



To determine the degree of reproducibility of maximum oxygen consumption (VO2max) among soccer players, using a modified Heck protocol.
METHODS:2 evaluations with an interval of 15 days between them were performed on 11 male soccer players. All the players were at a high performance level; they were training for an average of 10 hours per week, totaling 5 times a week. When they were evaluated, they were in the middle of the competitive season, playing 1 match per week. The soccer players were evaluated on an ergometric treadmill with velocity increments of 1.2 km·h−1 every 2 minutes and a fixed inclination of 3% during the test. VO2max was measured directly using a breath-by-breath metabolic gas analyzer.
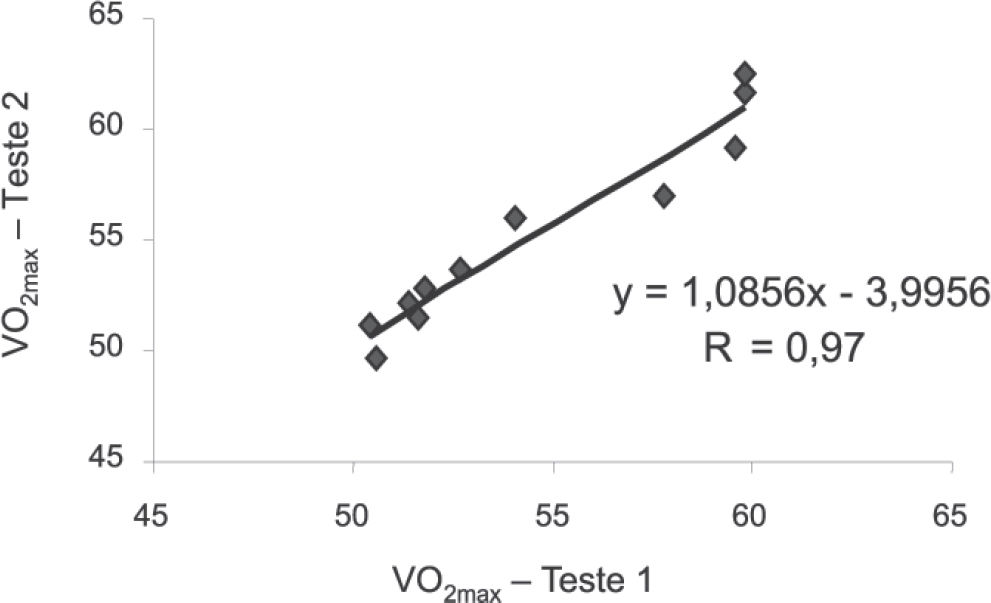
RESULTS:The maximum running speed and VO2max attained in the 2 tests were, respectively: (15.6 ± 1.1 vs. 15.7 ± 1.2 km·h−1; [P = .78]) and (54.5 ± 3.9 vs. 55.2 ± 4.4 ml·kg−1.min−1; [P = .88]). There was high and significant correlation of VO2max between the 2 tests with a 15-day interval between them [r = 0.97; P < .001].
CONCLUSION:The modified Heck protocol was reproducible, and the 15-day interval between the ergospirometric testing was insufficient to significantly modify the soccer players’ VO2max values.
Determinar o grau de reprodutibilidade do consumo máximo de oxigênio (VO2max) em jogadores de futebol utilizando o protocolo de Heck modificado.
MÉTODOS:Foram avaliados por duas vezes, com intervalo de 15 dias entre os testes, 11 futebolistas masculinos. Todos eram de alto nível, treinavam em média 10 horas por semana subdivididos em treinamentos físicos, técnicos, táticos e jogos competitivos, totalizando cinco vezes por semana e na fase em que foram avaliados se encontravam em pleno período competitivo realizando um jogo por semana. Os futebolistas foram avaliados em esteira ergométrica (1,2 km·h−1) a cada dois minutos e inclinação fixa durante o teste em 3%. O VO2max foi medido diretamente utilizando analisador metabólico de análise de gases expirados respiração-a-respiração.
RESULTADOS:A velocidade máxima de corrida e o VO2max atingido nos dois testes foram respectivamente: (15,6± 1,1 vs. 15,7 ± 1,2 km·h−1; [p = 0,78]) e (54,5 ± 3,9 vs. 55,2 ± 4,4 ml.kg−1.min−1; [P = 0,88]). Houve correlação significante e alta do VO2max entre os dois testes após 15 dias de intervalo [r = 0,97; P< 0,001].
CONCLUSÃO:O protocolo de Heck modificado foi reprodutível e o intervalo de quinze dias entre os testes ergoespirométricos não foi suficiente para modificar significativamente o VO2max dos jogadores de futebol.
Cardiopulmonary or ergospirometric tests have been widely used for studying functional capacity levels, assessing the effects of physical training and other measurements among non-athletes and athletes in various types of sports.1–6 The capacity to sustain exercise at varying degrees of intensity basically depends on 4 parameters: 1) the maximum oxygen consumption (VO2max); 2) the anaerobic threshold, above which lactate accumulation occurs; 3) the efficiency of mechanical work; and 4) the oxygen kinetics time.7 Maximum oxygen consumption is considered to be one of the most important parameters for aerobic function and has become extremely useful for evaluating cardiorespiratory performance in health and illness.8–13
Another important point to be considered as a prerequisite for studying the validity of any assessment procedure is the reproducibility of its measurements.14 In ergometry, various effort test protocols using treadmills and/or cycle ergometers, with different models for load increases, stage duration, and styles (ramped, stepped, or intermittent) have been used for testing VO2max and other metabolic variables.15–20 However, the validity and reproducibility of these protocols are not always tested.21 Moreover, the specialized literature has suggested that VO2max should be repeatedly measured within a maximum duration of 8 to 12 min. 15,22–25 The protocol tested in the present study had a mean repeat interval of 16 min. However, it was not the objective of this study to investigate this controversial question. Thus, to investigate the reproducibility of VO2max in a stepped protocol of progressive loads and fixed slope, we involved a homogenous sample of high-level soccer players.
MATERIALS AND METHODSSampleTwo evaluations were conducted on 11 soccer players who belonged to the junior category of a professional team in series A3, affiliated with the São Paulo Football Federation. These players were all performing at a high competitive level. The following inclusion criteria were used in this study: 1) age between 17 and 20 years and 2) mean of 10 hours of training per week, subdivided into physical, technical, and tactical training, totaling 5 times a week. At the time when they were evaluated, they were in the middle of the competitive season, with 1 match per week. Before undergoing the tests, the players were given explanations about the assessment procedures, the study objectives, and the possible benefits and risks, and they signed a consent statement in accordance with the requirements of the institution's Ethics Committee. The players’ ages and biometric characteristics are described in Table 1.
Mean values and standard deviations for age, height, body mass and fat percentage among the soccer players who underwent two ergospirometric tests with a 15-day interval between them, using the modified Heck protocol (n = 11).
| Variables | Test 1 | Test 2 | Student's t test |
|---|---|---|---|
| Age (years) | 18.6 ± 0.9 | ||
| Body mass (kg) | 69.0 ± 6.1 | 69.5 ± 6.3 | (p=0.800) |
| Height (cm) | 177 ± 7 | ||
| Fat (%) | 7.5 ± 3.2 | 7.3 ± 2.4 | (p=0.870) |
Note: The values represent means and standard deviations.
To avoid the effects of circadian variations, the soccer players underwent their 2 tests at the same time of the day.26–28 Thus, the evaluations were carried out in the mornings, starting at 8:00 AM, and in the afternoons, starting at 1:00 PM. The tests were conducted at room temperatures ranging from 20°C to 24°C, relative air humidity between 45% and 65%, and barometric pressures between 698 mm Hg and 705 mm Hg. In this study, the soccer players underwent 2 ergospirometric tests with an interval of 15 days between them, and they were advised to maintain their dietary habits and training routine over this period. They were also advised to avoid high-intensity exercises during the 24 hours preceding the effort test, and not to have drinks with high caffeine or alcohol content on evaluation day. The players had a light meal 1 hour before the test and came for the test dressed in T-shirts, pants, and running shoes.
Before the ergometric evaluation, and to investigate possible electrocardiographic abnormalities an electrocardiogram (EKG) was obtained. Their heart rates were recorded at rest, during effort, and during the recovery phase by means of simultaneous monitoring of 12 derivations (D1, D2, D3, AVr, AVl, AVf V1, V2, V3, V4, V5, and V6). These data were recorded on a computerized electrocardiograph (6.4, HeartWare, [Belo Horizonte, Brazil). To find the maximum heart rate during the test, the equation (208 – [0.7 x age]) was used.29 Arterial blood pressure was measured indirectly using an aneroid sphygmomanometer (Tycos, USA) at the end of each stage of the test, by means of the auscultatory method.30
Pulmonary ventilation (VEBTPS), oxygen consumption (VO2STPD), carbon dioxide production (VCO2STPD) and the respiratory quotient (RQ = VCO2/VO2) were calculated from the measured values using a computerized gas exchange analysis system (breath-by-breath) (CPX/D, Medgraphics, Saint Paul, MN, USA). Calibration and exchange of the pneumotachograph were performed before each test, with a syringe (5530, Hans Rudolph, USA) with a capacity of 3 L, with 100 mL of dead space used as a correction factor in determining the flow and respiratory volume readings. The oxygen analyzers (zircon) and carbon dioxide analyzers (infrared) were calibrated before and immediately after performing each test, using a known gas mixture (O2 = 11.9% and 20.9%; CO2 = 5.09%), and were balanced with nitrogen (N2) as well as with the atmospheric air composition itself. The ventilation variables were recorded instantaneously and then calculated for a mean time of 10 seconds.31–32 Thus, the breath-by-breath sampling technique evaluated the quantity of oxygen (O2) consumed, as the result of the difference between inhaled O2 from the atmosphere and the expired quantity of O2, and it also evaluated the carbon dioxide (CO2) production.33
The maximum physical capacity of the soccer players was found from an effort test on a motorized treadmill (ATL 10200, Inbramed, Porto Alegre, RS, Brazil) with variable velocity (km.h−1) and inclination (%). A continuous stepped protocol with a fixed grade inclination of 3% was used. In this protocol, the players spent 1 minute at rest and warmed up for 3 minutes at velocities of 4.8, 6.0, and 7.2 km·h−1 for 1 minute each. The test then began at 8.4 km·h−1, and the velocities went on increasing with increments of 1.2 km·h−1 every 2 minutes. The test was stopped when the player declared he was exhausted and/or if any important electrocardiographic alteration occurred (Table 2).34 The active recovery phase lasted for 3 minutes, starting immediately afterwards, with decreasing velocities of 6.0, 5.0, and 4.0 km·h−1 for 1 minute each. While both tests were in progress, the players were given continual verbal encouragement.35–36
Demonstration of the velocities and inclination of the modified Heck protocol used in this study
| Velocity/Inclination (km·h−1)(m·min−1) (%) | Duration of the Stage (minutes) | Accumulated Time (minutes) | |||
|---|---|---|---|---|---|
| Warm-up | |||||
| 4.8 | 80 | / | 3% | 1 | 1 |
| 6.0 | 100 | / | 3% | 1 | 2 |
| 7.2 | 120 | / | 3% | 1 | 3 |
| Exercise/running | |||||
| 8.4 | 140 | / | 3% | 1- 2 | 2 |
| 9.6 | 160 | / | 3% | 1- 2 | 4 |
| 10.8 | 180 | / | 3% | 1- 2 | 6 |
| 12.0 | 200 | / | 3% | 1- 2 | 8 |
| 13.2 | 220 | / | 3% | 1- 2 | 10 |
| 14.4 | 240 | / | 3% | 1- 2 | 12 |
| 15.6 | 260 | / | 3% | 1- 2 | 14 |
| 16.8 | 280 | / | 3% | 1- 2 | 16 |
| 18.0 | 300 | / | 3% | 1- 2 | 18 |
| 19.2 | 320 | / | 3% | 1- 2 | 20 |
| 20.4 | 340 | / | 3% | 1- 2 | 22 |
| 21.6 | 360 | / | 3% | 1- 2 | 24 |
| 22.8 | 380 | / | 3% | 1- 2 | 26 |
| 24.0 | 400 | / | 3% | 1- 2 | 28 |
*velocity increments of 1.2 kmh−1
The subjective perception of effort was estimated in each stage by means of Borg's graduated linear scale of 15 points (6-20).37–39 In the present study, the test was considered to have reached the maximum when the soccer players attained 2 of the following validation criteria: 1) maximum respiration exchange ratio (RER) ≥ 1.10; 2) Borg's scale of subjective perception of tiredness ≥ 18 and 3) maximum heart rate ≥ 95% of the maximum chronotropic response predicted for the age.8, 40–42 The criterion used for ascertaining VO2max was an increase in VO2 less than 2.0 mLkg−1·min−1 for an increase of 5% to 10% in the intensity of the exercise.43
Statistical Analysisa descriptive analysis of the soccer players was undertaken by calculating means and standard deviations for the variables of age, body mass, height, and fat percentage. To compare VO2max between tests 1 and 2, the Student t test for paired samples was used. In all analyses, the significance level accepted was P £ .05. To investigate any relationship that might exist for VO2max between test 1 and test 2, Pearson's correlation (r) was used.44
RESULTSThe variables of age, body mass, height, and fat percentage for the soccer players were compared across the 15-day interval between tests 1 and 2, and no statistically significant alterations were found (Table 1). The maximum running speed and maximum oxygen consumption (VO2max) attained by the players after the 15-day period between the tests were not significantly changed (Table 3). Thus, when the VO2max obtained in tests 1 and 2 was correlated across this time interval, the result was found to be highly reproducible and significant (r = 0.97; P < .001) (Figure 1).
Comparison between the means and standard deviations for the maximum running velocity and maximum oxygen consumption (VO2max) among the soccer players who underwent two ergospirometric tests with a 15-day interval between them, using the modified Heck protocol (n = 11).
| Variables | Test 1 | Test 2 | Student's t test |
|---|---|---|---|
| Vel. max (km·h−1) | 15.6 ± 1.1 | 15.7 ± 1.2 | (p = 0.780) |
| VO2max | 54.5 ± 3.9 | 55.2 ± 4.4 | (p = 0.878) |
| (ml·kg−1.min−1) |
Note: The values represent means and standard deviations.
 among soccer players, with 15-day interval between the tests.")
Test theory establishes that the usefulness of tests depends on fulfilling quality criteria. Prominent among these is the criterion of validity, defined as the degree of exactness with which a test measures what it is intended to measure. Logic or content validity that is constructed in the relationship between the nature of the test and its evaluation capacity is the most consistent criterion for validating a procedure.45 The present study was conducted to investigate the validity and reproducibility of VO2max measurements using a modified Heck protocol among high-performance soccer players.
The validity of a measurement first depends on the error in the methodology used, and also on the results from the variable obtained by repeated measurements. In the present study, the correlation found between the VO2max values after the 15-day interval between the tests was high and very significant (r = 0.97; P < .001). This correlation was within the range normally recommended for validating criteria and can be considered to be excellent.46
In addition to this, another important point to be considered as a prerequisite for a validity study is the reproducibility of the measurements. In this study, after the 15-day interval between tests 1 and 2, there was no significant difference in the VO2max measured (P = .88).14
From comments made by the participating soccer players themselves, another subjective characteristic observed while implementing the modified Heck protocol was the acceptability and comfort that this protocol provided for the test subjects. The individuals were able to warm up before beginning to run, and the load increments were not very aggressive (1.2 km·h−1). The inclination was fixed and not very great (3%), simulating the resistance of running on a grass lawn, which facilitated the movement of the soccer players on the treadmill.
As we aimed to achieve in this study, the specified duration, intensity, and progression of the stage must, insofar as possible, meet the characteristics of the activity of the individuals tested. These are matters that must be given due consideration in laboratory tests. When evaluations are not just for diagnostic or prognostic purposes but rather are for investigating performance and for advising on and evaluating performance, the type of protocol takes on great importance in relation to the result from an effort test. Traditional protocols of ergometric evaluation, such as those that Bruce, Ellestad, Balke, and others have frequently used in ergometric testing, adequately evaluate the cardiovascular response. However, in these protocols the athletes often complain about the steep inclinations of the treadmill that precipitates muscular peripheral fatigue due to less adaptation to the condition, diminishing the performance in the test. The modified Heck protocol used in our lab evaluates the cardiovascular response in the same way, but it presents an important advantage over the cited protocols, i.e., the lower inclination; consequently, the athlete does not perceive the inclination and the precocious sensation of fatigue is avoided. Saltin47 deemed it extremely important for the needs of the test to mobilize the right muscles in an appropriate manner, considering that much of the precision is lost if the test is not carried out using the specific exercise of the sport that is practiced, or something close to it. Strangely enough, all too frequently such recommendations are ignored in the majority of laboratory tests when treadmills are used. It is important to emphasize that disregard for the coordination of the movement, the mobilization of specific muscles, the recruitment of motor units and the involvement of cellular enzyme activity have implications for the performance of any motor action. This will certainly have a negative effect on energy production and consequently on the final yield from the test.
Some studies have demonstrated the importance of taking into consideration the similarity of the activity tested and the characteristics of the protocol. Strommer et al48 found that the VO2max values among cross-country skiers, rowers, cyclists, and track runners were 3% to 12% higher when such individuals were tested in activities similar to their type of sport than when the same athletes were tested by means of running uphill. In a comparative study between ice-hockey players and track runners, Leger et al49 found VO2max values 15% higher for the ice-hockey players under real playing conditions and 8% lower when evaluated on a treadmill. Roels et al50 compared VO2max among swimmers and triathletes on ergometric bicycles and in a swimming pool, respectively, and found that the swimmers had greater VO2max in the water (58.4 vs. 51.3 ml·kg−1·min−1) while the triathletes obtained better results on ergometric bicycles (68.2 vs. 53.0 mL·kg−1·min−1).
In the present study, we sought to adapt Heck's original protocol by decreasing the duration of each stage from 3 to 2 minutes, while the inclination went from 1% to 3%, thereby simulating the greater resistance of grass as experienced by soccer players, while the velocity increments (1.2 km.h−1) were maintained. Therefore, according to the population and the objectives of the functional evaluation, the type and design of the protocol applied is a strategy that must be considered in performance assessment procedures.
CONCLUSIONThe modified Heck protocol was safe, effective, and reproducible, and the 15-day interval between the ergospirometric tests while maintaining the same training routine was insufficient to result in a significant change in the soccer players’ VO2max values. Therefore, to ascertain the aerobic power in this type of sport, the VO2max values obtained via this protocol can be safely and reliably taken from a single assessment.
E-mail: fisiologistahc@bol.com.br