





Soft tissue sarcomas (STS) are non-epithelial malignant tumors of the extraskeletal tissue that can compromise the muscles, fat, fibrous tissue, blood vessels or other supporting tissues of the body. Treatment has changed from ablative procedures to more conservative surgical treatments.1 Resective surgery that may or may not be associated with adjuvant therapy is the standard treatment, and amputation is only considered when it is not possible to obtain wide margins or achieve functional reconstruction of the limb.2
The thigh is the most frequent location of sarcomas of the legs. Resection of this type of tumors requires wide margins, and the large secondary defects do not usually close directly, or they are obtained with tension. These resulting defects are usually deep and frequently expose the femoral vessels. The resulting dead space is usually greater than in more distal resections and, in this region, the wounds usually have a higher percentage of dehiscence and infections. For this reason, reconstruction of this region requires sufficient tissue to fill the dead space, protect the femoral vessels and avoid closure with tension.3,4 Furthermore, radiation makes proper wound healing more difficult.
Vertical rectus abdominis myocutaneous (VRAM) flaps have been successfully used for the coverage of defects in the rib cage wall as well as the inguinal, perineal, vaginal and gluteus regions with good aesthetic and functional results. The advantage of the pedicled VRAM flap is that it provides an extensive cutaneous island, great thickness of soft tissue with an easily executable surgical technique, low rate of complications and high probability for success.5
We present 2 case reports of patients with STS in the thigh who underwent radical resection and reconstruction with VRAM flaps.
Case 1The patient is a 63-year-old male who presented a mass in the left thigh that had been developing over the previous 3 months and was accompanied by pain and progressive growth. Upon examination, the tumor measured 10×10cm and was located on the side of the left thigh.
MRI demonstrated a multilobular mass on the anterior side of the upper third of the thigh that measured 15.5×7.5×5cm in the vastus lateralis. It was in contact with the bone and, located between it, the vastus intermedius, rectus femoris and the tensor fasciae latae, which were being compressed and displaced. The extension study found no data suggestive of malignancy.
FNA and Trucut biopsy of the mass provided positive cytology results for malignant cells and findings suggestive of pleomorphic sarcoma.
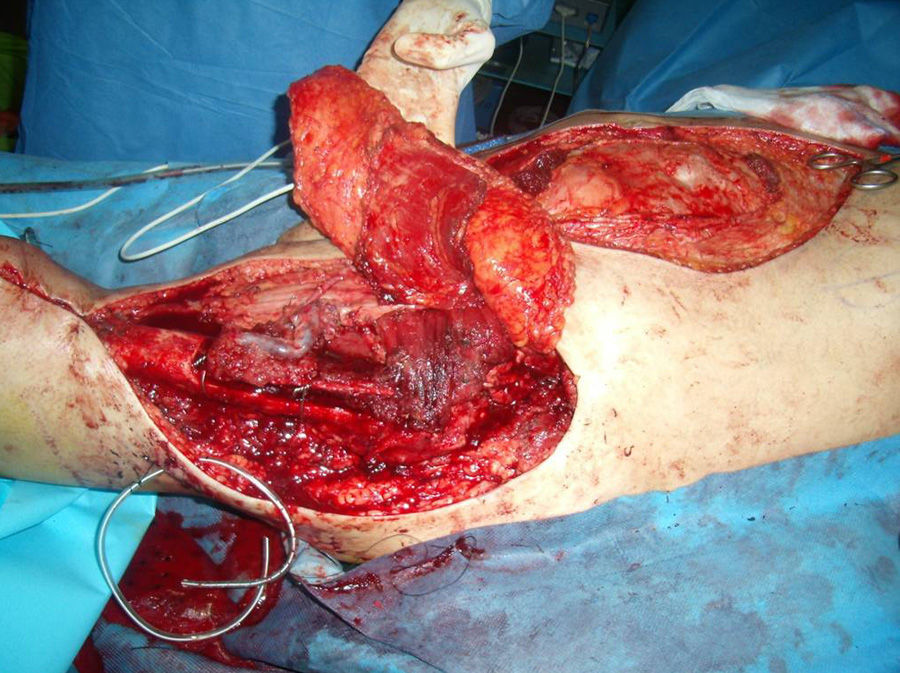
The patient underwent radical surgical resection with margins of the anterior compartment of the left thigh and anterior cortical of the femur. Bone reconstruction was performed using a free fibula flap with end-to-end anastomosis of the fibular pedicle to a branch of the superficial femoral package (1 artery and 2 veins). Coverage was created with a pedicled VRAM flap with the inferior epigastric vessels (Fig. 1).

Follow-up MRI done 2 years later showed no evidence of signal alterations in the bone. No differences were observed between the two femoral heads, with preserved morphology of the signal intensity and no signs of dysplasia, osteonecrosis or vascular necrosis.
Case 2A 72-year-old male presented with a mass on the anterolateral right thigh with FNA suggestive of STS. Upon examination, a mass was observed that was approximately 10cm in the proximal third of the anterolateral right thigh.
MRI reported the presence of a mass measuring 7.2×4.9×5.2cm in the middle of the vastus intermedius/lateralis and tensor fasciae latae of the right thigh with marked partial infiltration of these structures. The extension study found no data suggestive of distant metastasis.
The patient underwent radical resection of the mass, including the sartorius muscle, rectus femoris and vastus intermedius and lateralis of the quadriceps, using the coverage of a pedicled VRAM flap with preservation of the abdominal fascia, except a small ellipse that included the deep inferior epigastric artery perforators that vascularized the flap (Fig. 2).

The flaps evolved satisfactorily without requiring revision in either of the 2 cases. The patients were followed up weekly until wound healing was optimal before starting to walk. In both cases, the patients had a favorable recovery. To date, there has been no evidence of local recurrence or distant metastasis.
VRAM flaps are very useful for covering inguinal-femoral defects. They provide a large amount of tissue, are very versatile for design and rotation, do not require changes in patient position and present low abdominal wall morbidity.6
In the second case reported, the use of a dominant perforator vessel favored the reduction in morbidity in the donor zone by preserving practically all the abdominal fascia and avoiding hernias, incisional hernias or myofascial laxity, which are possible consequences of the donor area of this type of flaps.7
Please cite this article as: Sánchez Medina MT, Lima Sánchez J, Fernández-Palacios J, García Duque O. Sarcoma de partes blandas en muslo e ingle. Reconstrucción con colgajo miocutáneo vertical de rectus abdominis. Cir Esp. 2014;92:693–694.
