






The main cause of mortality in trauma patients with pelvic fractures is hypovolemic shock. We analysed the association between the source of bleeding, mechanism of action and type of fracture.
MethodsProspective descriptive study involving trauma patients older than 16 years old, admitted to the intensive care unit or dead before admission, with pelvic fractures and hemodynamic instability. Hemodynamic instability was defined as SBP <90 and/or HR >100beats/min. Pelvic fracture was defined by the Tile classification.
ResultsA total of 157 of 1088 trauma patients had pelvic fracture. We included 63 patients, all hemodynamically unstable. A total of 85% of pelvic fractures after falls from great heights bled from the fracture itself, compared to only 44% of victims of the impact (hit). A total of 65% of patients with stable pelvic fracture bled from associated lesions; 70% of patients with unstable fracture bled from the fracture itself. There is an interaction between the mechanism of action and type of fracture. The probability of pelvic bleeding is higher in the precipitated patient (>80%) regardless of the type of fracture. Bleeding from associated injuries is greater in impact victims, doubling when the fracture is stable (91%).
ConclusionsMechanism of action is a key to determine the source of bleeding in patients with pelvic fracture. After falls patients bleed from the fracture itself, while patients with an impact (hit) can bleed both from the fracture and associated injuries, depending on the type of fracture.
La principal causa de mortalidad en los politraumatizados con fracturas pélvicas es el shock hipovolémico. Analizamos la asociación entre el origen de la hemorragia, mecanismo de acción y tipo de fractura.
MétodosEstudio descriptivo y prospectivo que incluye a pacientes politraumatizados mayores de 16 años, ingresados en el área de críticos o que han fallecido antes de su ingreso, con fractura pélvica e inestabilidad hemodinámica. Se define inestabilidad hemodinámica como PAS<90 o FC>100 latidos/min. La fractura pélvica se define según la clasificación de Tile.
ResultadosUn total de 157 de 1.088 politraumatizados tenían fractura pélvica. Se ha incluido a 63 pacientes, todos hemodinámicamente inestables. En el 85% de los pacientes precipitados la hemorragia procedía de la propia fractura pélvica, comparado con solo el 44% de las víctimas que sufrieron un (choque). El 65% de los pacientes con fractura de pelvis estable sangraban de lesiones asociadas; el 70% de los pacientes con fractura inestable sangraban de la propia fractura. Existe una interacción entre el mecanismo de acción y el tipo de fractura. La probabilidad de sangrar de la pelvis es mayor en los precipitados (> 80%), independientemente del tipo de fractura. La hemorragia de las lesiones asociadas es mayor en un impacto, duplicándose cuando la fractura es estable (91%).
ConclusionesEl mecanismo de acción es un factor clave para determinar el origen de la hemorragia en pacientes con fractura de pelvis. Los pacientes precipitados sangran de la propia fractura, mientras que los pacientes con un impacto (choque) pueden sangrar tanto de la propia fractura como de las lesiones asociadas, dependiendo del tipo de fractura.
Polytrauma patients with pelvic fractures have sustained high-energy injuries. The energy required to cause such an injury means that these multiple-trauma patients also have a high risk of morbidity and mortality as well as a high rate of associated injuries.1
The main cause of mortality in polytrauma patients with pelvic fractures is hypovolemic shock.2,3 In these patients, the principal source of hypovolemia is the pelvic fracture itself, which is the main cause of the haemorrhage in 60% of cases; in the remaining 40%, the patients present hypovolemic shock due to associated injuries.3 It is essential to detect and treat hypovolemia as rapidly as possible because mortality increases by 1% for every 3min of haemodynamic instability,4 regardless of the cause of the hypovolemic shock. It is therefore necessary to identify and treat the pelvic fracture and determine any possible associated lesions that could be the origin of the haemorrhage.
In polytrauma patients, the main lesions associated with pelvic fractures are abdominal, genitourinary, thoracic and head injuries.3,5,6 Between 4% and 23% of abdominal injuries are associated with pelvic fractures. We would like to emphasise the importance of having a high degree of suspicion for their diagnosis.7
There is much controversy about the risk factors that can help predict the bleeding origin, the most widely accepted of which are the mechanism of injury and the fracture type.
Some authors6,7 defend that the origin of the haemorrhage depends on the mechanism of injury causing the fracture: if the mechanism is a fall, the haemorrhage probably originated from the pelvic fracture6; meanwhile, if the mechanism is an impact (crash) then the associated injuries probably caused the haemorrhage.7 Other authors, however, have not been able to clearly establish this correlation.8
Furthermore, some authors have identified a more severe type of pelvic fracture (AIS≥4, requiring blood transfusion or resulting in death). These patients have a greater risk of presenting associated abdominal injuries, with a greater risk of haemorrhage from these injuries as well as the pelvis itself.5,9
The hypothesis of this study is that the mechanism of injury, either a fall or impact (crash), predicts the cause of bleeding in haemodynamically unstable polytrauma patients with pelvic fracture.
The objective of this study is to study the possible association between the origin of the haemorrhage and the mechanism of injury, while correlating the type of fracture and origin of the haemorrhage.
Material and MethodsThe following is an observational study using a prospective database from Hospital Universitari Parc Taulí between March 2006 and December 2013.
Included for the study were all those polytrauma patients admitted to the critical care unit or that had died before hospitalisation, presented pelvic fractures and were haemodynamically unstable.
Excluded from the study were multiple-trauma patients under the age of 16 and those whose injuries were due to a penetrating mechanism of injury.
Haemodynamic instability is defined as systolic blood pressure <90mmHg or heart rate >100bpm.1
Pelvic fractures were classified in accordance with the Tile classification.10 Type A pelvic fractures were considered stable, and types B and C were considered unstable pelvic fractures.
The following variables were registered prospectively in an Access®-protected database: demographic data for each patient, mechanism of injury, blood pressure, heart rate, respiratory frequency, oxygen saturation, temperature, Glasgow coma scale,11 Injury Severity Score (ISS),12 complimentary studies (simple radiograph, FAST ultrasound, computed tomography, arteriography, etc.) and the time they were completed (primary, secondary or tertiary studies), associated injuries, type of pelvic fracture, treatment of each injury, complications and resolution of each case (specifying cause of death in cases of death).
The origin of the haemorrhage was determined by a group of experts who analysed each case based on the complementary tests done and the clinical responses to the different therapies.
Statistical AnalysisCategorical variables are described as percentages, and the continuous variables are reported as mean and standard deviation.
The variables for mechanism of injury and fracture type were considered binary categories. A univariate analysis was done with the chi-squared test between these variables and the dependent variable origin of bleeding by means of Fischer's exact test. Logistic regression was used with the variables mechanism of injury and fracture type as well as the interaction variable mechanism of injury due to fracture type. Hierarchical modelling13 was used according to Hosmer–Lemeshow. The interaction variable remained in the final equation if it was found to be statistically significant. A P<.05 was considered statistically significant.
ResultsFrom March 2006 until December 2013, we prospectively registered 1088 multiple-trauma patients over the age of 16 who had been admitted to the critical care unit or had died before hospitalisation.
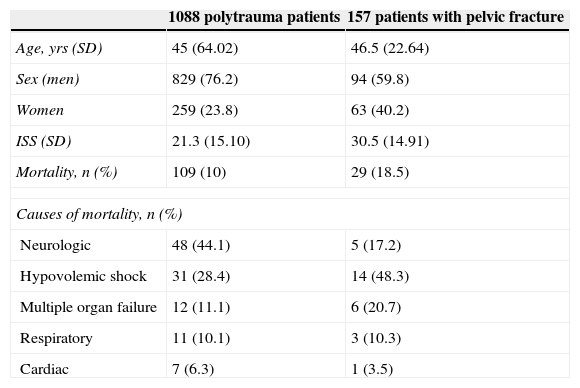
Out of the patients registered, 157 (14.4%) presented pelvic fractures due to blunt trauma. The mean ISS of the registered polytrauma patients with pelvic fractures was higher than the overall series (30.5 vs 21.3). The mortality rate of patients with pelvic fractures was 18.5%, and hypovolemic shock was the main cause of death in 48.3% of cases (Table 1).
Demographic Data.
| 1088 polytrauma patients | 157 patients with pelvic fracture | |
|---|---|---|
| Age, yrs (SD) | 45 (64.02) | 46.5 (22.64) |
| Sex (men) | 829 (76.2) | 94 (59.8) |
| Women | 259 (23.8) | 63 (40.2) |
| ISS (SD) | 21.3 (15.10) | 30.5 (14.91) |
| Mortality, n (%) | 109 (10) | 29 (18.5) |
| Causes of mortality, n (%) | ||
| Neurologic | 48 (44.1) | 5 (17.2) |
| Hypovolemic shock | 31 (28.4) | 14 (48.3) |
| Multiple organ failure | 12 (11.1) | 6 (20.7) |
| Respiratory | 11 (10.1) | 3 (10.3) |
| Cardiac | 7 (6.3) | 1 (3.5) |
Out of the 157 polytrauma patients with pelvic fractures, 94 were haemodynamically stable at the time of hospitalisation and 63 were haemodynamically unstable. The patients included in the study were the 63 multiple-trauma patients with pelvic fracture who were haemodynamically unstable.
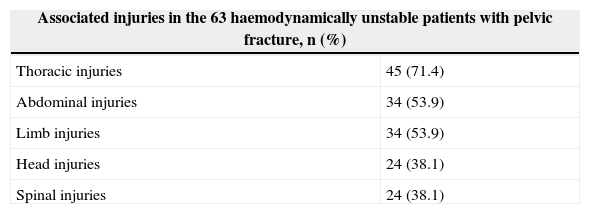
A total of 61 (96.8%) patients out of the 63 haemodynamically unstable multiple-trauma patients with pelvic fracture presented associated lesions. These associated injuries were mainly thoracic, followed by abdominal or extremity injuries (Table 2).
By analysing the origin of the haemorrhage in this group of patients and classifying them according to the mechanism of injury of the trauma (either a fall or impact/crash), we detected that 85% of the patients who had fallen bled from the fracture itself, while only 44% of the patients who had sustained an impact (crash) bled from the fracture. In these patients, the origin of the haemorrhage is secondary to the associated lesions (56% of cases) (Fig. 1).

Through this process of analysing the origin of the haemorrhage in haemodynamically unstable polytrauma patients with pelvic fractures, classifying them according to fracture type and as either stable (Tile type A) or unstable (Tile types B and C), we detected that 65% (11 cases) of the patients who presented stable pelvic fracture bled from the associated injuries and only bled from the pelvis itself in 35% of cases (6 patients). In contrast, patients who presented unstable pelvic fractures bled mainly from the pelvic fracture itself in 70% of cases (32 cases) (Fig. 2).

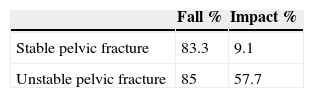
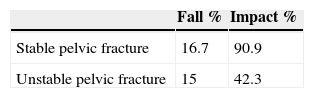
By means of logistic regression, we have detected an interaction between the mechanism of injury and fracture type. When the logistic regression formula was applied, Tables 3 and 4 were created. As the factors mechanism of injury and fracture type presented an interaction, we should contemplate both in order to predict the origin of the bleeding. In Table 3, we can observe that the probability of pelvic bleeding was greater in patients who had sustained a fall (>80%), regardless of the type of fracture. Meanwhile, in Table 4 we observed that, although the probability of haemorrhage through the associated injuries is greater in patients who have withstood an impact (crash), this probability doubles when the pelvic fracture is stable (91%). Patients who have been injured by impact and have an unstable pelvic fracture can bleed from the pelvis itself (57.7%) as well as the associated lesions (42.3%).
Our study concurs with the literature1 as we have detected that polytrauma patients with pelvic fractures have a more serious condition (ISS 30.5 vs 21.3) and higher associated mortality than polytrauma patients without this type of injury. The mortality rate for this type of patients in our series is 18.5%, which coincides with the literature.
In our experience, the main cause of death in patients with pelvic fractures is hypovolemic shock, which also coincides with most authors.2,3
Scalea et al.6 reported that 80% of haemodynamically unstable multiple-trauma (fall) patients bled from the pelvic fracture itself and from the associated retroperitoneal haematoma. In addition, Murr et al.7 wrote that all polytrauma patients with haemodynamically unstable pelvic fractures and an impact mechanism of injury bleed from the associated abdominal injuries. In our study, haemodynamically unstable multiple-trauma patients who had been injured by a fall also mainly bled from the pelvic fracture itself (85%), although haemodynamically unstable multiple-trauma patients with an impact mechanism of injury (crash) bled from the associated lesions (56%) as well as from the pelvic fracture itself (44%). Therefore, defining the mechanism of injury in a haemodynamically unstable patient with pelvic fracture can help determine and quickly treat the origin of the haemorrhage.
Demetriades et al.5 and Bond et al.9 reported a higher risk of haemorrhage due to associated injuries with more severe pelvic fractures. In our study, the type of pelvic fracture influenced the origin of the haemorrhage, although these findings are contrary to previous publications. Patients with stable pelvic fractures bled more from the associated lesions (65%), while the patients with unstable pelvic fractures bled more from the fracture itself (70%).
The results published by Demetriades et al. can be justified by the fact that more severe pelvic fractures are associated with multiple trauma caused by high-energy mechanisms of injury that in turn cause severe and potentially haemorrhagic associated injuries. Our results were based on a group of haemodynamically unstable patients. Thus, in patients with stable pelvic fractures, associated injuries are more likely to cause hypovolemic shock than the fractures themselves, while unstable pelvic fractures are able to cause sufficient bleeding to cause shock.
By analysing the mechanism of injury and pelvic fracture type, we observed that both factors interact; therefore, they must be considered in conjunction to predict the probability of the origin of the haemorrhage. For now, we do not know of any relevant publication describing this interaction. In our study, the patients who had sustained a fall showed a probability of more than 80% for bleeding from the pelvic fracture itself, regardless of the type of fracture. When we analysed the patients who had withstood an impact mechanism of injury (crash), we were able to observe that, in cases of stable pelvic fracture, the haemorrhage originated in associated injuries (91%). Meanwhile, patients with unstable pelvic fractures had bleeding from either the associated lesions (42.3%) or the pelvis itself (57.7%).
The strength of our study lies in the fact that it is based on a prospective patient register at a hospital with experience in the polytrauma patient care and medical training, involving an important number of severe polytrauma cases. Furthermore, the study is clinically applicable to any type of hospital centre that treats multiple-trauma patients. The main weakness is its sample size, which we would have liked to have been larger in order to draw stronger conclusions.
We are therefore able to conclude that the mechanism of injury is essential for suspecting the origin of the haemorrhage. Patients who have had a fall bleed from the pelvic fracture itself, while patients who have been injured by impact (crash) may bleed from the fracture as well as the associated injuries. After an impact (crash), this probability is influenced by the type of pelvic fracture.
Conflict of InterestsThe authors have no conflict of interests to declare.
Please cite this article as: Montmany S, Rebasa P, Luna A, Hidalgo JM, Cánovas G, Navarro S. Origen de la hemorragia en pacientes politraumatizados con fractura de pelvis e inestabilidad hemodinámica. Cir Esp. 2015;93:450–454.
