramón-Llín J, Vázquez Rojas JL. Seroma periprotésico tras bypass fémoro-femoral. Cir Esp. 2015;93:e15.
