




The activity of an Endocrinology and Nutrition (E&N) department consists of inpatient care both by those attached to the department and through consultations with specialists from other departments. The inpatient care activity of all the E&N departments of a public health system has not been studied in Spain.
Material and methodsThis was a retrospective study of hospital ward activity during 2018 of the E&N departments of the Castilla-La Mancha Public Health Service. It was undertaken in order to ascertain the characteristics of the patients attended to, both by those in charge of the E&N departments and through interconsultation with other departments, as well as the case-mix of the pathology of these patients. All patients admitted to E&N and a 10% sample of those treated through interconsultation were analysed.
Results261 admissions were recorded for Castilla-La Mancha Public Health Service E&N departments. 82.8% were urgent and 53.7% were due to type 1 diabetes mellitus. A total of 5955 patients were seen on an interconsultation basis, 591 of whom were analysed. The most frequent reason for interconsultation was diabetes mellitus/hyperglucemia (28.8%), requiring 6.1±6.7 days per patient. However, interconsultations for artificial nutrition required more days of attendance per patient and accounted for a higher percentage of the total number of days of interconsultation (60.4%).
ConclusionsThe inpatient care activity of the E&N departments of Castilla-La Mancha Public Health Service mainly consists of attending to patients with chronic pathologies of high hospital prevalence such as diabetes mellitus/hyperglucemia and, especially, clinical nutrition.
La actividad de los servicios de Endocrinología y Nutrición (EYN) incluye la asistencia en planta de pacientes propios o mediante interconsultas. La actividad asistencial en planta del conjunto de servicios de EYN de un sistema público de salud no ha sido estudiada en nuestro país.
Material y métodosEstudio retrospectivo de la actividad en planta de hospitalización durante 2018 de los Servicios de EYN del Servicio Público de Salud de Castilla-La Mancha para conocer las características de los pacientes atendidos, tanto con carácter de interconsulta como ingresados a cargo de los propios servicios, así como la casuística de la patología de dichos pacientes. Se analizaron todos los pacientes ingresados a cargo de EYN y una muestra del 10% de los atendidos como interconsulta.
ResultadosSe registraron 261 ingresos a cargo de los servicios de EYN del Servicio Público de Salud de Castilla-La Mancha. El 82,8% tuvieron carácter urgente y el 53,7% fueron por diabetes mellitus tipo 1. Se atendieron 5955 pacientes en régimen de interconsulta, de los cuales se analizó una muestra de 591. El motivo de interconsulta más frecuente fue la diabetes mellitus/hiperglucemia (28,8%), requiriendo 6,1±6,7 días por paciente. Sin embargo, las interconsultas para nutrición artificial requirieron más días de asistencia por paciente y supusieron un porcentaje mayor del total de días de interconsulta (60,4%).
ConclusionesLa actividad en planta de los servicios de EYN del Servicio Público de Salud de Castilla-La Mancha se basa en la asistencia de pacientes con patologías crónicas de alta prevalencia hospitalaria como la diabetes mellitus/hiperglucemia y, especialmente, la Nutrición Clínica.
Endocrinology and Nutrition is the branch of Medicine that studies the physiology and diseases of the endocrine system, the metabolism of nutritional substances, natural and artificial nutrition, health promotion through the prevention of diet-related diseases, and the corresponding diagnostic, therapeutic and preventive techniques used in these areas of medical knowledge.1
Endocrinology and Nutrition Departments in turn have care, teaching, management and research functions. Patient care activity is carried out both in hospital (inpatients and day hospital patients) and in the outpatient area through the endocrinology and nutrition outpatient clinics.1 The hospital ward attends patients admitted by the Endocrinology and Nutrition Departments with diseases specific to the specialty, as well as patients admitted under the supervision of other Departments that perform interconsultations for the management of endocrine or nutritional comorbidities.
The Endocrinology and Nutrition Ward Care Activity in Castilla-La Mancha (Actividad Asistencial en Planta de Endocrinología y Nutrición en Castilla-La Mancha [AAPENCAM]) study was sponsored by the Sociedad Castellano-Manchega de Endocrinología, Nutrición y Diabetes, and was designed to determine the characteristics of the hospitalized patients attended by the Endocrinology and Nutrition physicians of the Regional Health Service of Castilla-La Mancha (Servicio de Salud de Castilla-La Mancha [SESCAM]) – both in the context of interconsultation and admitted by the Departments themselves – as well as the diseases seen in these patients.
Material and methodsThe AAPENCAM was a retrospective cross-sectional study that analyzed the hospital ward activity of the Departments of Endocrinology and Nutrition of the public hospitals of Castilla-La Mancha between 1 January and 31 December 2018.
On one hand, an analysis was made of all patient admissions under the charge of the Endocrinology and Nutrition Departments of the SESCAM, and on the other, an analysis was carried out of a random sample of patients seen on an interconsultation basis during hospital admission.
Study variablesFor each patient admitted under the charge of the Endocrinology and Nutrition Departments, we documented patient age and gender, whether admission was on an emergency or scheduled basis, whether the patient died during admission, the total days of hospital stay, the days of admission under the charge of the Endocrinology and Nutrition Department, and up to two diagnoses as the cause of admission.
With regard to the patients attended on an interconsultation basis, we recorded age and gender, the total number of working days of patient care, and up to two reasons for consultation from a predetermined list including diabetes mellitus/hyperglycemia, other endocrine disorders, parenteral nutrition, enteral nutrition, and other types of nutritional support or assessment. For each reason for interconsultation, the number of working days dedicated to the consultation was recorded. In the case of patients in whom the reason for care was the prescription of parenteral nutrition, the management of hyperglycemia/diabetes mellitus was not considered an additional reason. In any other reason for interconsultation, if patient hyperglycemia/diabetes mellitus was moreover also managed, it was considered a second reason. In patients for whom two interconsultation reasons were recorded, their order of priority was left to the investigators’ discretion. When these reasons for care were successive, the number of days of care coincided with the sum of the days spent on each of the reasons. However, when two reasons applied simultaneously, the sum of the days spent on each of them was greater than the total days of care. In some patients, the total days of care was greater than the sum of the days corresponding to the two documented reasons, because they were also seen for a third reason that was not tabulated.
Statistical analysisThe statistical analysis was carried out using R software, version 3.5.2,2 through the integrated development environment Rstudio.3
The results of the patients seen on an interconsultation basis are expressed, in the case of proportions, as a percentage along with the corresponding 95% confidence interval (95%CI). In the case of patients admitted under the charge of the Endocrinology and Nutrition Departments, the confidence interval of the proportions was not calculated, since all admissions were recorded.
Age, in years, was analyzed as a continuous variable, and its result was expressed as the mean and standard deviation (SD). Gender, the number of reasons for interconsultation or of admission per episode and, in the case of patients admitted under the charge of the Endocrinology and Nutrition Department, whether admission was scheduled (elective) or on an emergency basis, were reported as percentages. These percentages were expressed, where applicable, together with the corresponding 95% confidence interval, calculated using the epi.conf function of the epiR version 1.0-2 package.4
With regard to the diagnoses, for the patients admitted under the charge of the Endocrinology and Nutrition Departments, an analysis was made of the proportion of the different diagnoses recorded as first diagnosis and as second diagnosis, expressed as percentages. For the patients seen on an interconsultation basis, we calculated the percentage of the different reasons for interconsultation – both the first reason and second reason, and the overall reasons, regardless of the order in which they were recorded. For each of them we calculated the corresponding 95% confidence interval, using the MultinomCI function of the DescTools version 0.99.28 package.5 In addition, for the total days of interconsultation, we calculated the percentage of days dedicated to each of the interconsultation reasons using the wpct function of the Weights version 1.0 package,6 followed by estimation of the confidence interval using the MultinomCI function.
With the main diagnosis, in the patients admitted under the charge of the Endocrinology and Nutrition Departments, and with the overall interconsultation reasons regardless of the order in which they were collected, for the patients seen on an interconsultation basis, we calculated age and the proportion of women for each diagnosis or reason for interconsultation.
Sample selection and sizeThe analysis of the patients admitted under the charge of the Endocrinology and Nutrition Departments involved all patients admitted during 2018; no sample was therefore used.
The analysis of those patients seen on an interconsultation basis was performed using a sample. Although the way in which this care modality is registered differs among the hospitals participating in the study, in all of them we were able to obtain a list of patients seen in 2018 on an interconsultation basis with Endocrinology and Nutrition. A random sample of this list of patients was selected from each hospital. In most centers and patients it proved possible to stratify randomization per Department in charge of the admitted patient, or at least to stratify whether interconsultation was due to an endocrinological cause or for nutritional treatment or assessment.
The sample size was calculated through simulation using the MultinomCI function of the DescTools package, in order to secure a confidence interval of under ±5% in the proportions of the first reasons for interconsultation. In this regard, we considered a population of 6000 interconsultations and the total of 5 possible reasons for care. A sample of 600 patients was found to be needed for analysis; a random sample of 10% of the total patients seen during the year on an interconsultation basis was therefore selected in each center. If a given patient experienced multiple admissions over the year on an interconsultation basis, the case was considered to correspond to a single process.
ResultsPatients admitted under the charge of the Endocrinology and Nutrition DepartmentsDuring 2018, a total of 261 admissions occurred in 6 of the Endocrinology and Nutrition Departments of the SESCAM (Complejo Hospitalario Universitario de Albacete, Hospital Virgen de la Luz de Cuenca, Hospital General Universitario de Ciudad Real, Hospital Universitario de Guadalajara, Hospital Nuestra Señora del Prado de Talavera de la Reina and Complejo Hospitalario de Toledo), of which 120 corresponded to women (46.0%). The patient age (mean±standard deviation [SD]) was 41.0±19.5 years, with an interquartile range (IQR) of 22.7–55.4 years. The age range was 7.0–93.7 years.
Of the total admissions, 216 (82.8%) were of an emergency nature, and in only four of the admission episodes (1.5%) were two diagnoses coded. In the year of the study, no patients died during admission under the charge of an Endocrinology and Nutrition Department in the hospitals of the SESCAM.
The hospital stay was 4.7±5.0 days, with a median of four days, an interquartile range of 2–5 days, and a range of 0–59 days. The duration of stay in the Endocrinology and Nutrition Department was 4.0±4.5 days, with a median of three days, an interquartile range of 2–5 days, and a range of 0–59 days.
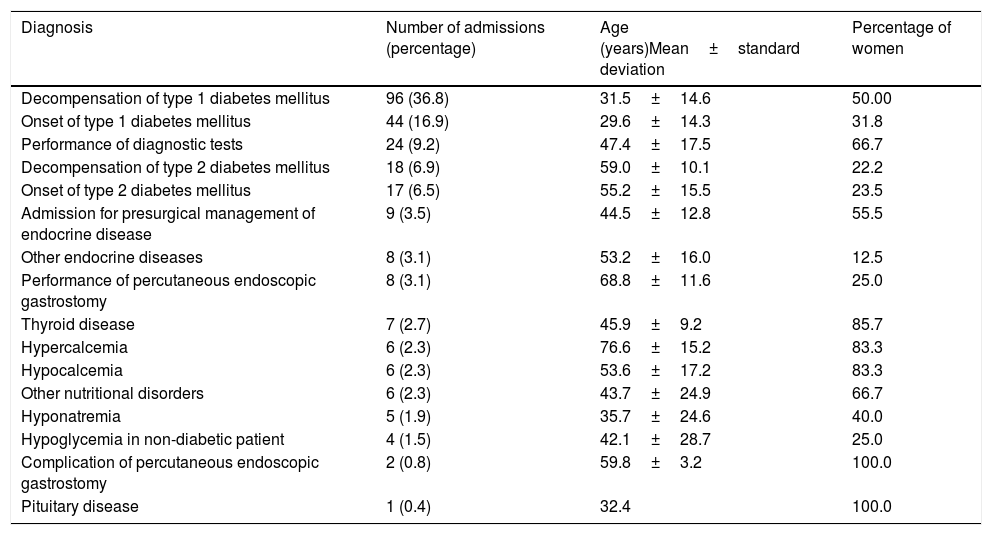
Admission due to type 1 diabetes mellitus, secondary to decompensation of already known diabetes disease or to the onset of the disease, was by far the most common cause of admission. Table 1 shows the data corresponding to the main diagnosis of the patients. Of the four admissions in which a secondary diagnosis was recorded, two involved autoimmune thyroid disease in patients with onset of type 1 diabetes mellitus, while the other two involved other unspecified endocrine disorders. Table 1 also shows the age and gender of the patients admitted according to each of the disorders.
Main diagnoses among the patients admitted under the charge of the Endocrinology and Nutrition Departments, and age and gender of the patients according to diagnosis.
| Diagnosis | Number of admissions (percentage) | Age (years)Mean±standard deviation | Percentage of women |
|---|---|---|---|
| Decompensation of type 1 diabetes mellitus | 96 (36.8) | 31.5±14.6 | 50.00 |
| Onset of type 1 diabetes mellitus | 44 (16.9) | 29.6±14.3 | 31.8 |
| Performance of diagnostic tests | 24 (9.2) | 47.4±17.5 | 66.7 |
| Decompensation of type 2 diabetes mellitus | 18 (6.9) | 59.0±10.1 | 22.2 |
| Onset of type 2 diabetes mellitus | 17 (6.5) | 55.2±15.5 | 23.5 |
| Admission for presurgical management of endocrine disease | 9 (3.5) | 44.5±12.8 | 55.5 |
| Other endocrine diseases | 8 (3.1) | 53.2±16.0 | 12.5 |
| Performance of percutaneous endoscopic gastrostomy | 8 (3.1) | 68.8±11.6 | 25.0 |
| Thyroid disease | 7 (2.7) | 45.9±9.2 | 85.7 |
| Hypercalcemia | 6 (2.3) | 76.6±15.2 | 83.3 |
| Hypocalcemia | 6 (2.3) | 53.6±17.2 | 83.3 |
| Other nutritional disorders | 6 (2.3) | 43.7±24.9 | 66.7 |
| Hyponatremia | 5 (1.9) | 35.7±24.6 | 40.0 |
| Hypoglycemia in non-diabetic patient | 4 (1.5) | 42.1±28.7 | 25.0 |
| Complication of percutaneous endoscopic gastrostomy | 2 (0.8) | 59.8±3.2 | 100.0 |
| Pituitary disease | 1 (0.4) | 32.4 | 100.0 |
In the course of 2018, a total of 5955 hospitalized patients were seen on an interconsultation basis by the Endocrinology and Nutrition Departments/Sections/Units of Complejo Hospitalario Universitario de Albacete, Hospital La Mancha-Centro de Alcázar de San Juan, Hospital General de Almansa, Hospital General Universitario de Ciudad Real, Hospital Virgen de la Luz de Cuenca, Hospital Universitario de Guadalajara, Hospital Comarcal de Hellín, Hospital Nuestra Señora del Prado de Talavera de la Reina, Complejo Hospitalario de Toledo and Hospital General de Villarrobledo. Of these patients, a sample of 591 was analyzed in the present study. Registry problems precluded the inclusion of cases from another district hospital with approximately 60 patients seen on an interconsultation basis during the mentioned study period.
A total of 43.5% (39.7–47.3) of the patients were women. The mean age (±standard deviation [SD]) was 64.1±17.3 years, with a median of 66.5 years and an interquartile range (IQR) of 54.8–77.0 years.
In relation to interconsultation, the patients seen for diabetes mellitus/hyperglycemia were 63.9±16.3 years old, and 42.1% (35.3–49.1) were women. Those seen for other endocrine disorders were 59.0±18.3 years old, and 53.8% (43.7–63.6) were women. Those seen for the prescription of parenteral nutrition were 68.0±16.0 years old, and 40.4% (32.9–48.8) were women. Those seen for the prescription of enteral nutrition were 69.6±13.1 years old, and 40.3% (32.1–49.1) were women. Lastly, those seen for other nutritional support or assessment were 60.7±18.3 years old, and 48.5% (40.0–57.0) were women.
A single healthcare reason was recorded in 82.7% (79.9–85.8) of the cases, while two were recorded in the rest of cases. Patient care lasted 8.3±10.2 days, with a median of 5 days and an interquartile range of 2–10 days.
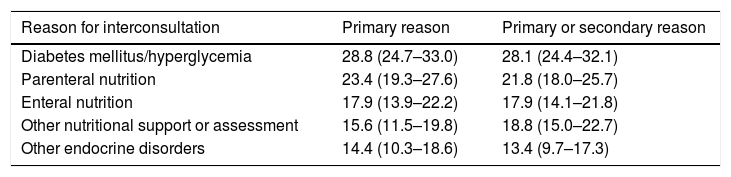
The most common reason for interconsultation among the 591 patients was diabetes mellitus/hyperglycemia, followed by parenteral nutrition, whether considered to be the main reason or any reason for interconsultation. Table 2 shows the data referred to the reasons for interconsultation: both those cases recorded as the primary reason and those in which primary or secondary reason was not taken into account.
Distribution of reasons for interconsultation, expressed as percentage with 95% confidence interval (95%CI).
| Reason for interconsultation | Primary reason | Primary or secondary reason |
|---|---|---|
| Diabetes mellitus/hyperglycemia | 28.8 (24.7–33.0) | 28.1 (24.4–32.1) |
| Parenteral nutrition | 23.4 (19.3–27.6) | 21.8 (18.0–25.7) |
| Enteral nutrition | 17.9 (13.9–22.2) | 17.9 (14.1–21.8) |
| Other nutritional support or assessment | 15.6 (11.5–19.8) | 18.8 (15.0–22.7) |
| Other endocrine disorders | 14.4 (10.3–18.6) | 13.4 (9.7–17.3) |
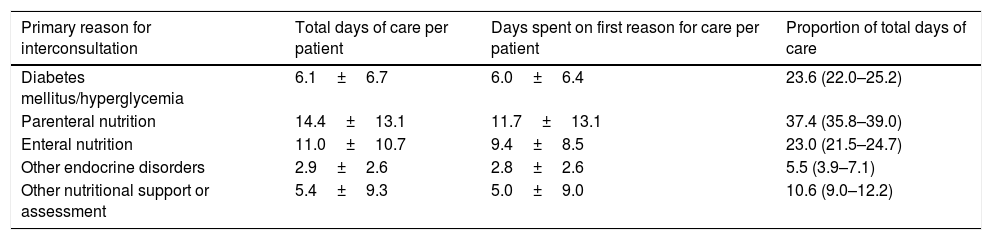
The 591 patients analyzed required a total of 4925 days of care. Although diabetes mellitus/hyperglycemia was the most common reason for interconsultation, parenteral and enteral nutrition required longer care times per patient. Accordingly, of the total days of interconsultation-based care among the endocrinologists of Castilla-La Mancha during 2018, parenteral nutrition was the reason for which most days of care were required (Table 3).
Days dedicated to care on an interconsultation basis per patient.
| Primary reason for interconsultation | Total days of care per patient | Days spent on first reason for care per patient | Proportion of total days of care |
|---|---|---|---|
| Diabetes mellitus/hyperglycemia | 6.1±6.7 | 6.0±6.4 | 23.6 (22.0–25.2) |
| Parenteral nutrition | 14.4±13.1 | 11.7±13.1 | 37.4 (35.8–39.0) |
| Enteral nutrition | 11.0±10.7 | 9.4±8.5 | 23.0 (21.5–24.7) |
| Other endocrine disorders | 2.9±2.6 | 2.8±2.6 | 5.5 (3.9–7.1) |
| Other nutritional support or assessment | 5.4±9.3 | 5.0±9.0 | 10.6 (9.0–12.2) |
Days dedicated to care on an interconsultation basis per patient according to the primary reason for interconsultation expressed as mean±standard deviation (SD) and proportion of total days of care dedicated to each primary reason for interconsultation reported as percentage and 95% confidence interval (95%CI).
To the best of our knowledge, this is the first multicenter study on the clinical activity in hospitalized patients of specialists in Endocrinology and Nutrition referred to the global Spanish Regional Health System.
The number of admissions under the charge of the Endocrinology and Nutrition Departments of the SESCAM was not particularly notorious when compared to the number of patients seen on an interconsultation basis. This is due on one hand to the fact that most endocrine and nutritional disorders can be managed on an outpatient basis, and on the other to the fact that not in all SESCAM hospitals do the Endocrinology and Nutrition Units/Sections/Departments have specifically assigned beds for admissions. As a result, patients admitted with disease corresponding to the specialty of Endocrinology and Nutrition are admitted under the charge of other Departments such as Internal Medicine (a circumstance also sometimes seen in hospitals with beds assigned to Endocrinology and Nutrition when patient admission is decided by physicians on duty who are not endocrinologists).
In this regard, it should be noted that more than half of the admissions under the charge of Endocrinology and Nutrition were due to type 1 diabetes mellitus, in the form of either acute decompensation of the disease or the onset of diabetes. The DIACAM 1 study analyzed a cohort of 1465 patients with type 1 diabetes mellitus aged 16 years or older and seen in 2009–2010 in the Endocrinology and Nutrition outpatient clinics of all the healthcare areas of Castilla-La Mancha; this cohort was estimated to represent one-third of all type 1 diabetics in Castilla-La Mancha.7 Although the mentioned study did not analyze newly diagnosed patients or those not attending control visits, the DIACAM 1 trial allows the placing in context of the 140 patients admitted under the charge of Endocrinology and Nutrition due to type 1 diabetes mellitus in the analyzed hospitals of Castilla-La Mancha during 2018 – 96 of them due to decompensation of already known type 1 diabetes mellitus – since the DIACAM 1 trial gives us an idea of the prevalence of type 1 diabetes in Castilla-La Mancha, and the number of admissions due to decompensation must be related to it.
Regarding interconsultations, more than a quarter of the total were due to hyperglycemia or diabetic decompensation. The prevalence of diabetes mellitus/hyperglycemia in hospitalized patients is very high. One study reported that 12.9% of all hospital discharges in Spain in 2007 included a diagnosis of diabetes mellitus,8 and in this regard prevalence rates of 12–26% have been reported in the United States.9 Previous studies of the Sociedad Castellano-Manchega de Endocrinología, Nutrición y Diabetes have reported a 33.5% prevalence of hyperglycemia or known diabetes mellitus among hospitalized patients in Castilla-La Mancha,10 with a progressive increase in the number of discharge reports reflecting the diagnosis of diabetes mellitus.11
Although diabetes mellitus/hyperglycemia was the main reason for interconsultation when considering the predefined list on which the recording of such reasons was based, nutritional support and assessment overall accounted for 56.9% of the interconsultations and for 68.3% of the total days of care. The PREDYCES study reported a prevalence of malnutrition among hospitalized patients of 23.7%, with increased hospital stay and costs associated to malnutrition.12 If the prevalence of diabetes mellitus/hyperglycemia and malnutrition among hospitalized patients may be of similar magnitude, the fact that twice as many consultations were made for nutritional support and assessment as were made for the management of hyperglycemia may be due to fact that endocrinologists are familiarized with nutritional support techniques, such as artificial nutrition, which are not usually used by other specialists. In contrast, many patients with hyperglycemia are managed by non-endocrinologists exclusively based on “fast insulin regimens” – despite the fact that these have been shown to contribute to poor blood glucose control13 – without interconsultation with Endocrinology and Nutrition.
A weakness of our study regarding analysis of the interconsultation activity is its retrospective design, analyzing a sample representing approximately 10% of the total patients seen on an interconsultation basis. The diverse methods for recording interconsultation activity in the different centers precluded the use of exactly the same type of stratification in randomization in all centers. However, considering that in most of them stratification could be made either according to interconsultation due to an endocrinological or nutritional causes, or the Department in charge for the patient, we feel that the results are representative of the interconsultation activity of Endocrinology and Nutrition in the SESCAM.
The RECALSEEN study revealed the existence of differences in Endocrinology and Nutrition activity among different Spanish Regional Health Systems14; our results therefore do not necessarily have to be comparable to those of other region (Autonomous Communities) in the country. However, our methodology is applicable to studies that may be conducted in other Autonomous Communities or even referred to the whole of Spain.
As a strength of our study, it is the first to analyze the hospital ward clinical activity of specialists in Endocrinology and Nutrition corresponding to virtually all the hospitals in a Spanish Regional Health System.
In sum, the present study shows that in the hospital ward, most of the activity of Endocrinology and Nutrition corresponds to interconsultations referred to patients admitted under the charge other Departments. Endocrinologists deal with highly prevalent diseases that increase hospital stay and costs, such as diabetes mellitus/hyperglycemia and, very particularly, malnutrition. This explains the fact that much of the growth of our specialty in recent years has taken place in the field of Clinical Nutrition.14 In any case, both as regards the management of diabetes mellitus/hyperglycemia and in relation to malnutrition, there is much work to be done in hospitalized patients, and the leading role in this respect falls upon the specialists in Endocrinology and Nutrition.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Albacete: Alejandro Esteban Sirvent Segovia, Antonio Moya Moya, María del Carmen López García. Alcázar de San Juan: Cristina Contreras Pascual, Álvaro García Manzanares Vázquez de Agredos, Paloma González Lázaro, Francisco Javier Gómez Alfonso. Ciudad Real: Belén Fernández de Bobadilla, Miguel Aguirre Covisa. Cuenca: Mubarak Alramadan Aljamalah, David Martín Iglesias, José Pérez Rodríguez, Javier González López. Guadalajara: Visitación Álvarez de Frutos, Marta Cano Megías, Sandra Herranz Antolín. Talavera: Benito Blanco Samper, Petra de Diego Poza, Iván Quiroga López, Miguel Ángel Valero González. Toledo: Bárbara Cánovas Gaillemin, Ofelia Llamazares Iglesias.
Please cite this article as: Alfaro-Martínez J-J, Peña-Cortés V-M, Moreno-Fernández J, Platero-Rodrigo E, Calderón-Vicente D-M, Gómez-García I-R, et al. Actividad asistencial en planta de Endocrinología y Nutrición en Castilla-La Mancha (estudio AAPENCAM). Endocrinol Diabetes Nutr. 2020;67:665–671.

recomendados