




To verify the incidence of facetary and low back pain after a controlled medial branch anesthetic block in a three-month follow-up and to verify the correlation between the positive results and the demographic variables.
METHODS:Patients with chronic lumbar pain underwent a sham blockade (with a saline injection) and then a controlled medial branch block. Their symptoms were evaluated before and after the sham injection and after the real controlled medial branch block; the symptoms were reevaluated after one day and one week, as well as after one, two and three months using the visual analog scale. We searched for an association between the positive results and the demographic characteristics of the patients.
RESULTS:A total of 104 controlled medial branch blocks were performed and 54 patients (52%) demonstrated >50% improvements in pain after the blockade. After three months, lumbar pain returned in only 18 individuals, with visual analogue scale scores >4. Therefore, these patients were diagnosed with chronic facet low back pain. The three-months of follow-up after the controlled medial branch block excluded 36 patients (67%) with false positive results. The results of the controlled medial branch block were not correlated to sex, age, pain duration or work disability but were correlated with patient age (p<0.05).
CONCLUSION:Patient diagnosis with a controlled medial branch block proved to be effective but was not associated with any demographic variables. A three-month follow-up is required to avoid a high number of false positives.
The American College of Physicians and the American Pain Society recommend that patients with low back pain should be classified into one of three pain categories to allow for a proper clinical approach: back pain potentially associated with radiculopathy or spinal stenosis, back pain potentially associated with another specific spinal cause or nonspecific low back pain. Although imaging is recommended in cases with specific low back pain (i.e., when severe or progressive neurologic deficits are present or when serious underlying conditions are suspected on the basis of history and physical examination), clinicians should not routinely obtain imaging or other diagnostic tests in patients with nonspecific low back pain (1); such patients can comprise 85% of all patients with lumbar pain complaints (2). Muscle contractions or myofascial syndromes, intervertebral disc or facet joint problems can cause the pain (1).
Between 8% and 12% of all patients with lumbar pain comprise chronic cases, with complaints lasting longer than three months (3,4). Facet joint disturbances can be responsible for 10% to 50% of all cases of chronic lumbar pain (5-8). However, clinical history or physical examination cannot identify facet joint alterations as the origin of pain (7,9-13), nor does imaging (e.g., radiography, computed tomography [CT] or magnetic resonance imaging [MRI]) (7,14-16). The only tool to identify facet joint alterations as the cause of pain is the verification of an analgesic response to anesthetic injections into the zygapophyseal joints or at their nerve supplies (17-20) and medial dorsal branch blocks are easier to perform (21). The diagnostic power of the blockade is based on the assumption that anesthetizing the facet joint or the capsule containing the innervations would result in pain relief. A positive result (i.e., pain relief) would mean that the facet joint is the site from which the pain originates. The technique of medial dorsal branch block consists of blocking each of the medial branches that innervate a facet above and a facet below their corresponding roots and also blocking the multifidus and interspinous muscles in the region of the corresponding dermatome (22,23).
However, several studies (20), have documented a high rate (varying from 25% to 40%) of false positive diagnoses in controlled medial branch blocks (CMBs) depending on the use of different anesthetics or saline solution as the control. There are many reasons for the high rates of false positives (e.g., the placebo response, use of sedation during CMBs, liberal use of anesthesia of the skin and subcutaneous tissue, use of large volumes of anesthetic, causing dispersion of anesthetics to other structures) (27). To minimize false positives, the following solutions are recommended: using saline controls (7,18,28,29) to avoid confusion with myofascial pain (24), reducing the amount of anesthetic applied to 0.5 ml at each point to avoid or reduce anesthesia of the skin as much as possible and avoiding the use of sedation for the procedure (7). No study, however, has investigated CMB after a three-month follow-up to verify whether the results are the same after such a period.
Therefore, the objective of this study was to determine the prevalence of low back pain after CMB immediately after the blocks and also after three months. The hypothesis to be verified here is that three-months of follow-up can modify the CMB results, thus, evidencing false-positives and altering therapeutic planning.
METHODSDesign, setting and ethicsThis prospective, controlled, diagnostic study was performed as the first phase of a randomized controlled clinical trial conducted by our team to analyze the effect of neurolysis in chronic facetary lumbar pain (registered in Clinicaltrials.gov under the number NCT01367860). This diagnostic study, which concerns the value of a three-month follow-up in diagnosing facetary pain in patients undergoing controlled medial branch block (CMBs), was approved by the local ethics committee (under protocol 337/10); all participants provided signed informed consent. The patients were informed that the procedure would be performed without topical analgesia and that there was a small risk of allergy to the injected lidocaine. The study was conducted from March 2011 to January 2013.
Sample and participant recruitmentThe participants in this study were patients with lumbar back pain being treated in public primary care settings in São Paulo city; they were referred to our specialized center or informed by relatives or acquaintances who had learned of the study and contacted our screening center. The study was open to anyone with lumbar back pain, regardless of the region of residence or registration at our hospital. All participants called the center by telephone and spoke with a nurse who applied the triage criteria: age (18 to 76 years old), lumbar back pain for three months or more without a specific diagnosis and the ability to visit the hospital for clinical evaluation. The nurse also collected certain demographic data, such as educational level and marriage status.
Following this assessment, an orthopedic surgeon (IDR) conducted a clinical evaluation, verifying the presence of nonspecific chronic back pain and using a visual analog scale (VAS) to evaluate pain intensity. Pain with a score ≥4 was a criterion for study inclusion.
The following exclusion criteria were applied: pain irradiating to the limbs (sciatica), previous lumbar spine surgery, pregnancy, history of drug abuse, history of psychiatric problems, rheumatologic diseases, fibromyalgia or lidocaine allergy, as well as the presence of fever or neurologic abnormalities in the physical exam. The patients who did not sign the consent form were also excluded.
Interventions and outcomeFor CMB, the patient was positioned in the prone position and monitored for vital signs. The participant was not sedated and did not receive any analgesic/anesthetic in the skin. Once positioned, the patient was asked to note (with a pencil) the intensity of pain using the VAS.
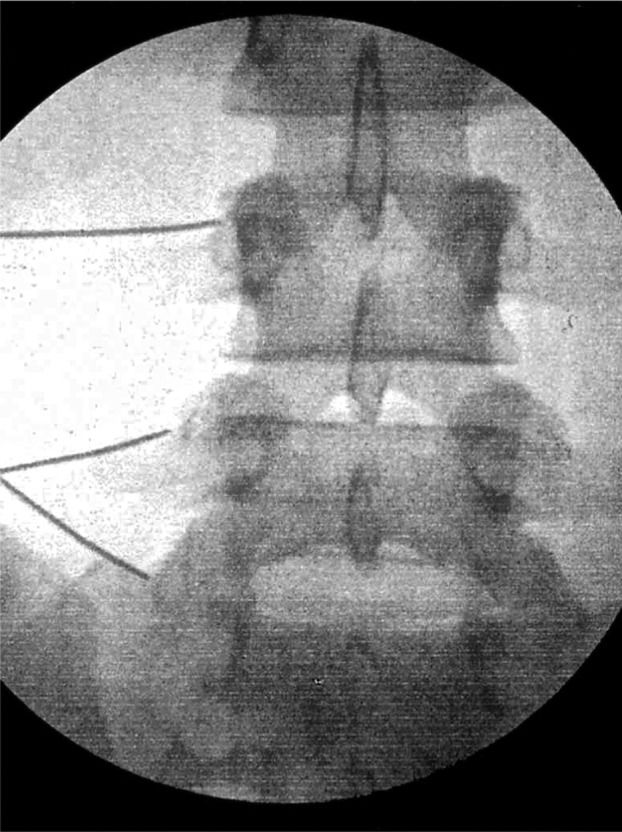
After the VAS was registered, the patient was warned that the test would begin with one injection and was asked to indicate the levels/sites of the most intense back pain. Saline solution (1 ml) was injected at these sites; 10 minutes later, the patient was again asked to indicate the pain intensity on the VAS. If the pain was improved by 50%, a placebo effect was detected and the patient was immediately excluded from the study and did not undergo CMB. If the pain was not improved, CMB was then applied. CMB was performed with a 25-G needle, 90 mm long, through the skin until reaching the medial branch nerves in L2, L3, L4 and L5 in both sides (Figure1). A dose of 0.5 ml of lidocaine at 2%, without epinephrine, was used in all cases. All procedures were performed by the same surgeon (IDR).
.")
After 10 minutes, the patient was again asked to note the pain intensity using VAS. If the pain improved by only ≤50%, the patient was excluded from the study and was referred for MRI to investigate the origin of the symptom. If the pain improved by >50% using VAS, the patient was included in the study and followed up.
The following day, the patient again visited the center for pain evaluation. The VAS analysis was repeated after one week, one month and three months. The VAS score was expected to be <4 in these evaluations; a score ≥4 would be an indication for neurolysis and the patient would then be included in the above mentioned clinical trial study. All VAS scores were recorded for statistical analysis.
Statistical analysisAt the end of the data collection, the patients' VAS data were tested for normal distribution with the Kolmogorov-Smirnov test using histogram subjective analysis. Given a normal distribution of the data, the averages and standard deviations were computed and subjected to parametric tests, including an analysis of variance (ANOVA) to verify the homogeneity of variance and the t-test for two independent samples. To analyze the association of dichotomous data, Fisher's exact test and chi-squared tests were used. For these data, we used the Kruskal-Wallis analysis for three or more groups and the Wilcoxon test for the comparison of two groups. For all tests, an alpha error of 5% was established.
RESULTSDuring the study period, 213 patients were screened by telephone at the center and 101 (47%) were excluded in this interview. The remaining 112 were clinically evaluated and 8 (7%) were further excluded: 3 because they did not agree with the study conditions and 5 because of the exclusion criteria (Figure2).

Among the 104 remaining patients who were initially evaluated with chronic back pain, 50 (48%) were men. Regarding race, 87 were white (85%), 7 were black (5%), 9 (7%) mulattos and 1 was Asian. Most patients (63%) were married or had been married for some time (15%). The patient ages ranged from 29 to 75 years (average, 49.56±10.97 years). Table1 shows the educational levels of the patient cohort.
At the moment of study inclusion, the patients had been experiencing low back pain for 33.11±39.85 months. Most patients (80%) were not using opioids for pain. Regarding work disability and social security benefits, 41 patients (39%) had already stopped working and were receiving government benefits. Among the 63 patients (61%) who were not receiving benefits, 21 (33%) felt they should receive benefits because of their pain.
The initial VAS score (before the first injection) was 75.72±18.20 on average.
Among the 104 individuals subjected to controlled medial branch block (CMB), 17 (16.3%) felt improvement with the saline solution injection and were excluded from this study, as were 33 (31.7%) patients who felt ≤50% improvement after the lidocaine injection. These 33 patients were referred for MRI and then diagnosed with degenerative diseases, except for one patient who had an osteoid osteoma in S1. Therefore, this study was completed with 54 patients undergoing CMB and all VAS evaluations.
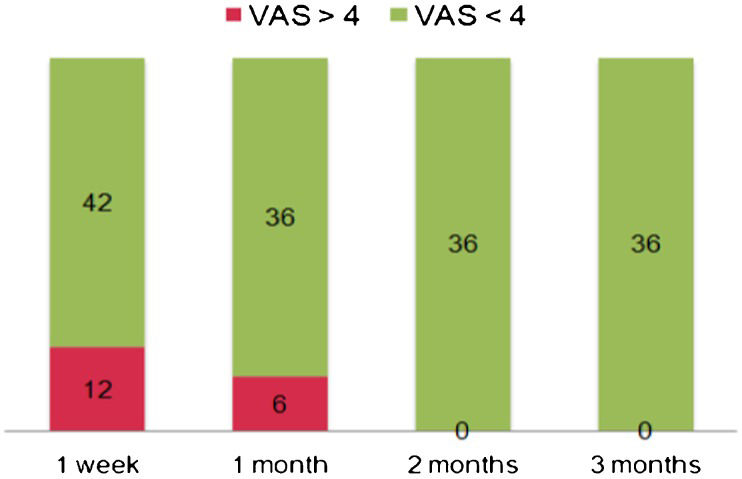
The average VAS score immediately after CMB was 43.27±31.23 (for the entire sample, n = 104). The average VAS score was 67.78±20.74 immediately after the CMBs among the 33 patients who did not respond well to the lidocaine injection (pain improvement ≤50%), whereas in the 54 well-responding patients (pain improvement >50%), the VAS score was on average 16.7±12.80. (Figure3) shows the patient distribution based on pain recurrence after CMB.
.")
The average age of the well-responding patients (n = 41) was 33.29±44.53 and the average age of the non-responding patients (n = 33) was 29.82±27.82 (p<0.05).
Of the 54 patients, 36 (67%) maintained pain improvement after three months, with a VAS score of 25.40±9.48. The remaining 18 (33%) experienced increases in pan, with a VAS score >4 and these patients were diagnosed with chronic lumbar facetary pain. Twelve patients (67%) felt pain again in the first week and 6 (33%) felt pain again one month after the CMBs.
The investigation of correlations between VAS scores and demographic variables, including the duration of pain, showed no significant association between any variable and VAS scores (p≥0.102) or between the demographic variables and VAS scores before and after CMB (p≥0.197).
DISCUSSIONImaging exams have been considered to be poor tools to identify chronic lumbar pain originating from the facet joints (30-33), as are a patient's clinical features and history (25,26). To the best of our knowledge, no controlled study has investigated the diagnosis of facet joint chronic lumbar pain using controlled medial branch anesthetic block (CMB) in an attempt to identify the prevalence of false positives in a three-month follow-up. Other studies have used CMB as a diagnostic tool for facet joint pain (34-37), but none have reevaluated the patients weeks after the blockade. We show here that it is important to reevaluate patients for weeks following the CMB procedure because when a patient begins to feel discomfort again after the effects of the lidocaine block have passed, it means that the source of pain was, in fact, the structure being anesthetized. However, as was the case of 67% of the patients (n = 36) in our sample, when pain improvement is maintained, it likely indicates that the symptoms do not originate in the medial branch nerves, which are no longer anesthetized; most likely, the cause of pain is myofascial and has been resolved in another manner. The remaining 33% of patients (n = 18) still had VAS scores >4 in the three-month follow-up, confirming the diagnosis of chronic lumbar facetary pain and these patients began to experience pain again in the first week (12) or first month (6) after the CMBs.
Patients undergoing CMBs can feel relief for an average of up to 14 weeks (25,26). In our study, the 36 patients with improvement after three months most likely had myofascial pain and the facet joint origin of the pain was correctly removed after the final follow-up, allowing them to be treated properly. Other studies did not follow positive patients after such a period (34-37); in such a situation, these 36 patients could have been inappropriately included in the neurolysis clinical trial as if they indeed had pain originating in the facet joint.
False-positive rates can be as high as 38% in CMB using lidocaine only in patients with low back pain (24). The false positive rate calculated from the result of bupivacaine-controlled block 3-4 weeks after the first procedure was found to be 27% for the lumbar spine (6). Considering that using a controlled procedure is important, we opted to limit confounding factors in our research, for instance, avoiding the use of sedation (7), which can interfere with neuronal plasticity (38) and restricting the volume of lidocaine to 0.5 ml per injection site, thus eliminating a possible myofascial effect (39). More importantly, however, was the use of a controlled block with saline solution (37,40) in a sham procedure that we were able to implement at the time of surgery, thereby eliminating the need to utilize the operating room, staff and materials a second time (with the associated costs). The placebo and lidocaine injections were 10 minutes apart, which allowed the immediate exclusion of patients feeling pain improvement with the saline solution.
Our study is most likely representative of the population (41) because the research was open to the community, without any restrictions regarding the place of residence or need for prior registration at our hospital. The patients were referred from primary care units from across the city or spontaneously reached us by telephone after being informed of the project by health professionals or acquaintances. In fact, as shown in other studies (6,25,26,42,43), we found no correlation of the results with demographic data, such as age, years of schooling or social security benefit.
One of the limitations in the present study is the fact that we did not evaluate depression symptoms, which could possibly interfere with chronic pain results. This evaluation could have been accomplished with scales such as the Zung-DV (Zung Self Rating Depression Scale) or MPI-DLV (Pain-Related Psychosocial and Behavioral Aspects). Nevertheless, van Wijk et al. (36) used these measures and observed no differences in depression prevalence between treated and placebo groups of patients undergoing radiofrequency denervation. Another study limitation is that, although we recorded the opioid use by our chronic low back patients, we did not perform a quantitative or qualitative analysis on this or any other analgesic. A recent study has shown, however, that pain sensitivity in chronic low back pain patients is not altered by chronic opioid intake (44).
In conclusion, the diagnosis of facet joint lumbar pain through CMB was proven to be effective but was not associated with demographic variables. A three-month follow-up is important to discard myofascial pain cases, which accounted for 67% of patients undergoing CMB.
AUTHOR CONTRIBUTIONSRocha ID and Cristante AF were responsible for study design, experimental study planning, manuscript writing, final review of the manuscript, data collection, analysis and interpretation. Marcon RM, Oliveira RP, and Letaif OB were responsible for data analysis and interpretation and final review of the manuscript. Barros TE was responsible for study design, experimental study planning, manuscript writing and final review of the manuscript.
No potential conflict of interest was reported.