




Psychological disorders and particularly depression are common in chronic renal failure and hemodialysis (HD) patients. These disorders have important influences on quality of life and increased mortality rate. This study was performed to evaluate the frequency of depression and its related factors among HD patients.
MethodsThe study population consisted of 120 patients on conventional maintenance hemodialysis who filled Beck's questionnaires in order to screening of depression. Data were collected by a questionnaire, medical history and laboratory findings. The SPSS v.16 was used for data analysis and Chi square and based on Spearman's tests were applied.
ResultsFrequency of depression among study population was 70% and 26.7% of them suffered from severe depression. There was no correlation between age; gender; underlying disease; HD duration; history of renal transplantation; marital status; occupation; hemoglobin; serum albumin levels and depression (p>0.05). Frequency of HD sessions per week and dialysis adequacy (Kt/V) significantly correlated with depression severity (p=0.01 and p=0.04).
ConclusionWith regard to high prevalence of depression among HD patients, depression screening seems necessary in this population. Early diagnosis and treatment of depression could improve patients’ quality of life.
En pacientes con insuficiencia renal crónica y sometidos a hemodiálisis (HD) son habituales los problemas psicológicos y en particular la depresión. Estos procesos tienen una importante influencia en la calidad de vida y aumentan la tasa de mortalidad. El presente estudio se efectuó para valorar la frecuencia de depresión y los factores relacionados entre pacientes sometidos a HD.
MétodosLa población del estudio consistió en 120 pacientes que recibían hemodiálisis de mantenimiento convencional y completaron cuestionarios de Beck para un examen de cribado de la depresión. Los datos se obtuvieron a través de un cuestionario, una anamnesis y los hallazgos de laboratorio. Para el análisis de los datos se utilizó el programa SPSS versión 16 y se aplicaron la prueba de la X2 y la de Spearman.
ResultadosLa frecuencia de depresión entre la población estudiada fue del 70%, y el 26.7% de pacientes experimentaba depresión grave. No se identificó una correlación entre la edad; sexo; enfermedad subyacente; duración de la hemodiálisis; antecedentes de trasplante renal; estado conyugal; profesión; hemoglobina; concentración sérica de albúmina y la depresión (p>0.05). La frecuencia de las sesiones de HD por semana y la adecuación de la diálisis (Kt/V) se correlacionaron significativamente con la gravedad de la depresión (p=0.01 y p=0.04).
ConclusiónCon respecto a la elevada prevalencia de depresión entre pacientes sometidos a HD, en esta población parece necesario un examen de cribado en busca de la enfermedad. El diagnóstico y tratamiento precoz pueden mejorar la calidad de vida de los pacientes.
Chronic debilitating diseases such as chronic renal failure and hemodialysis (HD) prescription have several psychiatric consequences. HD as a main therapeutic modality in end-stage renal disease (ESRD) is a stressful process associated with mental pressure and psychosocial problems.1 Although, the longevity of ESRD patients on hemodialysis is more, however, it results in many complications such as mental disorders in which depression occurs to most of them.2,3
Depression is considered as the fourth main cause of death in the world and at least 15% of general population may experience a depression episode.4 Furthermore, because of some somatic illnesses, and social and environmental factors; the frequency of depression is increasing particularly in chronic illnesses such as ESRD.5 Despite, depression is a common finding among HD population, the similarity of depression symptoms (e.g. reduced appetite; fatigue; impatience; sexual dysfunction and sleep disorders) with some somatic diseases, makes its diagnosis difficult. On the other hand, depression treatment encompasses a great expense compared to other diseases which may be attributed to non compliance of patients to treatment.6,7
Thus, it seems that early diagnosis and effective treatment of depression can improve quality of life and survival of HD patients.5 With this idea, the present study was conducted to determine the frequency of depression and its related factors among HD patients at the Mustafa Khomeini Hospital in Tehran, Iran.
Materials and methodsBeck Depression Inventory (BDI) questionnaire has been used for depression screening in HD patients with high sensitivity and specificity indices.8–13 Beck's questionnaire included 21 questions which evaluate the severity of depression and score it from 0 to 63. In HD patients, score above 10 is sufficient for the diagnosis of depression. Based on scores, depression is classified to mild depression (11–16); mild depression requiring consultation (17–20); moderate depression (21–30); severe depression (31–40) and extremely severe (41–63).8,9
The study population consisted of 120 subjects undergoing conventional maintenance HD (HD vintage>3 months) who referred to the Mustafa Khomeini Hospital from April 2008 to April 2010. None of the patients had experienced a psychiatrist consultation and antidepressant medication before HD prescription. All patients were informed of study purposes and consented. Blood samples were obtained for biochemical analyses including measurements of serum albumin, urea, creatinine and hemoglobin levels.
Urea is the main index of solute (soluble materials) removal and particularly reflects the clearance of small size uremic toxins. Several methods have been used for assessing the adequacy of hemodialysis which the most common ones are urea reduction ratio (URR) and Kt/V. In this study, single pool Kt/V, was calculated by Daugirdas formula14:
where R is the post-pre SUN (serum urea nitrogen) ratio, t is session length (in hours), UF is the volume of fluid removed during dialysis (in liters) and W is post dialysis body weight (in kilograms). Pre- and post dialysis (immediately at the end of dialysis) blood samples were drawn to obtain respective serum urea concentrations, in order to calculate spKt/V. The minimum target dose of spKt/V which is recommended by Kidney Disease Quality Outcomes Initiative (K/DOQI) is 1.2.14 In order to calculate spKt/V, the post dialysis blood sample was drawn from arterial blood line 20s after dialysis session termination while the pump speed was reduced to 80mL/min.
URR which is expressed as percentage (K/DOQI recommendation>65%) was calculated by the following equation:

All data analyses were carried out using the SPSS v.16. Descriptive statistical results were extracted and the one-way ANOVA, Chi square, Spearman's and t-tests were used to show correlations between depression and other variables. p value<0.05 was considered statistically significant.
ResultsThe study population consisted of 120 referral HD patients (57% male and 43% female) who were between the ages of 23 and 80 years (mean value of 30.15±57.57 years). HD duration in the participants ranged from 6 to 60 months with mean of 5.42±3.36. Table 1 shows quantitative variables which were analyzed in this study.
Diabetes mellitus and hypertension were the most common underlying diseases (57.6% and 20.3%, respectively) in participants. Other data about qualitative variables are shown in Table 2.
Descriptive data of qualitative variables.
| Variables | Subgroups | Frequency (%) |
| Gender | Male | 57 |
| Female | 43 | |
| Underlying diseases | Diabetes | 57.6 |
| Hypertension | 20.3 | |
| Glomerulonephritis | 6.1 | |
| Poly cystic kidneys | 5 | |
| Idiopathic | 11 | |
| History of renal transplantation | 9.3 | |
| Marital status | Married | 76.6 |
| Single | 23.4 | |
| Occupation | Employed | 45 |
| Unemployed | 55 | |
| Frequency of HD sessions/week | 3 times | 87.3 |
| <3 times | 12.7 |
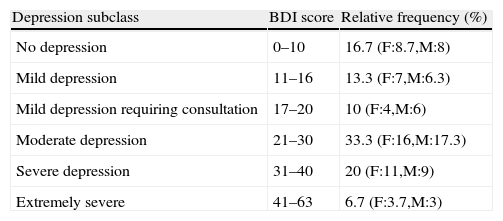
The mean score of BDI in HD patients was obtained as 23.37±11.05. This study revealed that 70% of the participants were depressed. Table 3 shows the relative frequency of depression subclasses, based on BDI scores or disease severity among HD patients.
Relative frequency of depression subclasses based on BDI scores.
| Depression subclass | BDI score | Relative frequency (%) |
| No depression | 0–10 | 16.7 (F:8.7,M:8) |
| Mild depression | 11–16 | 13.3 (F:7,M:6.3) |
| Mild depression requiring consultation | 17–20 | 10 (F:4,M:6) |
| Moderate depression | 21–30 | 33.3 (F:16,M:17.3) |
| Severe depression | 31–40 | 20 (F:11,M:9) |
| Extremely severe | 41–63 | 6.7 (F:3.7,M:3) |
F:females; M:males.
There was no statically significant correlation between age; gender; underlying disease; HD vintage; history of renal transplantation; marital status; employment status; hemoglobin; serum albumin and depression (p>0.05). The frequency of HD sessions per week and HD adequacy (Kt/V) significantly correlated to depression severity (BDI score) and frequency (p=0.01 and p=0.04, respectively), so that Kt/V increment was accompanied with low BDI score (depression severity) while increased frequency of HD sessions had detrimental effect on depression.
DiscussionPsychiatric disorders including mood disorders, depression, organic brain disease, schizophrenia and personality disorders in patients with chronic illnesses such as ESRD are very common.2 Psychiatric disorders increase rate of hospitalization in HD patients compared with other chronic diseases and lead to higher mortality.2 These disorders result in more hospitalization of HD patients compared to peritoneal dialysis patients that may be attributed to patient selection for a particular type of dialysis prescription or increased prevalence of behavioral disorders leading to hospitalization in HD patients.2 However, it seems that the type of dialysis prescription has no significant influence on depression symptoms; sexual disorders and life satisfaction.15 Depression in ESRD patients, independently of the HD adequacy, can impact on mortality rate. The exact prevalence of depression in HD patients is unknown and ranges from 10 to 66%.11 This wide range may be attributed to various criteria which are used to assess mood disorders. Furthermore, some patients may extremely emphasize on their physical symptoms and deny any affective disorders or other depression related symptoms.11 On the other hand, depression is more common in the Caucasian race and prior unfamiliarity with dialysis prescription and depression may also exist at the beginning of dialysis prescription. There are conflicting information about depression and survival rate.16,17 This study revealed that 70% of the study population on maintenance hemodialysis suffered from some degrees of depression and 26.7% had severe depression. However, in recent years the prevalence of depression in HD patients in other studies has been reported considerably less than our finding, nearly 28–38.7%.18,19 Lower prevalence of depression in these patients may be related to the high dialysis adequacy due to high efficient HD filters which have better performance, nocturnal home hemodialysis prescription (6–7 times a week) and good compliance of the cases to continue the therapeutic course.
As mentioned above, gender; age; underlying disease; HD vintage; marital status; employment status; history transplantation; hemoglobin and serum albumin levels had no correlation with depression. Some investigators have got similar findings,5 but some have not. For instance, gender; age and diabetes correlated with depression in some studies.20 In addition, a cohort study indicated that physical illness and female gender are considered as depression risk factors.21 In our study, factors such as frequency of HD sessions per week and Kt/V had influences on depression. Hemodialysis sessions of 3 times/week or more were associated with more severe depression (higher BDI score), a finding that has confirmed by some other researches.22 Although, HD patients must be dialyzed at least 9–12h/week (3 times a week) in order to remove uremic toxins from their bodies which is unavoidable, and even newer methods of nocturnal home hemodialysis increase this time to seven times/week, however this fact also could not be denied that the frequency of movement to HD units and its difficulties especially for debilitated HD patients is very stressful and results in depression. Nocturnal home hemodialysis as a new promising technique has largely resolved these problems; however this technique is very expensive and there are few facilities to employ it for all patients. Considering the inevitability for the time spent on HD in our country, it seems that providing more facilities for traffic of HD patients; selection of close HD centers to patients’ homes; increasing the number of HD units in our country and improving the adequacy of HD by employing the high efficient HD filters and bicarbonate (as dialysis solution) dialysis instead of acetate, could be appropriate measures to reduce psychiatric disorders in HD patients.
With regard to the high prevalence of depression among HD patients, screening of depression using the BDI questionnaire seems to be necessary. People with high depression scores in this screening need to get further evaluation and appropriate therapeutic measures by a psychiatrist. Improved dialysis and risk factor elimination can play roles in reducing the prevalence of mental disorders such as depression in HD patients. On the other hand, adequacy of HD as a prognostic index is dependent on a variety of factors such as patient size, protein intake, HD duration and type of equipment used in the process of HD. We recommend further studies with more samples in order to better clarify the prevalence of psychiatric disorders in HD patients.
Conflicts of interestThe authors declare no conflicts of interest.