








Today's clinical psychology advocates for empirically validated treatments. This supports the need for outcome-driven research, but may overlook the importance of process-driven research, which can respond to the question of why psychological treatments work. Functional analysis of behaviour has received a new boost with the emergence of the third wave of psychological therapies, which stress the importance of verbal behaviour in therapy as a way to access and modify client problems. The case presented in this work was analysed in order to make an approach to the strengthening processes that take place in therapy through verbal interaction. First, we developed and applied a categorization system of client's adaptive verbalizations. We found that this type of verbalizations increase significantly after the first few sessions, remain high in the middle sessions, and gradually decrease towards the end of the therapy. We subsequently developed and used a system of categorization of therapist's verbal behaviour. We found that agreeable verbalizations were concentrated in the middle sessions, being replaced by other verbalizations in the final sessions.
La psicología clínica actual es partidaria de los tratamientos validados empíricamente, lo cual invoca la necesidad de una investigación guiada por los resultados, si bien puede soslayar la importancia de la investigación quiada por los procesos, que puede responder a la pregunta de por qué funcionan los tratamientos psicológicos. El análisis funcional de la conducta ha recibido un nuevo impulso con la emergencia de la tercera ola de terapias psicológicas, que destaca la importancia del comportamiento verbal en la terapia como una manera de acceder a los problemas del cliente y modificarlos. El caso que se presenta en este trabajo nos permitirá acercarnos a los procesos reforzadores que tienen lugar en la terapia debidos a la interacción verbal. En primer lugar hemos desarrollado y aplicado un sistema de caracterización de las verbalizaciones adaptativas del cliente. Observamos que este tipo de verbalizaciones aumenta significativamente transcurridas las primeras sesiones, se mantiene elevado en las sesiones intermedias y disminuye paulatinamente hacia el final de la terapia. Posteriormente elaboramos y utilizamos un sistema de categorización del comportamiento verbal del terapeuta, observando que las verbalizaciones se concentraban en las sesiones intermedias y eran sustituidas por otras verbalizaciones en las sesiones finales.
From the very beginning, the study of clinical cases has been considered as an essential tool in psychotherapy research. In fact, the development of large psychotherapeutic approaches began with the study of cases, some of which have become widely known inside and outside of the world of research (Ana O. or little Albert cases are probably the most famous in the history of psychotherapy). This methodology's intrinsic characteristics, especially its ideographic nature and its ability to show the dynamic of changes that occur over time, make it particularly suitable for both outcome-driven and process-driven clinical research. This study is part of the latter type of clinical research as our objective is to clarify the mechanisms that underlie and explain the clinical change. To do this, we have opted for the “moment-by-moment” study of the therapeutic process from a functional-analytical perspective and through observational analysis. Our ACOVEO research team of the Universidad Autónoma de Madrid has been working and refining this research methodology for almost a decade with interesting findings, some of which were published in articles of this journal (Froján-Parga, Montaño-Fidalgo, Calero-Elvira, & Ruiz-Sancho, 2011; Marchena-Giráldez, Calero-Elvira, & Galván-Domínguez, 2013; Montaño-Fidalgo, Froján-Parga, Ruiz-Sancho, & Virués-Ortega, 2011).
Throughout these years, our efforts have been focused on the study of verbal interaction between therapist and client during the therapeutic process. We start from a conception of the clinical situation as a natural context in which client's problems are presented in the same way as in any other aspect of his life. At the same time, we conceive verbal behaviour carried out in therapy as a clinically relevant behaviour (CRB), in the same way as conceived by the Functional Analytic Psychotherapy (FAP; Kohlenberg & Tsai, 1995). We also share with the FAP its postulates about behaviour-behaviour relationships and the say-do correspondence, according to which the human being is capable of establishing a relationship of correspondence between what is said and done (Baer, Detrich, & Weninger, 1988; Israel & O’Leary, 1973). It is therefore possible to influence client's actions through the verbal report of such actions and vice versa. It is worth spending some time focusing on these aspects, as they are essential when it comes to contextualising our case study both theoretically and methodologically. One of the key features of the so called contextual therapies or third generation therapies – amongst which we find the previously mentioned Functional Analytic Psychotherapy – is their interest in verbal behaviour and how it relates to clients’ problems, therapists’ activities and the clinical change. We cannot forget that psychological therapy is essentially oral and that the main activity carried our by client and therapist during a session is, precisely, speaking. In this sense, what both individuals say has a fundamental relevance in multiple aspects affecting the development of the therapy. Concerning the client, his verbal behaviour is not limited to being a mere channel of transmission of information on his problems or progress, but what he says becomes part of the problem and progress. In virtually all cases, part of the problem that brings clients to therapy lies precisely in the kind of things being said about his situation, about himself, others or about life in general. For this reason, client's verbal behaviour in session is considered a clinically relevant behaviour (Kohlenberg & Tsai, 1991) that needs therapist's attention and on which therapist must influence as part of the treatment. Thus, the client's language goes from being considered a simple communication channel with no other function than to allow the exchange of information, to being regarded as a fundamental goal of therapy. In this sense, a great portion of the therapist's job is to modify the client's speech, facilitating the development of a more adaptive verbal repertoire. The main tool that the therapist has to achieve this is precisely his own verbal behaviour. The therapist uses the language to shape client's behaviour, favouring the acquisition and development of more adaptive behaviour, both verbal and nonverbal, and both inside and outside of therapy. The power of therapist's verbal behaviour is not limited to the immediate context of session. It also goes beyond this context, extending to all other aspects of the client's life through the say-do correspondence mentioned before. The notion of say-do correspondence refers to the capacity that human beings have to establish functional equivalence relationships between words we use and their referents in reality and, more specifically, our ability to establish relationships of functional correspondence between what we do and what we say we do. The words we use acquire the same functions as the realities to which they refer, so that it is possible to influence our behaviour by focusing on the verbal description we make of it, just as if we were acting directly on such conduct. Focusing on the therapeutic context, clients establish a functional correspondence relationship between their behaviour outside the clinic and the story they tell of such conduct in the clinic. The therapist can use this correspondence relationship to influence on behaviours carried out outside of session by acting on the verbal report that the client makes of them. Thus, the therapist can discriminate, reinforce, or punish the client's behaviour, even if it happens outside of the clinic, thanks to the verbal description that the client does of such behaviour (Galván-Domínguez, Beggio, Pardo-Cebrián, Segovia-Arroyo, & Froján-Parga, 2014).
We can find the origins of these concepts in Skinner's (1957) book Verbal Behaviour, in which the acclaimed author uses the principles of operant conditioning to explain the acquisition of language as another behaviour. Besides giving rise to heated debates, this work has given rise to several lines of research concerned with language from a behavioural perspective, among which we find the studies on stimuli equivalence (Sidman & Tailby, 1982) and the Relational Frame Theory (Barnes-Holmes, Hayes, & Roche, 2001). The concept of equivalence relationship refers to the rise of an association between two elements with no previous exposure or training in such association. Sidman (1971) initially describes this phenomenon with the matching to sample procedure. Under this procedure, after training in discrimination of two relationships separately (e.g., A-B and A-C), new discriminations can flourish (e.g., B-A, C-A, B-C and C-B) with elements that have not appeared in conjunction before (Valero-Aguayo & Luciano-Soriano, 1992). Symbolic behaviour in general and language in particular would therefore be explained by the development of such equivalence relationships between symbols (words) and reality (referents). Applied to the field of behaviour, when a functional equivalence relationship between a word and a referent is established, the word acquires its properties and can influence the behaviour of the subject in the same way that the reference. The Relational Frame Theory (RFT) collects and expands Skinner's principles (Barnes-Holmes, Barnes-Holmes, & Cullinan, 2000), and presents criticisms to several aspects of the stimuli equivalence stream. The RFT proposes that relational learning can be considered a generalized operant characterized by the development of relationships established or derived from stimuli. These relationships would not be based on the formal properties of the stimuli, but on contextual cues that indicate what kind of relationship is applicable given a history of reinforcement with multiples examples of such cues (Gómez-Martín, López-Ríos, & Mesa-Manjón, 2007). In this sense, the language would arise mainly from the establishment of derived relationships, which are those between stimuli acquired with no previous training. From this standpoint, these relationships are considered generalized operants applied arbitrarily, that is, relationships that are not subject to the physical properties of stimuli, but are established by the verbal community to which the subject belongs and which can modify these relationships. The RFT has served as the basis for the development of one of the most famous contextual therapies: the Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999).
In short, the therapeutic situation takes place in a unique context where verbal behaviour is the main instrument to establish reinforcement and punishment contingencies over the behaviours object of treatment (Froján, 2011). In this sense, as stated by Froján (2011), what the psychologist does in therapy is initiate a series of learning processes that will lead to more adaptive behaviours by the client and that will occur mainly through verbal interaction that occurs during therapy. Thus, we understand that the in-depth analysis of the clinical phenomenon should consider studying verbal interaction between therapist and client (Froján-Parga et al., 2011) and that the functional-analytical perspective is best-suited to carry out this study. Based on these considerations, our research group has focused on the development and application of various categorization systems of verbal behaviour in therapy. These systems have allowed us to analyse the characteristics and dynamics of the therapist and client verbalizations, and the relationships that take place between both along intervention (Froján, Pardo, Vargas, & Linares, 2011; Marchena-Giráldez et al., 2013; Ruiz-Sancho, Froján-Parga, & Galván-Domínguez, 2015). Currently, the team counts with an incipient line of research covering the punitive process in therapy with a preliminary case study approach to the relationship between maladaptive client verbalizations and the therapist's response (Froján Parga, Galván Domínguez, Izquierdo Alfaro, Ruiz Sancho, & Marchena Giráldez, 2013). The aim of this work is to make a similar approach to the process of verbal reinforcement in therapy, focusing on the analysis of the dynamics of the client's adaptive verbalizations during therapy and how such verbalizations relate to the therapist's verbalizations. We start with two premises: (1) the increase in adaptive verbalizations expressed by the client is one of the basic objectives of the therapist, and (2) certain therapist verbalizations can have a significant reinforcement value to the client. It is worth mentioning that we have considered as adaptive all client verbalizations that, linked to the problem areas exposed during the case formulation, suppose an approach to the therapeutic goals. Such adaptive verbalization will take the form of: (1) anticipation or description of the realization of the tasks proposed by the therapist; (2) anticipation or description of the achievement of the objectives; and (3) the interpretations about the client's own behaviour and beliefs about what the causes of such behaviour are in functionally successful terms from the psychological standpoint – in line with the type 3 CRB proposed by the Functional Analytic Psychotherapy (Parra & García, 2006).
We have analysed a complete clinical case, beginning with the client's verbal behaviour. From such analysis, we built a categorization system of the client's adaptive verbalizations. This allowed us to analyse the dynamics during therapy. We then analysed the therapist's verbalizations that took place immediately after the client's adaptive verbalizations, resulting in another categorization system of the therapist's verbal behaviour. Such system allowed us to analyse the evolution of the therapist's verbalizations and its relationship with the client's adaptive verbalizations. This facilitated an approach to the type of verbalizations that could be considered reinforcing with higher probability. In line with previous studies carried out by the team about the distribution of the therapist and client verbalizations in the therapeutic process (Froján-Parga et al., 2011; Ruiz-Sancho, Froján-Parga, & Calero-Elvira, 2013), we expect to find that the frequency and duration of the client's adaptive verbalizations are low during the initial sessions – when the therapist's objective is primarily evaluate and explain becoming more apparent during the therapist's treat phase, and progressively decreasing when the therapist's main objective is consolidate the client's change.
MethodParticipantsWe analysed the clinical case of X., composed of 13 clinical sessions of approximately one-hour length. The intervention was conducted by an expert therapist with more than 15 years of clinical experience in ITEMA, a private centre specialised in Cognitive Behavioural Therapy.
X., a 29 year-old Spanish woman, a market analyst, sought therapy because of a low state of mind that, according to her, she had had ‘all her life’. This low mood had been accentuated by a recent breakup. She defined herself as ‘quite a sad person’ with ‘intense periods of sadness with no apparent cause’. She considered this sadness as something inherent to her nature. For this reason, she had never been determined enough to consider attempting to change, viewing this as futile. However, in recent conversations with her work colleagues, many of whom were psychologists, they had remarked that this could be something that had been learnt and that there was the option to change many emotional problems. This is what had motivated her to seek the help of the clinical psychology centre.
On the date of the first interview, X. was living with her parents and, until the week before, also with her sister, but she had left home. X. spoke about her problematic childhood, with a father who maltreated both his wife and daughters. Her mother left home to elope with another woman, and returned two years later to re-join the rest of the family. Her method of coping with her father's maltreatment as well as her mother's disappearance and reappearance was to avoid talking about it and pretend as if it had never happened.
With respect to the familial relationships, she said that it was ‘practically non-existent’ with her father and that she felt ‘kind of responsible’ for her mother and felt ‘hated’ by her sister, whom she had not spoken to for a few years. As for her academic and professional life, X. had started to work at the age of 15, working and studying simultaneously, gaining Professional Teaching Qualification. As of the first interview, she was working as a qualitative market analyst, having risen to this position in the company where she began as s secretary.
With regards to her love life, X. had had two long-term relationships from the age of 16, with a period of two years of being single, after which she began her relationship with P. He had ended the relationship one month before her initial consultation, and this break up was the main catalyst for the session. The break up had happened precisely because of the client's constant sadness. X. expressed that she was ‘a burden for all couples’.
Lastly, regarding her social relationships, X. indicted that she had neither had friends in childhood nor in adolescence, something which she attributed to her ‘way of being very introverted’, defining herself as a ‘solitary person’. Nevertheless, she did established that, in more recent months before the interview, she had socialised more along with her boyfriend, although her boyfriend had always made the plans and therefore socialising had become less frequent after the break up.
After the first interview, the therapist made the X.’s case formulation, in which she related the tendency to sadness and social inhibition to the characteristics of the family environment in which the client was brought up and still lived.
Since it was an unpredictable environment in which neither sister knew what to do to avoid being beaten up by her father, both of them generated a state of learned helplessness (Maier & Seligman, 1976) that kept them rather inactive and low profile in the family context given the impossibility to escape from it as they were still minor. This environment also reduced significantly the level of interaction that the girls had with their peers, who could have ended up becoming friends, hindering the development of social skills. These two facts were the main consolidators of the introverted and sad character of X.
This sadness had remained until the first interview due to the fact that X. stayed in an environment that had remained virtually unchanged mainly due to the continued avoidance by all family members of talking about the situations that had taken place years ago. This therefore consolidated a pattern of elusive and avoidant interaction with little affection and significant roughness.
During the second session, the psychologist explained to X. the formulation of her case, to which X. expressed her agreement. The therapy goals that were agreed in this session included reducing sadness and guilt, improving social skills in family settings and first encounters, and leaving the parents’ house for her own home.
In order to preserve the ethical and professional guarantees in the study, we obtained the informed consent from the client, the therapist, and the director of the centre to record and transfer the clinical sessions, in line with articles 40 and 41 of the Code of Ethics of the Profession of Psychologist. This procedure was approved by the Research Ethics Committee of the Universidad Autónoma de Madrid.
InstrumentsGiven that we have used the observational methodology in this study, the instruments included herein are those employed for the observation and codification.
The recording of the cases was carried out in a closed circuit of cameras pointing exclusively to the therapists with the aim of preserving the client's anonymity.
The category systems of the client's adaptive verbalizations (SISC-ADAPT-CVC) and its subsequent response by the therapist (SISC-ADAPT-CVT) were developed ad hoc for this study.
The software used for the observation and register of the recorded sessions, as well as for the analysis of the inter-observer reliability of the registries obtained, was version 12.0 of The Observer XT ®, tool commercialized by Noldus Information Technology.
Procedure- •
Collection of audio-visual materials. We collected the recordings corresponding to the 13 clinical sessions of the X. case in compliance with all ethical criteria and guaranties of confidentiality.
- •
No systematic observation of the sessions. We first observed the recordings of X.’s case with the purpose of establishing the type of problem, the problem areas and behaviours and their evolution.
- •
Establishment of the base line. We then exhaustively observed the sessions covering the evaluation (session 1) and the return of the functional analysis (session 2) with the goal of determining the initial criteria that would allow the identification, in comparison, of the client's adaptive verbalizations.
- •
Initial formulation of a categorization system of the client's adaptive verbalizations. We developed an initial categorization system of the client's adaptive verbalizations based on the content of her speech and the main problem areas with the advisory of an expert psychologist.
- •
Refinement and final formulation of the categorization system of the client's adaptive verbalizations. We proceeded with the exhaustive registration of the client's adaptive verbalizations using the initial categorization system. During this process, we identified certain difficulties related to the categories and the initially proposed categorization rules. After analysing and discussing these difficulties, we then proposed a categorization system that would overcome them: SISC-ADAPT-CVC.
- •
Systematic registration of the client's adaptive verbalizations and inter-observer reliability analysis. We conducted an exhaustive registration of the client's adaptive verbalizations using the SISC-ADAPT-CVC system and the software tool The Observer XT ® version 12.0. Two observers conducted this task. We then randomly selected three of the thirteen sessions of the X. case in order to analyse the inter-observer reliability degree using The Observer XT ® version 12.0.
- •
Descriptive analysis of the evolution of the client's adaptive verbalizations. Once all X. case sessions were registered using the SISC-ADAPT-CVC system, we then analysed the way in which the frequency of the client's adaptive verbalizations was distributed throughout the therapy, both in absolute terms and grouped by the SISC-ADAPT-CVC categories.
- •
Detailed observation of the fragments following adaptive verbalizations and formulation of a categorization system of the therapist's verbal behaviour. We observed, for all sessions composing the clinic case, the fragments that followed each of the client's adaptive verbalizations with the goal of analysing the therapist's verbalizations in relation to them and be able to propose a categorization system for their registration: SISC-ADAPT-CVT. Such system was developed with the advisory of an expert psychologist.
- •
Systematic registration of the therapist's verbalization and inter-observer reliability analysis. We conducted an exhaustive registration of the fragments following adaptive verbalizations from the client using the SISC-ADAPT-CVT system and the software tool The Observer XT ® version 12.0. Two observers conducted this task. We then randomly selected one of the thirteen sessions of the X. case in order to analyse the inter-observer reliability degree using The Observer XT ® version 12.0.
- •
Descriptive analysis of the evolution of the therapist's verbalizations and its relationship with the client's adaptive verbalizations. Once we registered the therapist's verbalizations following the client's adaptive verbalizations, we analysed the way in which the former were distributed throughout the therapeutic process in each category. Lastly, we conducted an exploratory analysis of the relationship between the client's adaptive verbalizations and their relationship with the subsequent verbalizations from the therapist.
In Table 1 we show the categories that we employed for the registration of the client's adaptive verbalizations throughout therapy.
Category Definitions in the Categorization system SISC-ADAPT-CVC
| Categories | Definition |
|---|---|
| Self | Verbalizations about the client's self-esteem both in her personal and professional life; positive aspects of the client; her capacity to change as individual; well-being and positive frame of mind; recognition of achievements and personal qualities; as well as descriptions of third parties’ verbalizations about her noticeable improvements. |
| Family | Verbalizations regarding the accomplishment of tasks that involve her family (sister, mother and father); as well as descriptions of her family members and her relationship with them in an adaptive way. Taking into account the client's learning history, this implies verbalizations about her ability to choose and personal autonomy of each family member and their responsibility for their actions, as well as the improvement in the way she relates to them and the description or anticipation of the facing to talk about the past as an event avoided. |
| Partner | Verbalizations related to following the therapist's instructions regarding the development of the relationship with her partner and decision-making, and her commitment to such decision, around the desire to resume or not the relationship. It also includes verbalizations about her self-autonomy and the right and/or desire of being by herself in order to focus on herself. |
| Social relationships | Verbalizations about accomplishing the tasks of developing new social circles, including work colleagues and people other than her ex-boyfriend and her family; as well as verbalizations about well-being and social achievement. |
In Table 2 we show the Cohen's Kappa index values (k) and the inter-observer's percentage agreement (PA), which were calculated using a tolerance window of 2seconds. The Kappa index values are above .75, allowing us to classify them as excellent according to Bakeman (2000) and Landis and Koch (1977), and to reject the hypothesis that the agreements need to reach a confidence level of .99.
Evolution of the Client's Adaptive VerbalizationsWe registered a total of 539 adaptive verbalizations. Figure 1 shows the distribution and evolution of the absolute frequencies of the client's adaptive verbalizations throughout sessions.

As can be seen, the client's adaptive verbalizations show a practically inexistent frequency in the first session, after which the tendency is to gradually increase, reaching the highest peaks by mid-treatment, especially between the sixth and ninth sessions. Afterwards, there is a decreasing tendency in this type of verbalizations, although never going below the first session.
Regarding each isolated category, we find peaks and valleys in each of them, maintaining the same growing trend between the third and eleventh sessions and the following decrease. As per the family category, we can clearly see two increases in the appearance frequency of these verbalizations, with a decrease between sessions five and eight. During these sessions, there is a noticeable increase in the appearance frequency of adaptive verbalizations related to social relationships that similarly decreases gradually in final quarter of the therapy. As per the category partner, we found that its highest growth does not take place in the middle sessions but towards the end of treatment, in sessions eleven and twelve, retracing in the last session to low levels. Lastly, regarding the self category, there is also a significant growth in frequency around the middle sessions of the therapy, after which it decreases. Contrary to the other categories and the overall adaptive verbalizations, it shows a growing trend in the last two sessions.
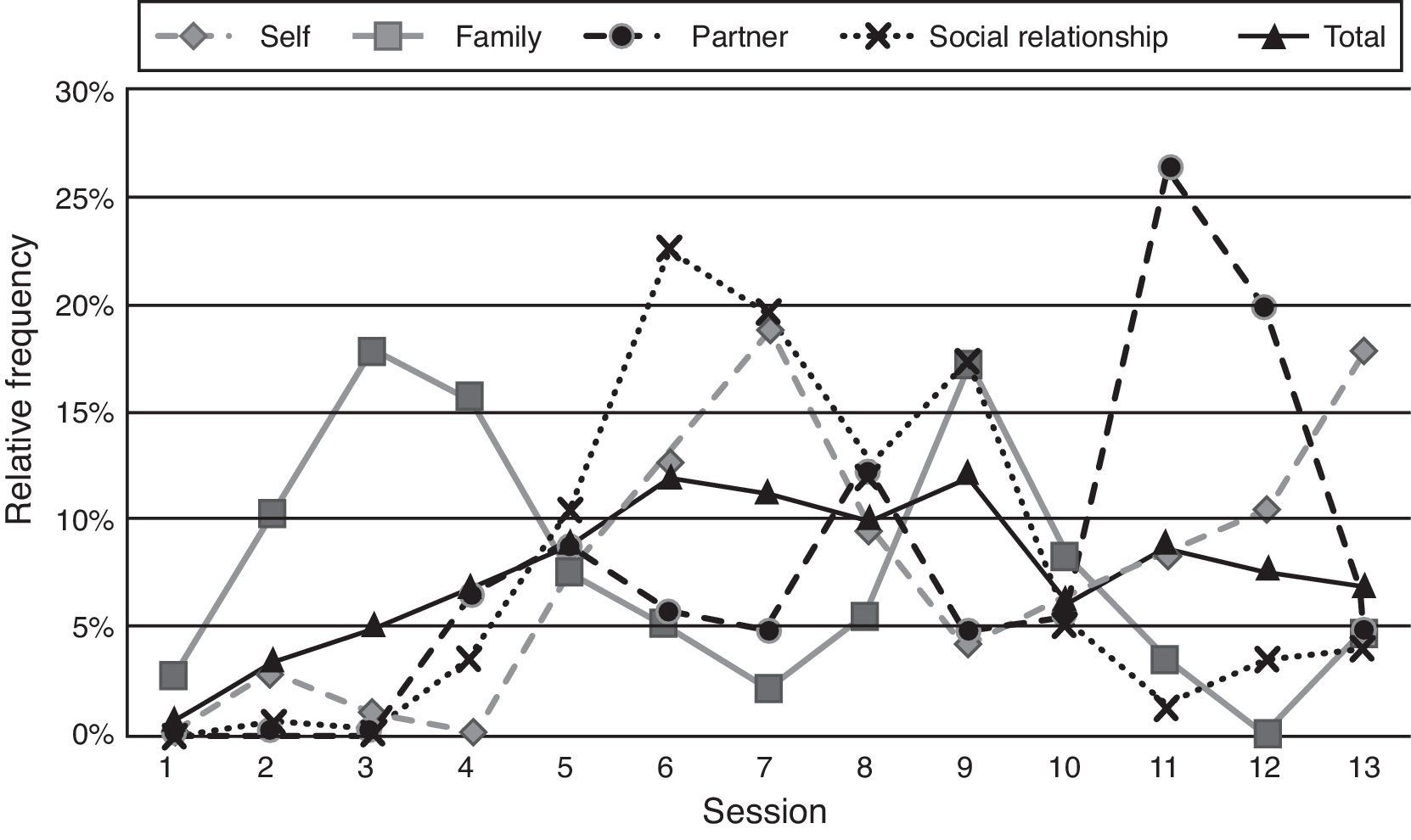
Figure 2 shows the distribution of the adaptive verbalizations in relative terms to their frequency of appearance throughout the entire treatment, both grouped and by categories. This allows us to see more clearly their evolution in relation to the chronological moment of the therapy.

On this figure we can see certain nuances with respect to the trends of appearance of the previously mentioned client's adaptive verbalizations.
More precisely, we can see how the verbalizations around the problem area partner show their highest relative frequency in the last therapy sessions, in sessions 11 and 12.
Further, and contrary to the expected direction, while the rest of categories show very low relative values in the last session, the self category presents its second highest appearance index in terms of relative frequency during this session.
Against this, the global trends in appearance of adaptive verbalizations do show the expected course: very small levels in the initial sessions, a gradual increase to reach the highest levels in the middle sessions and a final decreasing trend.
Categorization System of the Therapist's Verbalizations (SISC-ADAPT-CVT)Table 3 presents the categories employed for the registration of the therapist's verbalizations immediately following the client's adaptive verbalizations.
Category Definitions in the Categorization System SISC-ADAPT-CVT
| Categories | Definition |
|---|---|
| Repeat/complete speech | Verbalizations that, following the client's speech, complete, repeat, reformulate or summarize it. In the latter two cases, it refers to allusions to the client's previous speech concluded in an evident way, without any opinion from the therapist. |
| Express opinion | Verbalizations of therapist's opinions and personal or professional points of view about a client's verbalization, as well as recommendations about it. |
| Congratulate/flatter/highlight change | Greeting verbalizations by the therapist to the client, as well as references to the improvement of frame of mind or client's skills in relation to previous moments in therapy. |
| Show agreement/interest | Agreement verbalizations with the immediately preceding client's speech or expressions of interest in it. |
| Request information | Verbalizations that, following the thread of previous discourse or breaking it up, pursue the provision of information by the client. |
| Mention information from other sources | Verbalizations of explicit reference to information acquired through other sources, whether information from interviews in previous sessions, in the same session or with other assessment instruments. |
| Other | Interruptions, continuing with the previous therapist's speech with no regard to the client's speech, proposing tasks not directly related to what had been immediately said, and any verbalization that can not be included in any of the other categories. |
Table 4 shows Cohen's Kappa index value (k) and the inter-observer's percentage agreement (PA), which was calculated using a tolerance window of 2seconds. Again, the Kappa index is excellent (Bakeman, 2000; Landis & Koch, 1977), allowing us to reject the hypothesis that the agreements need to reach a confidence level of .99.
Evolution of the Therapist's VerbalizationsWe registered 793 therapist verbalizations following the emission of adaptive verbalizations by the client.
In terms of total frequencies by category, we observed that the most frequent category was Congratulate/flatter/highlight change, more than doubling the appearance of Express opinion, the second most frequent category. At the same time, Express opinion showed a very similar appearance frequency to Request information and Show agreement/interest. The lowest frequency levels were found in categories Repeat/complete speech, Other and lastly, Mention information from other sources.
Figure 3 shows these results in a graphical form, compared to the relative frequency of the set of adaptive verbalizations expressed by the client throughout the entire therapy.

With the goal of exploring the way in which the therapist's verbalizations are distributed in relation to its more or less agreeable character, we grouped the frequency of the categories Repeat/complete speech, Congratulate/flatter/highlight change and Show agreement/interest, given their rather agreeable topography. We also grouped the categories Request information and Express opinion given their variant topography, as they are sometimes considered more agreeable – when immediately linked to the client's speech or when providing technical information that justifies the client's situation, while other times are considered more aversive – when they break the previous speech or call attention to changes in the client's behaviour that are still to be introduced after an adaptive verbalization from the client. Lastly, we grouped the categories Mention information from other sources and Other, given their predominantly aversive character, in the sense that the former was registered in situations where the therapist made reference to previously obtained information which contradicted the client's verbalization and the latter was registered when the therapist continued her own speech ignoring the client's verbalization or when she directly interrupted the client.
In order to compare the results of these groupings, we calculated the relative appearance frequencies of the appearances of each group in the overall therapy. A graphical representation of these results is depicted in Figure 4.

As shown, all three groups have a growing trend in the first sessions, but differ in the way they are distributed after the third session: verbalizations with rather agreeable topography are concentrated between sessions 6 and 9 and decrease progressively towards the end of the treatment and surpassing the other two groups in the last session. Variant topography verbalizations are concentrated in sessions 5, 6, 8, and 9, with a marked decrease in session 7 and the final sessions. As per those verbalizations with a rather aversive topography, we see significant appearance points in the fourth, sixth, and eleventh sessions, surpassing the other two groups towards the end of the treatment albeit almost disappearing in the last session.
DiscussionAs previously indicated, this work is framed inside a broader line of research that aims to explain the learning processes that take place in the therapeutic context linked by the verbal interaction between therapist and client. As such, it constitutes an initial specific approach to the process of verbal reinforcement by the therapist to the client's adaptive verbal behaviour.
It should be pointed out that the conclusions that can be extracted from this study have an intrinsically limited reach, since they are the result of a single case study executed using an observational and descriptive methodology with no experimental manipulation. This prevents us from, among other things, isolating the effect of the therapist's verbalizations on the client's clinical change, and therefore, proposing their reinforcing functionality.
Despite the limitations inherent to this type of study, we consider that some conclusions can be extracted from the analysis of the results obtained. These conclusions are set forth below.
In regard to the client's adaptive verbalizations, these presented, in general, the expected trend throughout the therapeutic process, with virtually null values in the first session, progressively increasing to reach the highest peaks in the treatment's middle sessions, and progressively decreasing to show very low values in the last session.
The practically non-existent adaptive verbalizations in the first session can be explained by the fact that the client, as it frequently happens, comes to therapy in a critical moment of her life, so it is expected for her verbal repertoire to be eminently maladaptive. Moreover, the therapist's clinically relevant activity in this first session is mainly to evaluate, discriminating verbalizations of relevant information about the client's current situation in order to formulate the case (Ruiz-Sancho et al., 2015).
The fact that the client's adaptive verbalizations gradually increase from the second session is in line with the fact that these can start being reinforced by the therapist trough her consequent verbal behaviour. However, as previously indicated, the methodology used does not allow us to isolate this factor's effect from other possible explaining factors.
Regarding the last sessions, it could have been possible to expect that, as a result of the psychological therapy, the client's adaptive verbalizations would show either a lineal increase or an increase and stabilization on high values, but never a final decrease in frequency. This distribution, far from contradicting with the client's clinical improvement, is coherent with the nature of psychological therapy and with the attainment of the therapeutic goals. Firstly, we should take into account the fact that the definition of adaptive verbalization used in this study refers to those client verbalizations that show an approximation – compared to previous moments in therapy – to the therapeutic goals in the different problem areas proposed during the case formulation, i.e., the problem areas how the client perceives herself and how she relates with her family, ex-couple, and others. Therefore, we could expect that, once the therapeutic goals have been achieved and the problems of each area have been solved, the client's speech would progressively move away from these contents, which are no longer so relevant for therapy or for everyday life, and replacing them for new ones void of problematic. What can be observed in the last session is, precisely, the way in which therapist and client maintain an apparently non-transcendental conversation about the latter's possible future if she decides to move abroad to work. This is directly related to the second aspect to be considered: according to the group's previous studies (Ruiz-Sancho et al., 2013; Ruiz-Sancho et al., 2015), we can expect that when the therapist's primary goal is to consolidate already achieved changes, which happens precisely in the last session, she will try to discriminate those client verbalizations which are not directly related to the problem areas of her case formulation but that are, from a broader perspective than the one strictly used in this study, also adaptive.
The frequency of appearance of client's adaptive verbalizations in isolated categories show a more unstable tendency, with peaks and valleys, which could seem incoherent with the general evolution. However, these apparent irregularities also respond to clinical intervention's own natural course, in which diverse aspects of the different problem areas are being differentially influenced throughout the sessions, following a criterion of ease of change, relevance for the client's improvement and others. These aspects, once solved, are left behind in order to continue with the intervention on other therapeutic goals that could be framed in a different problem area, which could explain the peaks and valleys so common in category distributions.
However, there is an anomaly that does deserve specific attention due to the moment it takes place during therapy. The self category is distributed, like others, showing peaks and valleys throughout the therapeutic process. However, one of these peaks takes place precisely on the last session according to absolute and relative frequencies. The explanation for this phenomenon is related, on one hand, with what was previously exposed about the psychologist's actions when her goal is to consolidate achieved changes, and on the other hand, with the category's definition itself, which includes verbalizations of well-being and positive frame of mind, acknowledgement of achievements and personal attributes. In this last session, in which therapist and client talk about the future once the therapy ends, the client makes repeated mentions to her personal developments and well-being in retrospective and to her recently acquired will to focus on herself and enjoy life like she never did before. This verbalizations therefore fulfil, on one hand, the requirements of the categorization of the self category – reason why they get registered – but, on the other hand, are constituted as more global adaptive verbalizations and not related with problem areas already solved by that moment in therapy, which responds to the therapist's consolidation goal.
In regard to therapist's verbal behaviour, we can confirm that the most frequent verbalization after a client's adaptive verbalization is one that congratulates, compliments, or outlines the change. We can expect that, if the therapist gives her client's verbal behaviour the role that recent research is giving back to it (Montaño-Fidalgo, Martinez-Sanchez, Froján-Parga, & Calero-Elvira, 2013), she will remain alert to the occurrence of adaptive verbalizations on her client's part in order to reinforce them. At the expense of a detailed analysis on what can constitute a verbal reinforce for each client, we can expect that the therapist will use those verbalizations that, given their topography, can constitute with greater probability an appetitive stimulus. In this regard, handbooks of Behaviour Modification like Martin and Pear's (2007) present compliments in a prominent place among stimuli to choose from at the moment of reinforcing appropriate behaviour.
The occurrence of the express an opinion category after many adaptive verbalizations could be intended to, precisely, making the client aware of the adaptive features of her own behaviours to the extent that the therapy's goal should not only be the client's improvement but also to give her enough technical knowledge to be able to explain her own behaviour in functional terms (Kohlenberg & Tsai, 1991), in order to have a greater control over herself and prevent future setbacks, what would be, citing the famous Chinese proverb, like teaching to fish instead of giving the fish.
Regarding the many occasions in which the therapist asks for information after a client's adaptive verbalization, it is worth noting that many of these requests target the client's emission of verbalizations that are progressively more adaptive, generally as conclusion to a cognitive restructuring. In the following example, therapist and client maintain a conversation about the discomfort the latter feels for having negative feelings towards her father, who mistreated her as a child: (Therapist) “Do you think that the detachment feeling towards your father is damaging?” – (Client) “No” – (Therapist) “Do you think this is logical?” – (Client) “Yes” – (Therapist) “Do you think it is a product of a situation you experienced?” – (Client) “Yes” – (Therapist) “Good”. As can be seen, the therapist discriminates on the client verbalizations which are every time closer to the goal to finally congratulate her once achieving it by applying what could be considered verbal modelling (Froján-Parga & Calero-Elvira, 2011). On the other hand, these information requests can be intended to obtain more details around the client's adaptive verbalization, as it happens when asked about the way in which she conducted a task proposed during the previous session or how she felt doing it.
When grouping the therapist's verbalizations by topography, we found that most of the rather agreeable verbalizations concentrate around the middle sessions, where the largest instances of occurrence of adaptive verbalizations on the client's part are found. On the contrary, the more aversive verbalizations have one of their areas of most appearance towards the end of the treatment, accumulating 20% of their occurrence on sessions 11 and 12. These results could be explained alluding to the phenomenon of satiation of the reinforce (McSweeney, 2004) where, after receiving an elevated number of specific reinforces, their value for the subject would diminish to the point where presenting them would not produce any reinforcement. This, added to the pavlovian character of language (Staats, 1997; Staats & Hammond, 1972) could lead, in case the verbal stimulus is still being presented once its reinforcing value has disappeared, to the extinction of the association between such verbal stimulus and the positive effect it would have previously provoked by classical conditioning. With the intention of avoiding this phenomenon of satiation in the client and, by contrast, favour the resistance to the extinction of her adaptive verbalizations as a whole through their intermittent reinforcement (Martin & Pear, 2007), the therapist would then diminish the frequency of emission of verbalizations of rather agreeable topography, substituting part of these with other types of verbalizations, including those of a rather aversive topography.
In summary, the results of the exploratory analysis of this case study bring up some possible implications for the clinical psychologist in order to conduct a successful intervention. Firstly, the importance of taking into account the relevant role of verbal behaviour in therapy as a means to access the client's problems and as a tool to influence over it in the therapeutic context itself (Kohlenberg, Tsai, & Dougher, 1993). This deviates the attention over the debate about what is more important for the achievement of clinical change, the application of techniques of psychological intervention or the therapeutic relationship. On the contrary, it centres the attention on the fact that both are a result of the verbal interaction between therapist and client, which starts up learning processes that facilitate the achievement of the therapeutic goals (Froján, 2011). Secondly, the pertinence of paying attention to the occurrence of client's verbalizations which describe or anticipate well-being, achievement or the following of the instructions provided, as well as those which explain his/her behaviour and implications in functional terms, in order to introduce agreeable verbalizations in a contingent way with the goal of reinforcing them, in line with what is proposed by the Functional Analytic Psychotherapy (Kohlenberg & Tsai, 1991). Lastly, the relevance of spacing the introduction of verbal reinforces while the therapeutic goals are being achieved, with the double intention of avoiding satiation and promoting resistance to the extinction of adaptive verbalizations as a class of response, as well as creating room for the occurrence of adaptive verbalizations not linked to already solved problem areas.
At this point, it is worth highlighting some of the limitations of this study that would have enriched the results and conclusions. In first place, not having registered the therapist's verbal behaviour previous to the emission of each of her client's adaptive verbalizations. Had this happened, such register would have allowed us to corroborate if, as proposed by both the Analytical Functional Psychotherapy (Kohlenberg & Tsai, 1991) and the same research group in which this line of work is framed (Froján-Parga et al., 2008; Froján-Parga et al., 2011), the therapist does discriminate adaptive verbalizations to the attempt to reinforce them. In second place, although the prosodic component of language was indeed taken into account, the same could not be done regarding the client's non-verbal language. Due to ethical reasons and professional and research deontology, the client's image was not recorded on the videos used to produce registers. For this reason, the therapist's non-verbal language was also discarded, which caused some of the registers of the Others category when she went silent; silence, on the other hand, was charged of meaning. As previously mentioned, given the methodological characteristics of this case study, the conclusions that can be extracted from it are of an exclusively descriptive character. We point towards possible directions of interest for future studies that analyse in a more detailed way and with a methodology that is closer to experimentation the reinforcement phenomena that take place in the clinical context. The present study seems to point out, as expected, that verbalizations referring to the client's progresses in respect to her problem areas are distributed, as a whole, in a shape similar to an inverted U. The same happens with the consequent therapist's verbalizations of a rather agreeable topography, and therefore probably more reinforcing, establishing a close relationship between both at least at an exploratory level. Experimental research will be required, with a larger sample, in order to determine if such relationship is, as it seems, causal, or on the contrary, anecdotic. This will also be required to explore the possible existence of more or less reinforcing verbal repertoires and their possible interaction with the characteristics of both therapist and client.
Conflict of InterestThe authors of this article declare no conflict of interest.
