




Lipomas are the most frequent soft tissue tumors, occurring in up to 50% of surgical series. They consist of mature adipocytes that are indistinguishable from normal fat. Occasionally, some lipomas may present morphological variations, including fibrolipomas, which are rare mesenchymal tumor with bands of mature fibrous tissue.1 Although their cellular composition is benign, these lesions sometimes behave as recurrent tumors that are locally aggressive and difficult to manage. In these cases, a strict differential diagnosis with other malignant lipoma diseases is essential. Only one similar case has been described in the literature.2
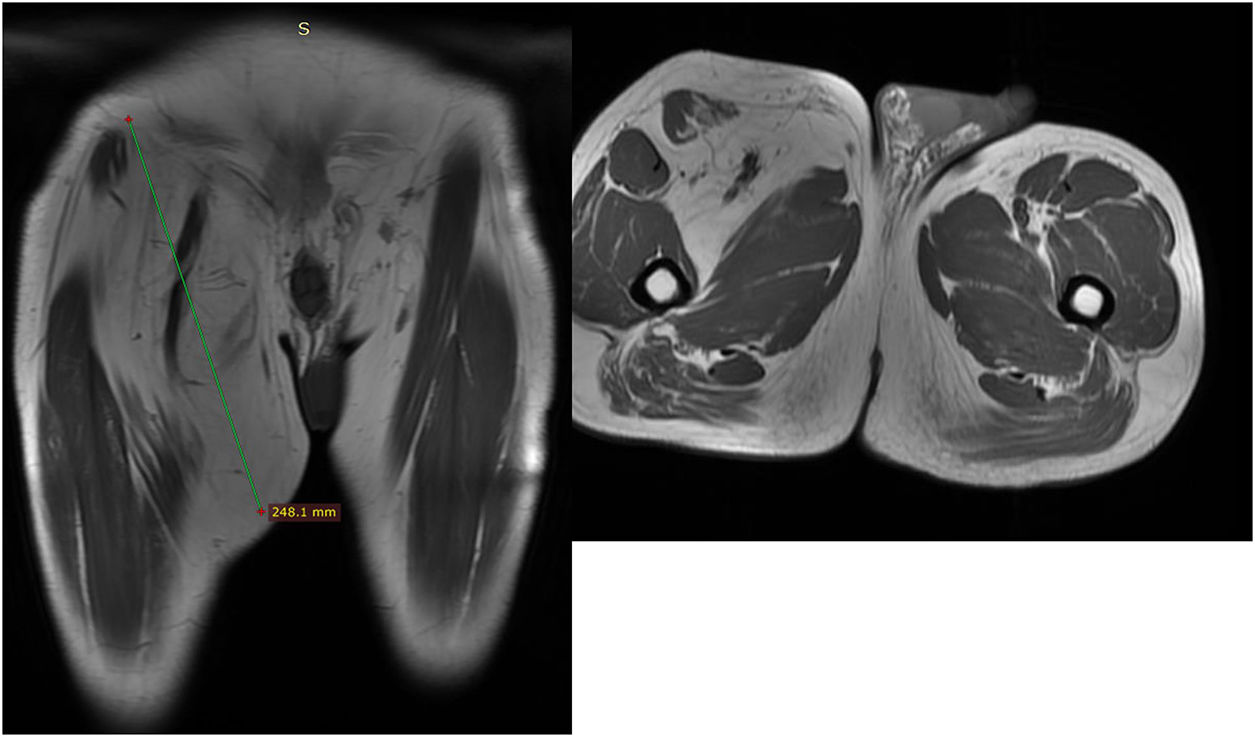
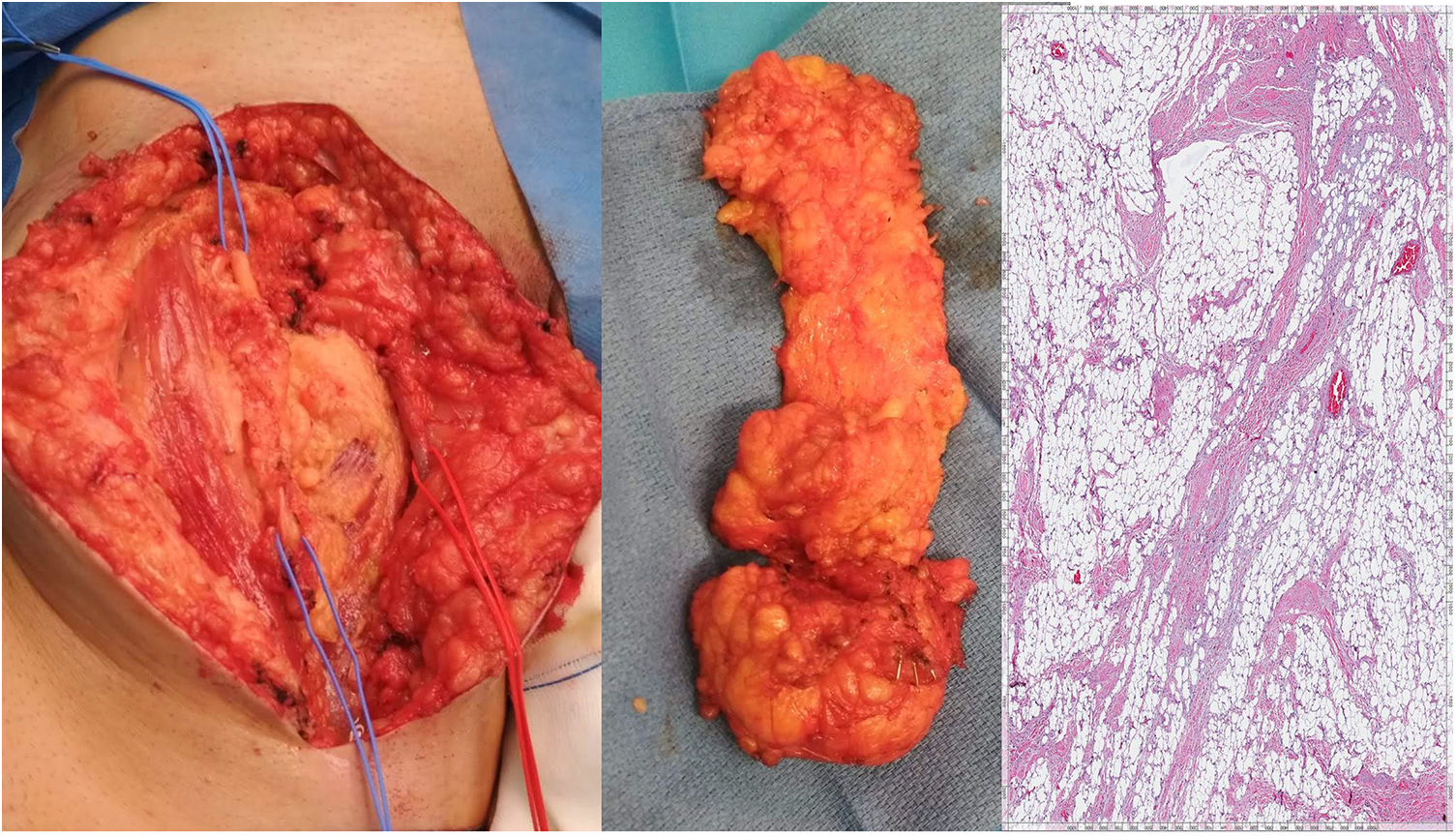
We present the case of a 54-year-old male from Morocco. The patient reported having undergone surgery twice in his home country for a tumor on the inner side of the right thigh 6 and 2 years ago. The patient provided no hospital reports, although he described the lesion as a soft tissue tumor that had reappeared in the last 6 months in the same location as previously, with rapid growth in recent weeks. The lesion caused neuropathic pain in the area, radiating to the lower and anterior leg, as well as impotence. On physical examination, we observed a large soft tissue mass of about 25cm in size that involved the inguinal region and inner side of the right thigh, as well as an 8-cm scar along the tumor from previous surgeries. Lab work was normal. A magnetic resonance imaging (MRI) study of the lower limb demonstrated a large poorly-outlined soft tissue mass measuring 24×6cm with signs of fat and a fibrotic component; the mass extended to the right inguinal region, with no vascular infiltration. These characteristics were all compatible with a possible fibrolipoma (Fig. 1). Surgery was initiated with an oblique incision over the lesion, finding abundant fibrosis due to previous surgeries and a soft tissue tumor measuring 25cm with poorly-defined edges. We dissected the femoral triangle and unaffected femoral vessels, conducting an en bloc excision of the lesion including the affected internal saphenous vein (Fig. 2). Given the possible need for adjuvant radiotherapy, the limits of the tumor were marked with metal clips. The patient presented favorable progress in the postoperative period, requiring a Braun splint for 7 days because of the tension in the surgical area. He was then discharged with no incidents to continue rehabilitation treatment. The pathological study determined the mass to be a giant fibrolipoma (Fig. 2), and the limits of the surgical specimen were thoroughly analyzed by a pathologist specialized in sarcomas, who observed no malignant cells. Six months after surgery, the patient has not presented recurrence of the lesion.

; histology study showing the adipocytes with bands of fibrous tissue running through them (H–E 20×).")
Giant lipomas are defined as being larger than 10cm in size or weighing more than 1000g. They typically have slow, painless growth and are easily resectable3; however, there are morphological variations (such as in this case) in which the clinical scenario becomes more complex. These variations include fibrolipoma, in which prominent bands of mature fibrous tissue invade normal adipocytes. Other subtypes include myxolipoma, chondrolipoma, myolipoma, angiolipoma, etc.4 The etiology of lipomatous lesions is unclear and may involve metabolic endocrine, genetic or trauma factors.2 When these large and transformed lipomatous lesions are located in a lower extremity, they can cause compression-related symptoms (lymphedema, neuropathic pain, compression syndromes, etc.). Although only one case of giant fibrolipoma has been described in this location (most are located in the trunk and upper limbs), the symptoms were similar to those of our patient,2 which could lead us to think of a more aggressive local behavior related to the greater fibrous component.3–5 The diagnosis is established by clinical examination, with complementary MRI studies to assess the relationship with deep structures as well as biopsy in selected cases. The treatment of choice is complete resection of the lesion.7 The recurrence rate after excision of a giant lipoma is 14% and is associated with incomplete excision,2–6 although in the case of a fibrolipoma these rates may be much higher given the difficulty to determine the extension of the lesion on occasion, as in our case, which makes postoperative patient follow-up necessary.8 These large tumors also have a higher risk of malignant transformation (liposarcoma), so early excision of the tumor is essential, especially when larger than 10cm or with rapid growth.9 When faced with a recurrent fibrolipoma of atypical, aggressive behavior, as is our case, other options to be considered are extended resection, including the Sartorius muscle, pectineal muscle, saphenous vein and fascia of Scarpa, as well as a deep dissection of the femoral neurovascular bundle. Adjuvant radiotherapy, which has provided favorable results in the case of soft tissue sarcomas, could also be an option to assess in these cases, although always provided there is consensus of a multidisciplinary team and the patient.10
There are isolated cases in the literature that describe the behavior of these fibrous mesenchymal neoplasms. In case of suspicion of this type of tumors, the surgical indication must be determined as early as possible, the excision should be thorough and complete, the follow-up should be cautious, and the case should be overseen by a multidisciplinary team. Future research at the cellular and subcellular level will determine the pathophysiological mechanisms underlying the progress of this type of lipomas.
Please cite this article as: Abellán I, Molina M, Bernabé A, González P. Fibrolipoma gigante recidivado: una enfermedad de difícil manejo. Cir Esp. 2019;97:544–546.
