


DOPPS 3 shows a high incidence of malignancies in dialysis patients. The main meta-analysis shows a higher IR for cancer than the general population, especially in patients with age <35 years; patients are identified with ESRD-related and other immune deficiency-related malignancies: the former has a RR of 4 in dialysis and renal transplantation, the latter has RR of 1.5 in dialysis but 5 in renal transplantation. The importance of immunosuppression for transplanted patients is stressed. Our experience: we examined 255 patients on chronic dialysis from 2001 to 2009; we identified a case of asymptomatic carcinoid tumor. A 45-year-old woman, underwent gastro-duodenal endoscopy for pre-transplant kidney screening; we detected a duodenal polyp:histological examination showed the presence of cells of medium and uniform size with immunohistochemical reactivity for chromogranin, neuron-specific enolase and synaptophysin. According to guidelines, the patient was suspended for two years from waiting list. Then she repeated diagnostic exams with normal results. Finally she was included in waiting list. We examine the literature regarding carcinoid tumors in patients on chronic dialysis or kidney transplant. We highlight the importance of common diagnostic tests for the prevention of malignancies in patients on chronic dialysis.
El estudio Dialysis Outcomes and Practice Patterns Study (DOPPS) demuestra una elevada incidencia de tumores malignos en pacientes sometidos a diálisis. El metaanálisis principal demuestra una tasa de incidencia (TI) de cáncer mayor que en la población general, en especial entre pacientes <35 años de edad; se identifican algunos tumores malignos relacionados con la nefropatía terminal y otros relacionados con inmunodeficiencia: los primeros se asocian a un riesgo relativo (RR) de 4 en pacientes sometidos a diálisis y trasplante renal, y los segundos con un RR de 1,5 en pacientes sometidos a diálisis pero de 5 en los sometidos a trasplante renal. Se destaca la importancia de la inmunosupresión en pacientes sometidos a trasplante. Los autores describen su experiencia: se examinaron 255 pacientes sometidos a diálisis crónica desde 2001 a 2009; se identificó un caso de tumor carcinoide asintomático. Una mujer de 45 años de edad, se sometió a endoscopia gastroduodenal para un examen de cribado pretrasplante renal; detectamos un pólipo duodenal: el examen histológico demostró la presencia de células de tamaño medio y uniformes con reactividad inmunohistoquímica para la cromogranina, enolasa específica de neurona y sinaprofisina. De acuerdo con las guías, se suspendió a la paciente de la lista de espera durante 2 años. Acto seguido, se repitieron los exámenes diagnósticos obteniéndose un resultado normal. Por último, se incluyó en la lista de espera. Examinamos los estudios publicados sobre tumores carcinoides en pacientes sometidos a diálisis crónica o trasplante renal. Destacamos la importancia de efectuar los exámenes diagnósticos habituales para la prevención de tumores malignos en pacientes sometidos a diálisis crónica.
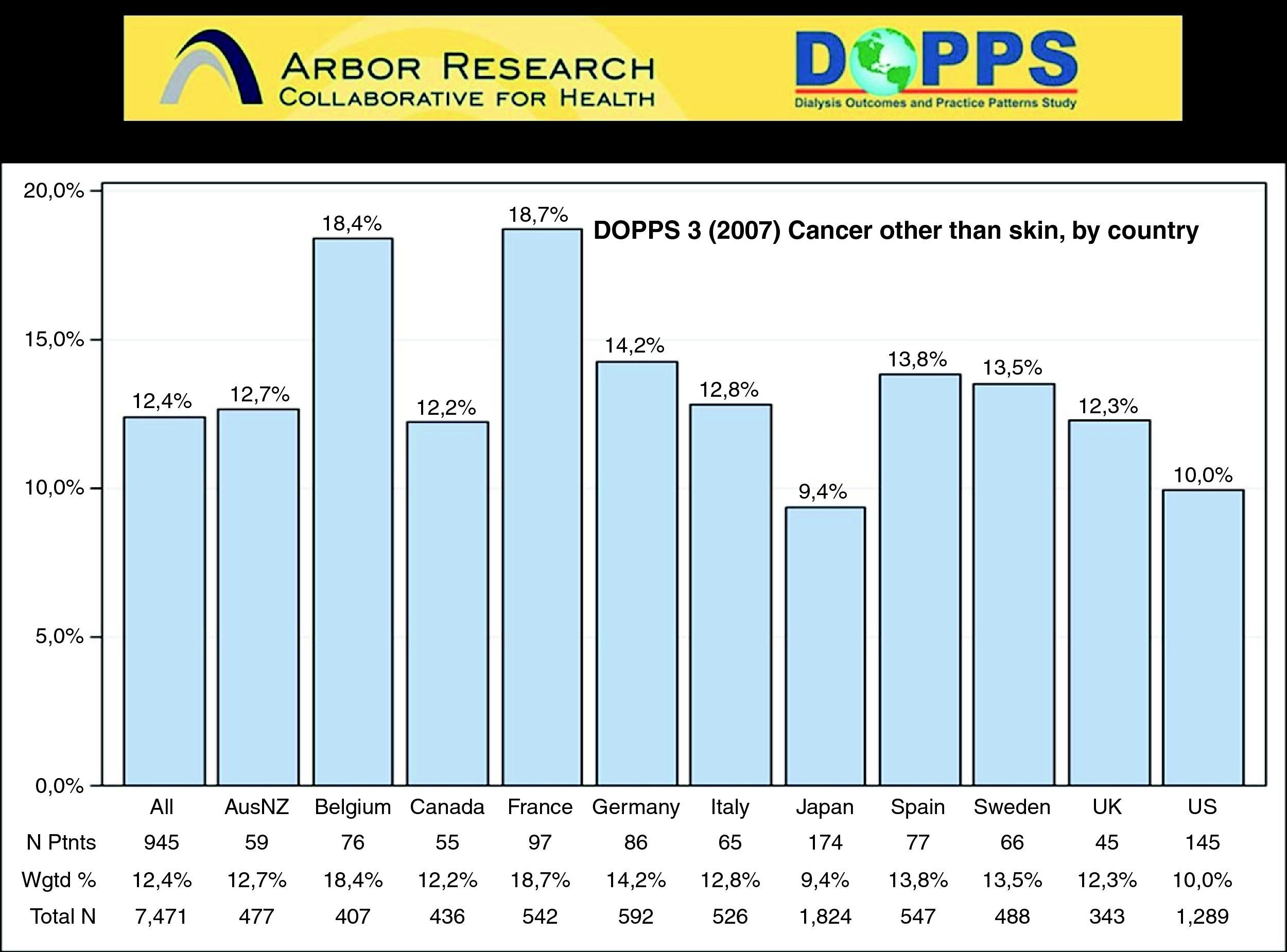
According to the DOPPS 3 (Fig. 1) the prevalence of malignancies in patients with ESRD1 has a growing importance. The people on chronic dialysis should be considered a cohort of high risk and therefore be subject to screening. However, unlike other cohorts of the general population, for patients on dialysis treatment there are no studies validated in a position to assess the benefit of certain diagnostic tests. Therefore the guidelines issued on this topic are adapted from those of the general population. There are several reports of individual cases but a few reviews in this topic. In 1999 a meta-analysis of Maisonneuve2 examined 831,804 patients on dialysis from 1980 to 1994 in the USA, Europe, Australia and New Zealand in a follow-up period of 2.5 years, identified 25,044 cases of malignant disease with a prevalence of 3% and incidence risk (IR) 1.18, detected a higher risk of cancer in patients younger than 35 years (IR 3.68) and the risk gradually reduces with increased age. Increased risk was observed for kidney cancer (3.60), bladder (1.50), thyroid and other endocrine organs (2.28). The incidence of cancer against lung, colorectal, prostate, breast and stomach was not significantly increased. In 2005 in Germany Jauch and Fischereder examined 382 renal transplant candidates and identified the presence of 45 malignant tumors in 38 patients: 20 cases (44%) were charged to the urinary tract, the total prevalence of malignancies was 9.9%.3 In 2009 a meta-analysis of Stewart about 28,885 patients on chronic dialysis from 1982 to 2003 in Australia, examined the cancer ESRD-related (kidney, urinary tract, thyroid, and myeloma) and those related to immune deficiency (non-Hodgkin's lymphoma and Hodgkin's lymphoma, melanoma, and s. Kaposi): compared with the general population the former shows an increase of four times both in dialysis and renal transplantation, the latter has an IR of 1.5 in dialysis but 5 in renal transplant.4 We report our experience. We reviewed the medical records of 255 patients in chronic dialysis treatment from 2001 to 2009 (145 haemodialysis and 110 peritoneal dialysis). We identified that 35 subjects were included in waiting list for kidney transplant. They were subjected to the most common screening tests (skin examination, PAP test, mammography, abdominal ultrasound, and endoscopy). We encountered a case of asymptomatic carcinoid tumor. A 45-year-old woman, born in Sri Lanka, was on haemodialysis for 1 year because of a post-partum HUS, underwent gastro-duodenal endoscopy screening for renal transplantation. Before the examination she had suffered from epigastralgia, and improved with dialysis and medication. The endoscopy showed an erosive gastro-duodenitis and a proximal duodenum sessile polyp with a diameter of 2mm, which was removed. The gastro-duodenal echo-ultrasound endoscopy, the echocardiogram and the chest and abdomen CT scan were of no pathological elements. The histological examination revealed the presence of cells of medium and uniform size with immunoreactivity to chromogranin, to neuron-specific enolase (NSE) and to synaptophysin. Octreotide scintigraphy did not show any abnormal uptake. Blood level of chromogranin-A was increased: 460U/l (nv 2–18), while NSE and other routine laboratory tests were within normal range. For Helicobacter Pilory positivity she received antibiotic therapy. Afterwards she repeated the same diagnostic tests without any pathological outcome. According to the guidelines,5 the patient was suspended for two years from the waiting list for kidney transplant. Serial blood levels of Chromogranin-A remained unchanged. Then the patient was referred back to endoscopy with normal results and finally included in the active list. In literature we have identified three reports of four cases of carcinoid tumor in patients on chronic dialysis. In the first of these, the patient had a typical carcinoid syndrome (flushing and watery diarrhea) and liver metastases,6 in another report there was no description of the cases.7 We reviewed the reports of carcinoid discovered after kidney transplantation. In 1983, Spees8 reported 6 cases in 1028 renal transplants (0.58%). In 1999, Nemes described a primitive hepatic carcinoid diagnosed 86 days after kidney transplantation.9 In 2008 Odashima reported a rapid regression of multiple gastric carcinoids that was identified three months after renal transplantation.10 In 2008, Jin reported a case of rectal carcinoid tumor diagnosed 12 years after kidney transplantation.11 Patients on dialysis are at greater risk for various cancers, particularly those of the kidney and urinary tract because of carcinogenic events following to the primary kidney disease (tuberous sclerosis, ADPKD), biochemical or immunological alterations resulting in CKD or to the same dialysis treatment. We want to emphasize the asymptomatic carcinoid tumor in our patient and the importance of common diagnostic tests (annual skin examination, PAP test, ultrasound of urinary tract, and routine blood tests). Screening for the most common solid tumors (prostate, colon, breast and uterus cervix) should be individualized.
Conflict of interest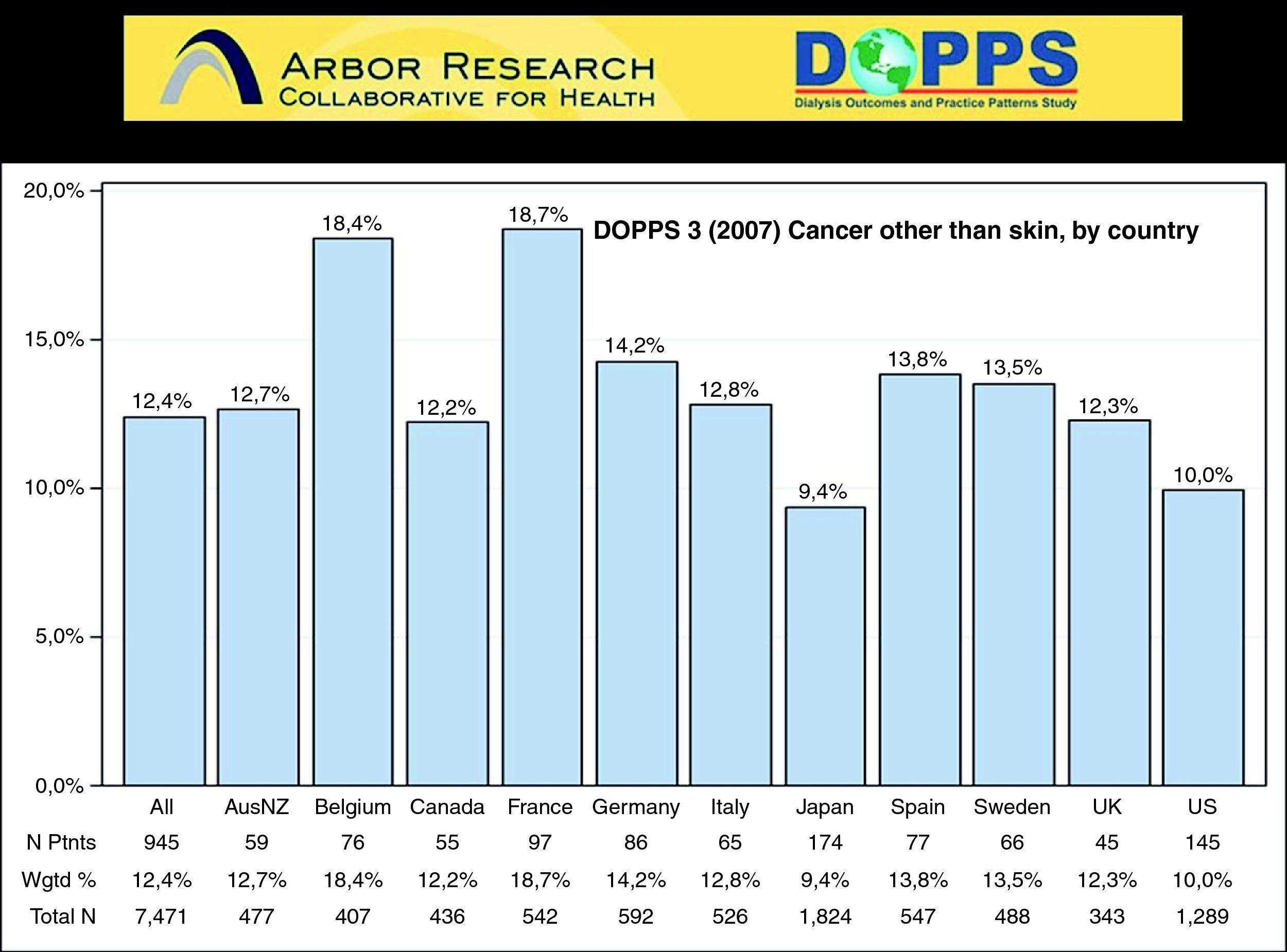
None declared.