



The six-minute walk test (6WT) has been proposed to be a submaximal test, but could actually demand a high level of exercise intensity from the patient, expressed by a respiratory quotient >1.0, following the guideline recommendations. Standardizing the 6WT using the Borg scale was proposed to make sure that all patients undergo a submaximal walking test.
PURPOSETo test the reproducibility of the six-minute treadmill cardiopulmonary walk test (6CWT) using the Borg scale and to make sure that all patients undergo a submaximal test.
METHODSTwenty-three male heart failure patients (50±9 years) were included; these patients had both ischemic (5) and non-ischemic (18) heart failure with a left ventricle ejection fraction of 23±7%, were diagnosed as functional class NYHA II-III and were undergoing optimized drug therapy. Patients were guided to walk at a pace between “relatively easy and slightly tiring” (11 and 13 on Borg scale). The 6CWT using the Borg scale was performed two times on a treadmill with zero inclination and patient control of speed with an interval of 24 hours. During the sixth minute, we analyzed ventilation (VE, L/min), respiratory quotient, Oxygen consumption (VO2, ml/kg/min), VE/VCO2 slope, heart rate (HR, bpm), systolic blood pressure (SBP, mmHg), diastolic (DBP, mmHg) blood pressure and distance.
RESULTSThe intraclass correlation coefficients at the sixth minute were: HR (ri=0.96, p<0.0001), VE (ri=0.84, p<0.0001), SBP (ri=0.72, p=0.001), distance (ri=0.88, p<0.0001), VO2 (ri=0.92, p<0.0001), SlopeVE/VCO2 (ri=0.86, p<0.0001) and RQ<1 (ri=0.6, p=0.004).
CONCLUSIONUsing the 6CWT with the Borg scale was reproducible, and it seems to be an appropriate method to evaluate the functional capacity of heart failure patients while making sure that they undergo a submaximal walking test.
Heart failure can be considered as the last stage of heart diseases and as a significant cause of mortality and morbidity throughout the world.1 A limited effort tolerance is frequently both the first and most important clinical characteristic of heart failure, reflecting the reduction in cardiac function and the alteration in reflex, metabolic, vascular and muscular function.1,2
The maximal exercise cardiopulmonary test is performed to evaluate the functional capacity, therapeutic response and prognosis in heart failure patients.3,4 The six-minute walk test is proposed to be a submaximal exam that could reproduce a patient’s daily physical activities and evaluate the prognosis of heart failure patients.5 However, if the original version is followed, the six-minute walk test could demand a higher exercise intensity than that demanded during the patient’s daily activities,6–8 as expressed by a respiratory quotient (RQ)>1.0.6 The Centers for Disease Control and Prevention recognize submaximal activities as 3 to 6 METs, which corresponds to a moderate intensity for most young to middle-aged adults.6 To make sure that all patients undergo a submaximal test, a careful standardization was proposed using the Borg scale (submaximal is defined as between relatively easy and slightly tiring, which is between 11 and 13 on the scale).6 The reproducibility of this new standardization is unknown.
The aim of this study was to test the reproducibility of the six-minute treadmill cardiopulmonary walking test (6CWT) using the Borg scale in patients with stable heart failure and to make sure that all patients undergo a submaximal test.
MATERIALS AND METHODSTwenty-three male heart failure patients (50±9 years) were included in the study. Baseline characteristics are listed in table 1. Patients with any of the following were excluded from the study: non-optimized drug therapy, atrial fibrillation, cachexia, interrupted walk test prior to the sixth minute and noncardiovascular functional limitations, such as osteoarthritis and chronic obstructive pulmonary disease. Female patients were not included in this study due to the reduced number of females available during the study period.
Characteristics of patients
| Characteristics | Number of Patients (%) |
|---|---|
| Pathogenesis | |
| Ischemic | 5 (21.7%) |
| Chagasic | 4 (17.3%) |
| Idiopatic dilated cardiomyopathy | 7 (30.4%) |
| Hypertensive | 5 (21.7%) |
| Valvar | 2 (8.6%) |
| Left ventricular ejection fraction (echo), % | 23 ± 7 |
| Left ventricular end-diastolic diameter (echo), mm | 72 ± 16 |
| NYHA functional class | |
| II | 19 (82.6%) |
| III | 4 (17.3%) |
| Current medications | |
| Digoxin | 18 (78.2%) |
| Diuretics | 21 (91.3%) |
| ACE inhibitor | 19 (82.6%) |
| AT1 Blocker | 2 (8.6%) |
| Spironolactone | 13 (56.5%) |
| β-blocker | 14 (60.8%) |
| Amiodarone | 4 (17.3%) |
| Nitrate | 2 (8.6%) |
All patients were in stable clinical condition, without changes in medication for three months. Patients performed both tests at least two hours after a light meal. The 6CWT was conducted by two randomized physical therapists on two consecutive days.
All patients underwent the exercise test on a programmable treadmill (Series 2000; Marquette Electronics; Milwaukee, WI, USA) in a temperature-controlled room (21–23 °C) with continuous electrocardiography monitoring (Max 1; Marquette Electronics; Milwaukee, WI, USA), blood pressure monitoring (auscultation method) and ventilation and gas exchange monitoring (computerized system, Vmax 229 model, SensorMedics, Yorba Linda, CA, USA).
The 6CWT using the Borg scale was performed on a treadmill with zero inclination and patient-controlled speed7. All patients were advised to keep walking during the test at a pace between “relatively easy and slightly tiring” (between 11 and 13 on the Borg scale). The distance walked was recorded by the treadmill microprocessor. Encouragement was standardized with phrases like “if you can walk faster, increase the speed”, “you are doing very well” and “if it is tiring, you can reduce the speed”. Blood pressure was measured at rest and at the sixth minute. The electrocardiography, ventilatory, hemodynamic and gas exchange variables were continuously evaluated during the test but only collected at the sixth minute. The protocol was approved by the Ethical Committee of Heart Institute of São Paulo’s Medical School. All patients provided informed consent before participation.
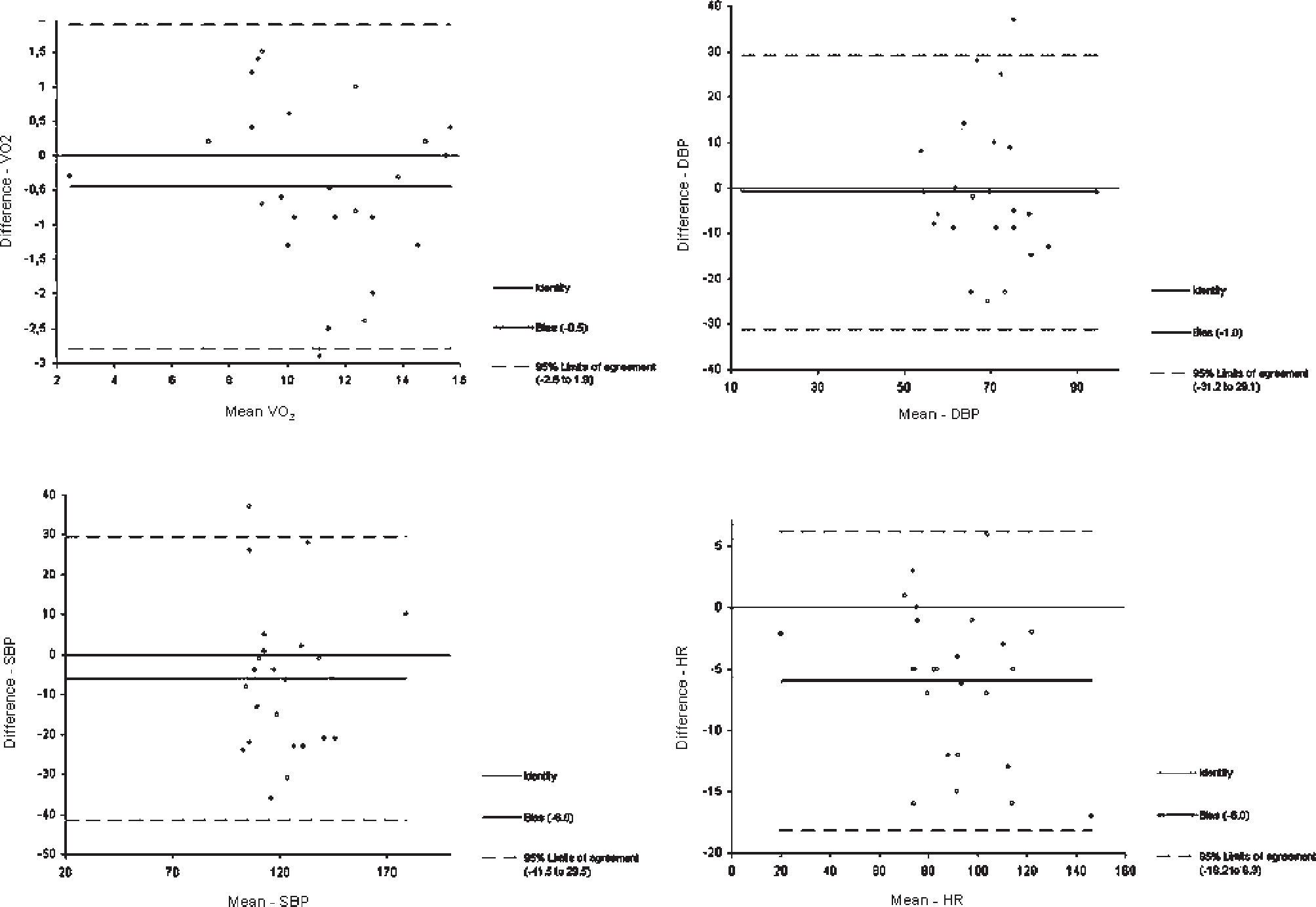
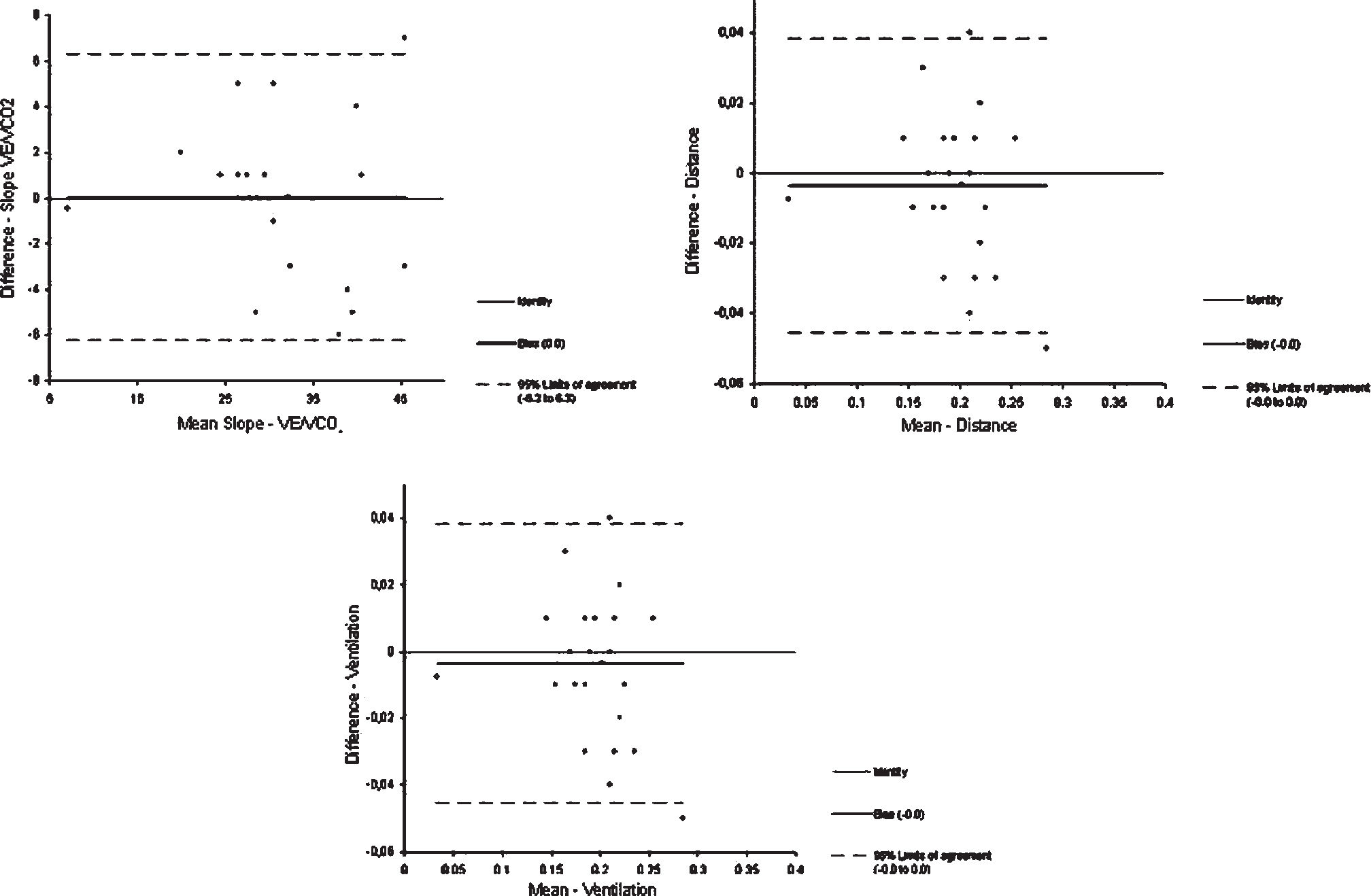
STATISTICAL ANALYSISData were analyzed using SPSS statistical software for Windows version 11.5 (SPSS Inc., Chicago, IL, USA). The descriptive analysis was presented as mean and standard deviation. Intraclass Correlation Coefficients (ri), with a 95% confidence interval, were calculated using analysis of variance (ANOVA)24 for the following variables: ventilation (VE, L/min), RQ, oxygen consumption (VO2, ml/kg/min), VE/VCO2 slope, heart rate (HR, bpm), systolic blood pressure (SBP, mmHg), diastolic (DBP, mmHg) blood pressure and distance (miles). p<0.05 was considered significant. Bland-Altman plots with 95% limits of agreements were also derived.
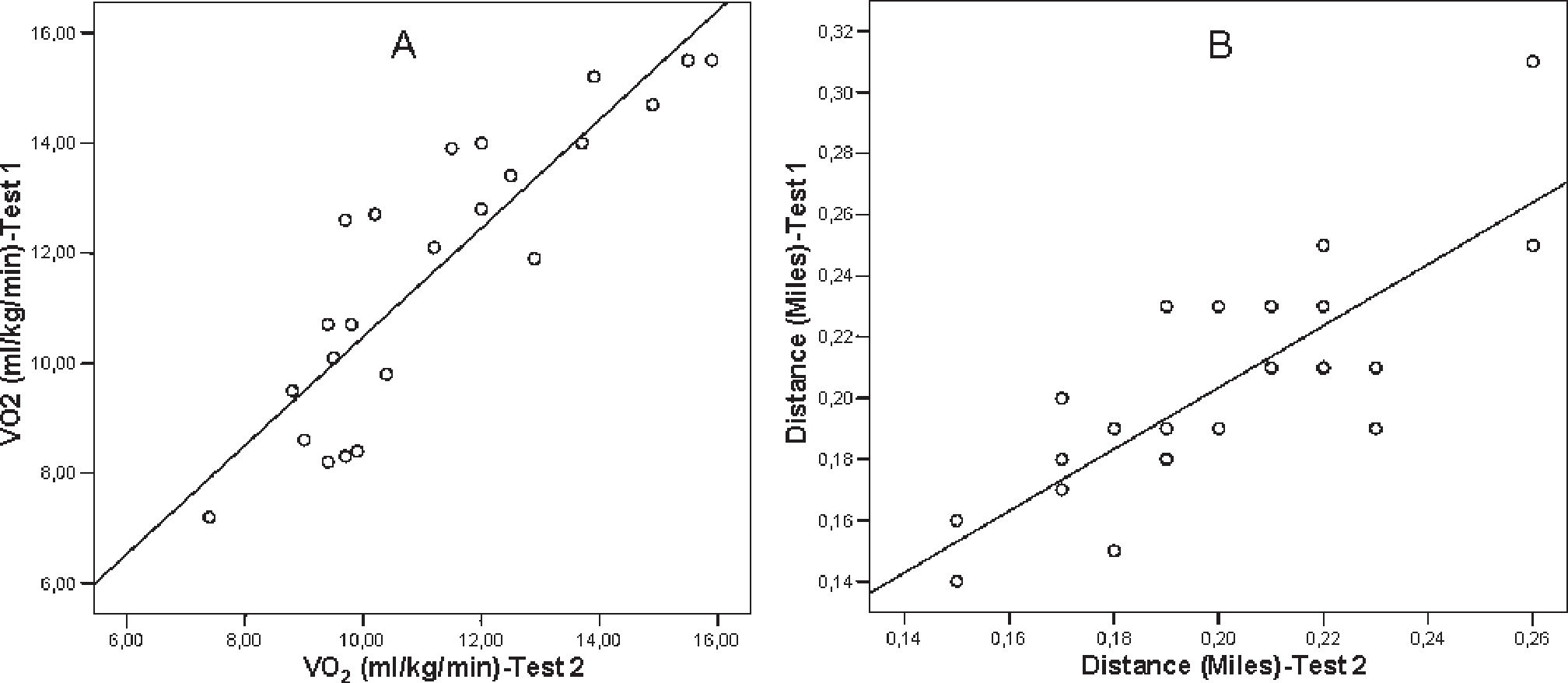
RESULTSAll patients were well-adapted to the six-minute walk test using the Borg scale and completed the protocol without interference. Results are listed in table 2 and the linear regression is presented in figure 1. The distance was highly reproducible between the two tests (0.20 ± 0.03 vs 0.20 ± 0.04 miles or 321 meters; ri=0.88, p<0.0001), as was VO2 (11 ± 2 vs 11 ± 2 ml/kg/min; ri=0.92, p<0.0001). Only DBP did not show reproducibility (ri=0.33, p=ns). The Bland-Altman plots for the six-minute walk test using the Borg scale are shown in figures 2 and 3.
Intraclass Correlations Coefficients (ri) for six-minute cardiopulmonary walking test-related parameters
| Parameter | Test 1 | Test 2 | ri | p (ANOVA) |
|---|---|---|---|---|
| HR (bpm) | 96 ± 21 | 90 ± 19 | 0.96 | <0.0001 |
| VE (l/min) | 25 ± 05 | 25 ± 05 | 0.84 | <0.0001 |
| VO2 (ml/kg/min) | 11 ± 2 | 11 ± 2 | 0.92 | <0.0001 |
| SBP (mmHg) | 125 ± 20 | 119 ± 20 | 0.72 | 0.001 |
| DBP (mmHg) | 70 ± 12 | 69 ± 12 | 0.33 | Ns |
| Distance (miles) | 0.20 ± 0.03 | 0.20 ± 0.04 | 0.88 | <0.0001 |
| Slope VE/VCO2 | 32 ± 7 | 32 ± 6 | 0.86 | <0.0001 |
| RQ | 0.9±0.03 | 0.87±0.04 | 0.6 | 0.004 |
*Values are mean and SD. HR= heart rate; SBP= systolic blood pressure; DBP= diastolic blood pressure; VO2= oxygen consumption; RQ=respiratory quotient.
 and Distance (B)")
, Systolic (SBP) and Diastolic Blood Pressure (DBP)")

In this study, we tested the reproducibility of the 6CWT using the Borg scale proposed by Guimarães et al., 2002.6 The six-minute walk test’s guideline does not recommend a treadmill walk test because patients are unable to pace themselves.8 In our study, all patients were well-adapted to the method and were able to pace themselves. Studies with chronic obstructive pulmonary disease showed that the distance walked on a treadmill was less than the distance in a corridor.9,10 Following the [current?] guidelines, the patient’s instruction for the six-minute walk test was: “walk as far as you can.”11 A previous study demonstrated that the six-minute walk test could demand a higher exercise intensity than that achieved while performing daily activities (RQ>1.0) when the guideline’s standard recommendations are followed.6 The Borg scale is a valid measure of relative intensity, showing good correlation with heart and exercise rate.11
Some studies require the patient to become familiar with the six-minute walk test.12–14 A learning effect of 6% was reported in a cardiac rehabilitation population that completed the test on non-consecutive days.12 In our study, patients did not undergo familiarization, and it was not important for the reproducibility of the principal variables. There is no data available regarding the reproducibility of the six-minute-walk test using the Borg scale.
In our study, heart rate, systolic blood pressure and ventilation were reproducible. It is known that heart rate correlates with exercise intensity14, and we expected this reproducibility because exercise intensity has been standardized by the Borg scale. The reproducibility of the maximum cardiopulmonary test was studied previously24 and showed good reproducibility for both heart rate and ventilation at an anaerobic threshold and during a peak exercise test. In the present study, only diastolic blood pressure did not show reproducibility. No data are available about the reproducibility of ventilation, heart rate, systolic or diastolic blood pressure during the six-minute walking test.
All of our patients showed good RQ reproducibility, which remained less than 1.0 during the entire six-minute cardiopulmonary walking test. An RQ above 1.0 characterizes a tester near their maximum effort.13 In this study, our methodology assured a submaximal walking test. There are no available studies with six-minute cardiopulmonary walking tests showing RQ values. The American Thoracic Society Guidelines for the six-minute walk test11 recommend that patients should walk “as far as possible for 6 minutes” and recognize that patients “will probably get out of breath or become exhausted”, suggesting that a maximum exercise test can occur.
In our study, the VE/VCO2 slope showed good reproducibility. Previous studies showed that the VE/VCO2 slope predicts mortality and morbidity in heart failure patients who underwent a maximal cardiopulmonary test.14–16 In the 6CWT, this variable is correlated with distance and also predicts mortality and morbidity in patients with primary pulmonary hypertension.14 There is no data available about the VE/VCO2 slope during the six-minute walk test in heart failure patients. Reproducibility of the VE/VCO2 slope at an anaerobic threshold was investigated in a maximal cardiopulmonary test and showed a good correlation.15
In our study, VO2 at the sixth minute showed good reproducibility. This result could be important in meta-analysis studies because VO2 could be accessed without the influence of a physical therapist’s encouragement. Peak oxygen consumption is the standard measurement to evaluate exercise capacity and is a powerful predictor of mortality in heart failure patients.16–18 The six-minute walk test distance in heart failure patients correlated with peak O2 consumption and could predict peak VO2 in advanced heart failure patients.30 The Centers for Disease Control and Prevention recognize submaximal activities as 3 to 6 METs, which corresponds to moderate intensity for most young to middle-age adults.9 In our study, the METs average was less than 3.2. Once again, our methodology assured a submaximal walking test. The reproducibility of the peak VO2 at anaerobic threshold and during a maximum cardiopulmonary test was investigated, and a good correlation was found.24
Walking distance showed good reproducibility in our study. This could be important to evaluate the walking distance in meta-analysis studies without the influence of a physical therapist’s encouragement. Previous studies showed that the distance walked during the six-minute walk test strongly predicts mortality and morbidity.16,16,17 A walked distance of less than 300 meters predicts death or hospital admission for inotropic or mechanical bridging to transplantation in a period of six months.18 Excess encouragement significantly increased the walked distance19, which is why we standardized it with the Borg scale. A study evaluated heart failure patients (n=233) three times: two times within an interval of 30 minutes and another one day after. The tests were performed in a hospital corridor (34 meters of length) with previous familiarization, and all of the exams were very reproducible.15 Another study evaluated the distance covered during the six-minute walk test one year after the original test in 1,077 heart failure patients using a 15-meter corridor. The distance correlated with self-perceived symptom changes, as evaluated by a questionnaire. The authors concluded that the distance is sensitive to changes in self-perceived symptoms of heart failure; when the self-perception does not change, the distance walked is reproducible.16
LIMITATIONSThis study was limited by both the number and gender of available patients, although our data showed reproducibility of the most important variables for the 6CWT. Prognosis based on distance should have a different cutoff point than the previously mentioned 300-m cutoff point. More studies with a greater number of heart failure patients (including females) are necessary for a better comprehension of the 6CWT using the Borg scale.
CONCLUSIONThe 6CWT using the Borg scale in heart failure patients was reproducible and assured a submaximal walking test. These results suggest that our methodology may be appropriate for evaluating functional capacity in heart failure patients. However, more studies are necessary for better comprehension.