


To study the potential associations among circulating insulinlike growth factor 1 (IGF-1) and adrenal and gonadal steroids with cognitive status and depression in a group of independently-living elders.
DesignPopulation-based cross sectional study.
MethodsA total of 313 individuals (160 women and 153 men, with a mean age of 76.7±7 years) participated in this study. A physical examination, assessment of functional capacity, cognitive function, depression, educational level and measurement of plasma cortisol, dehydroepiandrosterone (DHEA) and its sulphate (DHEAs), testosterone, estradiol, and IGF-1 were performed.
ResultsIn women, adrenal steroids showed a negative correlation with global cognition (β=−0.79; p=0.03 for DHEA and β=−0.27; p=0.002 for cortisol). A positive correlation with IGF-1 (β=0.026; p=0.04) was found for cognition in women after adjustment for depression. For memory function, DHEA correlated negatively but no relationship with IGF-1 and cortisol was observed. No relationships with cognition were observed in men for any of the steroids or other hormones studied. Educational level showed the highest protective effect (odds ratio [OR] = 6.25) for preserved cognition for both sexes; in women, OR for deteriorated cognition with age, DHEA and cortisol were 1.14, 1.57 and 1.09, respectively. No associations between depression and hormonal profile were found in either sex.
ConclusionsEducational level was positively associated with cognitive function in independently-living elderly men and women, while adrenal steroids were associated with impaired cognition in elderly women but not in men. The hormonal milieu seemed to have little or no influence on depression in the men and women studied.
Estudiar la posible relación del factor de crecimiento insulinoide tipo 1 (IGF-1) y los esteroides adrenales y gonadales con la función cognitiva y estado depresivo en un grupo de personas ancianas no dependientes.
DiseñoEstudio transversal de base poblacional.
MétodosParticiparon 313 individuos (160 mujeres y 153 varones, con una media de edad de 76,7±7 años). Se practicó un examen físico, evaluación de la capacidad funcional, estado cognitivo y estado depresivo, se registró su grado académico y se midió cortisol, deshidroepiandrosterona (DHEA) y su sulfato DHEAs, testosterona, estradiol y el factor de crecimiento insulinoide tipo 1 (IGF-1) en plasma.
ResultadosEn mujeres, los esteroides adrenales presentaron una correlación negativa con la función cognitiva general (β=−0,72; p=0,05 para DHEA y β=−0,15; p=0,004 para cortisol); hubo correlación positiva entre función cognitiva general e IGF-1 (β=0,04; p=0,02) tras ajustar por estado depresivo; no hubo correlación entre función de memoria e IGF-1 y cortisol. En los varones no hubo correlaciones entre esteroides adrenales e IGF-1 y función cognitiva. El nivel académico mostró el máximo efecto protector para una función cognitive preservada (odds ratio [OR]=6,25) en ambos sexos; en las mujeres la OR para el deterioro cognitivo fue de 1,14 para la edad, 1,57 para DHEA y 1,09 para cortisol. No se observaron asociaciones de las distintas hormonas estudiadas y estado depresivo en ninguno de los dos sexos.
ConclusionesHay asociación positiva del estado cognitivo con el nivel académico en personas ancianas no dependientes de ambos sexos, y en las mujeres pero no en los varones, los esteroides adrenales se asociaron también a un peor estado cognitivo; no se apreciaron influencias de las concentraciones de hormonas estudiadas en el estado depresivo de los sujetos estudiados de cualquier sexo.
Among healthy elderly individuals there is a considerable variation in the effects of age on physiological functions, with some people showing an important and accelerated decline and some others exhibiting a high resistance to this process. Continuous decline of certain hormonal systems throughout the lifespan has been related to the loss of function that characterizes the aging process; in particular, diminution of adrenal steroids in relation to dehydroepiandrosterone (DHEA) and its sulphate (DHEAs)/cortisol ratios, circulating sexual steroids and growth hormone (GH), have been claimed to be associated with poor cognitive status, depression and decreased functional performance in elderly people1-3. However, heterogeneous results have been recently reported by different studies4,5 leading to a much difficult understanding of the aging process and its associated diseases; also, accompanying diseases of elders and their treatments do not facilitate how to define the frontier between physiology and pathophysiology of aging and can themselves influence hormonal status6. Moreover, normative data in relation to hormones in elders are just beginning to get a consensus by clinicians7 and the diagnosis and treatment of certain hormonal defects in aged people are still a matter of debate, as late-onset male hypogonadism8.
This paper reports the results of the cross-sectional part of the Mataró Aging Study in which a sample of 313 old people are enrolled; investigations were carried out to clarify the potential relationship between sexual, adrenal and somatotropic hormones with mood status and cognitive function.
SUBJECTS AND METHODSIndividuals of both sexes aged more than 70 years living in the neighbourhood of Cirera-Molins in Mataró and the nearby village of Argentona, north to Barcelona, were randomly selected and invited to participate in a longitudinal study with the aim of defining factors influencing frail or robust condition while aging. From the municipal census, 16% of the population of both areas was older than 70; after contacting the target individuals, a total of 313 persons, 13.5% of the original population of 2304, accepted to participate in the study. Persons living in nursing homes, mentally or physically disabled did not participate in the study; main inclusion criterion was that individuals were able to come to the clinical research center by themselves. From these 313, 160 were women and 153 men; mean age was 77.3 ± 6.4 and 76.7 ± 5.4 years (76.7 ± 7 for the total group; range, 71-102 y); the general characteristics of the participants have been described elsewhere9; cardiovascular risk factors were highly prevalent in both women and men with diabetes mellitus (22.6% and 19.7%), hypercholesterolemia in 64.5% and 51.4%, hypertension in 56.7% and 49.3%, ischemic heart disease in 9.7% and 17.8% and previous stroke in 13.5% and 11.2% respectively, and most of them were taken medications for these conditions; however, none of these treatments influenced the relations described in this paper. Most of the individuals received primary and secondary education (54%) but did not have a university degree. The study was approved by the Ethics Committee of the Hospital de Mataró.
MeasurementsHormonal measurementsBlood samples were drawn in the morning after an overnight fasting. Hormonal measurements were performed by commercial validated immunoassay kits, and included: free testosterone (reference range [RR] men: 9-41pg/ml; women: 0,2-3,2pg/ml; Immunotech, Marseille Cedex, France), estrone (RR men: 30-90pg/ml; women: 20-40pg/ml; DSL, Webster, Texas, USA); dehydroepiandrosterone (DHEA) (RR men: 1,5-9ng/ml; women: 0,7-2,1ng/mL; Immunotech, Marseille Cedex, France) and DHEA sulphate (DHEAs) (RR men: 50-560μg/dl; women: 35430μg/dl; Immunotech, Marseille Cedex, France), insulin-like growth factor-1 (IGF-1) (RR men: 49-250ng/ml; women: 49-250ng/ml; Nichols Institute, San Clemente, CA, USA), and IGF binding protein 3 (IGFBP3) (RR 1,08-4,26μg/ml, Biocode, Liége, Belgium); LH (RR men: 2-12 mUI/ml; women: 10-62 mUI/ml) and FSH (RR men: 2-12 mUI/ml; women: 5-60 mUI/ml) (Advia Centaur, Bayer Diagnostics, Spain), cortisol (RR: 5-25μg/dl) (Immulite 2000, Diagnostics Product Corporation [DPC], Los Angeles, CA, USA) and GH (RR: 0,1-5ng/ml; Immulite 2000, Diagnostics Product Corporation [DPC], Los Angeles, CA, USA).
Physical performance and functional capacityPhysical performance was assessed by the balance unipodal test which consists in evaluating the capacity to stand with only one foot during 5 seconds (item 9 of the Tinetti test). Functional capacity was assessed by calculation of Barthel10 and the validated Spanish version of the Modified Stanford Health Assessment Questionnaire11. Nutritional status evaluated by performing the reduced form of Mini Nutritional Assessment test (MNA).
Mental status and depressionMental status was measured by the Mini Mental State Examination (MMSE)12 and depressive status by performing the 5 items Geriatric Depression Scale (GDS-5)13.
Data analysisStatistical descriptive analyses were performed expressing categorical data as percentages and continuous data as means and standard deviations. All analyses were performed separately for men and women. To compare proportions by gender or other categorical variables a chi square test or a Fisher's exact test was used. The correlations between hormone concentrations, mental and depressive status, and functional capacity measurements were done using the Pearson or Spearman correlation coefficient (r or rs). For further study of the relationship between these variables an initial univariate analysis was carried out by using a linear regression. A multivariate regression analysis was additionally performed to adjust the effects of the variables showing an association in the univariate analysis with mental status, depressive state or functional capacity with a p value < 0.20. Statistical significance was considered when the p value was < 0.05.
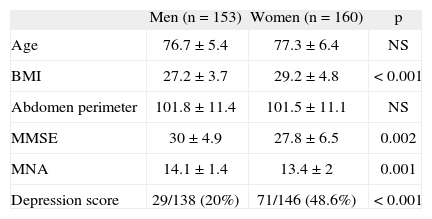
RESULTSDescriptive data of the physical characteristics, as well as age, body mass index (BMI) and abdominal perimeter are shown in table 1. According to the MNA, 1.4% of men and 6.2% of women were at risk of malnutrition (p = 0.061); moreover, both males and females showed a high degree of overnutrition, as mean BMI was above normality in either sex. This tendency to obesity was paralleled by elevated abdominal perimeter, with no differences in absolute values between sexes.
Descriptive data of the study sample
| Men (n = 153) | Women (n = 160) | p | |
| Age | 76.7 ± 5.4 | 77.3 ± 6.4 | NS |
| BMI | 27.2 ± 3.7 | 29.2 ± 4.8 | < 0.001 |
| Abdomen perimeter | 101.8 ± 11.4 | 101.5 ± 11.1 | NS |
| MMSE | 30 ± 4.9 | 27.8 ± 6.5 | 0.002 |
| MNA | 14.1 ± 1.4 | 13.4 ±2 | 0.001 |
| Depression score | 29/138 (20%) | 71/146 (48.6%) | < 0.001 |
BMI: body mass index; MMSE: Mini Mental State Examination; MNA: Mini Nutritional Assessment; NS: p ≥ 0.05.
A notable difference in depressive status was found according to gender after GDS evaluation, as 71 out of 146 women showed depressive scores (48.6%) in comparison to 29 out of 138 men (21%); there were no changes in GDS scores with older ages. According to MMSE, 22 women (15.3%) and 10 men (7.3%) had moderate impairment in cognitive status, 14 women (9.7%) and 9 men (6.6%) had mild impairment and the rest had a normal cognitive function (108 [75%] women and 118 [86%] men); MMSE results showed a negative correlation with age (rs = –0.27; p < 0.001). Physical activity, measured as outdoor self-reported walking hours per day, was 0.87 hours/day in women and 1.56 hours/day in men (p < 0.001).
Relations of hormones concentrations with age and correlations between hormonesIn women, DHEA and DHEAs showed a decrease with age (rs = –0.17; p = 0.037 and rs = –0.16; p = 0.048 respectively), while free testosterone, estradiol and estrone, IGF-I, IGFBP3 and IGF-I/IGFBP3 ratio did not show changes in the age range studied (71-102 year old). In men, a decrease with age was only observed in testosterone (rs = –0.19; p = 0.025) with no changes in the rest of hormones.
No differences were found in mean values of any of the hormones studied between obese and non- obese individuals; how ever, BMI showed a positive correlation with TSH (rs = 0.11; p = 0.05) and a strong negative correlation with SHBG (rs = -0.10; p < 0.001) for the hall group. In men, BMI correlated with IGF-I (r = 0.17; p = 0.03) and statistical significance was almost reached with free testosterone (r = –0.15; p = 0.07). In women, LH and estradiol correlated with BMI (r = –0.19; p = 0.01, and r = 0.16; p = 0.04, respectively) as well as with SHBG (rs = –0.23; p = 0.004) and TSH (rs = 0.22; p = 0.005).
Estrogens were higher in men than in women, either estradiol (48.7 ± 14.7 vs 32.1 ± 12.7; p < 0.05) and estrone (42.9 ± 21.4 vs 27.9 ±16.1; p < 0.05). Testosterone showed a positive association with estradiol in men (β = 0.33; p < 0.001) but not in women. IGF-I did correlate with IGFBP-3 in both sexes.
Relations between hormones, cognition and depressive statusNo relationship was observed in men with any of the steroids and other hormones studied with cognition and mood, while cognitive function in women showed a negative relationship with DHEA (β = –0.72; p = 0.05), cortisol (β = –0.15; p = 0.004) and a positive correlation with IGF-1 (β= 0.04; p = 0.02). In women, cognitive function also showed a relationship with academic degree (β = 3.4; p < 0.001) after adjustment for depressive status (GDS score). Academic degree also correlated with cognitive function in men (β = 0.37; p < 0.001) and women (β = 0.51; p < 0.001). These results in women were also observed when the memory items of the MMSE were separately analysed, with persistence of the negative association of DHEA, although IGF-1 and cortisol lost their statistical significance.
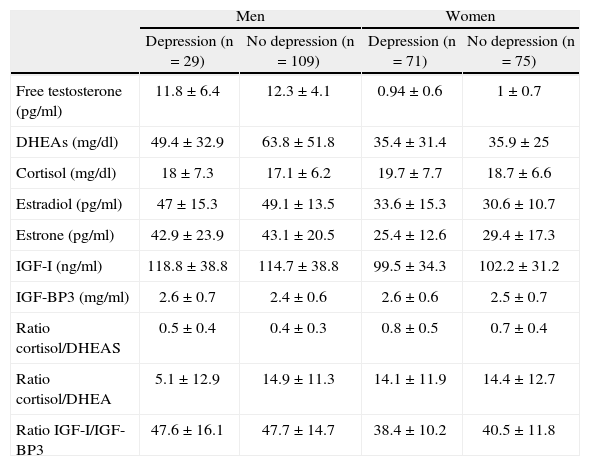
When a multivariate logistic regression analysis (that included age, academic level, DHEA and cortisol in the model) was performed, the academic degree showed the maximal protective effect (OR = 6.25) for preserved cognitive status in both sexes. In women, OR for deteriorated cognition for age, DHEA and cortisol were 1.14, 1.57 and 1.09, respectively, all statistically significant. No associations were observed between DHEAs and any of the variables evaluated. Furthermore, no associations for depression and any of the other hormones studied were found in either men or women (table 2).
Steroids and IGF-I concentrations and depressive status
| Men | Women | |||
| Depression (n = 29) | No depression (n = 109) | Depression (n = 71) | No depression (n = 75) | |
| Free testosterone (pg/ml) | 11.8 ±6.4 | 12.3 ±4.1 | 0.94 ± 0.6 | 1 ±0.7 |
| DHEAs (mg/dl) | 49.4 ± 32.9 | 63.8 ±51.8 | 35.4 ±31.4 | 35.9 ± 25 |
| Cortisol (mg/dl) | 18 ±7.3 | 17.1 ±6.2 | 19.7 ±7.7 | 18.7 ±6.6 |
| Estradiol (pg/ml) | 47 ±15.3 | 49.1 ± 13.5 | 33.6 ±15.3 | 30.6 ± 10.7 |
| Estrone (pg/ml) | 42.9 ± 23.9 | 43.1 ± 20.5 | 25.4 ± 12.6 | 29.4 ± 17.3 |
| IGF-I (ng/ml) | 118.8 ±38.8 | 114.7 ±38.8 | 99.5 ± 34.3 | 102.2 ±31.2 |
| IGF-BP3 (mg/ml) | 2.6 ± 0.7 | 2.4 ± 0.6 | 2.6 ± 0.6 | 2.5 ± 0.7 |
| Ratio cortisol/DHEAS | 0.5 ± 0.4 | 0.4 ± 0.3 | 0.8 ± 0.5 | 0.7 ± 0.4 |
| Ratio cortisol/DHEA | 5.1 ± 12.9 | 14.9 ±11.3 | 14.1 ± 11.9 | 14.4 ± 12.7 |
| Ratio IGF-I/IGF-BP3 | 47.6 ±16.1 | 47.7 ±14.7 | 38.4 ±10.2 | 40.5 ±11.8 |
DHEA: dehydroepiandrosterone; DHEAs: dehydroepiandrosterone sulphate; IGF-I: insulin-like growth factor-1; IGF-BP3: IGF binding protein 3.
Neither in men, nor in women, the differences of hormones included in the study were statistically significant between depressive and non depressive subjects.
In this population of independently living old men and women, we found an expected decline in global mental function and certain hormones with age. A considerable percentage of women, about half of the sample –the double of men-, showed a depressive mood score with no remarkable changes in relation to age. Also, a similar situation was seen in relation to cognition with more women showing cognitive dysfunction in either category explored (global and memory items of the MMSE) in comparison to men. The endocrine system may influence the dynamics of aging, and reciprocally, changes in the synthesis and metabolism of different families of hormones are determined and timed by age6. In our study, it was also shown that estrogens exposure is higher in old men than in old women, because of a continuous conversion of testosterone to estrogens in peripheral tissues from testosterone; testosterone and estradiol depicted a high positive correlation in men. Therefore, overall, men are under a more prolonged gonadal hormonal exposure during the lifespan than women. This fact may have implications for physical, mental and mood performance when comparisons between sexes are considered, and mostly in terms of frail and robust condition. DHEA and its sulphate remain the main gonadal prohormone in women, with a potential of conversion to either androgen or estrogenic pathway, but always at a considerably low absolute level than that observed in men. A remarkable debate has been raised in the last decade in relation to potential beneficial effects of supplementation with DHEAs to old women, with the aim to achieve circulating levels in the range of younger women; an overexposure to this steroid would theoretically encompass a much similar aged masculine hormonal milieu. The fact is that no consistent results have yet been obtained19 that justify giving support to long-term supplementation with this steroid in the general population of old women27; by now, it is just recommended as substitutive treatment for young women with primary adrenal insufficiency, in which an improvement of self esteem, mood and general well being have been recently described20. Despite this lack of a formal recommendation DHEAs is available in some countries without medical prescription. Our results do not support that DHEA is associated to better cognition, mood or physical performance; moreover, we found that DHEA, as well as cortisol were associated to an impaired global cognitive function and DHEA to a lower memory performance in old women; other studies have shown that overexposure to cortisol is associated to cognitive impairment14,15. Kalmijn et al16 did not find a relationship between either cortisol or DHEAs and cognition, although a relationship was found with the cortisol/DHEAs ratio and mental impairment, in which a higher ratio was associated to an impaired cognitive performance. DHEA itself has been proposed as a neuroprotective steroid, but most of the information was raised in experimental models in which DHEA has been considered as a natural counteractive factor of cortisol, the latter being believed to have increasing neurotoxic actions at the hippocampus and other relevant sites of the central nervous system when DHEA is decreasing as a consequence of aging22,23. We did not find any relationship between cortisol/DHEA ratio and cognitive or memory performance in our cohort of women. More than cortisol, or the ratio cortisol/DHEAs, the relevant factor maybe the individual sensitivity or resistance to circulating cortisol according to some specific polymorphisms of the glucocorticoid receptor gene17,18. Conversely, it maybe hypothesized that DHEA was elevated in those women with impaired cognitive function as part of a reactive and/or protective mechanism, but the cross-sectional nature of our report do not allow us to establish causal relationships of these findings.
Also remarkable is that no relationship in terms of hormonal status and cognition was evident in our men cohort.
The most prominent factor associated to a good cognitive status was academic degree, with much higher OR than any other biological factors considered, and in both genders; the other factor accounting for cognitive impairment was age itself. Therefore, although the hormonal changes seen in aging maybe of some importance, non-hormonal factors are the driving factors determining the cognitive status of “healthy” old persons.
Somatotropic axis activity was also weakly associated to better cognitive scores in women, a fact that has also been reported in other studies in men28; this may be due to some neuroprotective actions of GH and IGF-I26. In old men, substitutive treatment with GH and/or testosterone has shown contradictory results in mood changes2,24-26. In our cohort, men seemed to be overall exposed to more factors associated to better psychophysical condition, with better academic degree, more hours per day of exercise, and higher levels of somatotropic axis activity and sexual hormones but significant statistical associations were not found.
We did not find any relationship between depressive status and adrenal or sexual steroids in men and women when analysed separately, although the double of women in relation to men had depressive scores and the overall gonadal hormones, both androgens and estrogens were much higher in men; it is difficult to elucidate whether these gender differences of elderly mood may be influenced by these different hormonal profiles. A lack of statistical power of our study may the cause, as other studies with more individuals have shown a positive relationship of testosterone and less depression in men29. Finally, it has to be remarked that our study was performed with the information obtained by a single determination of hormones in which the sample was drawn during the morning hours; this may have a potential influence in certain hormonal axis, as the corticotropic axis, and interpretation of our findings should be done taking into account these considerations.
In conclusion, our study indicates that in independent living old people, gonadotropic, somatotropic and adrenal axis may contribute to some extent to changes in cognitive status that characterize aging condition in particular in women; however, non-hormonal factors, such as academic together with age per se maybe much more relevant driving elements.
We thank Cristina Mas for technical assistance in the preparation of the manuscript.
The Mataró Aging Study Group: Ayllón J, Boquet X, Bosch A, Burdoy E, Cadenas I, Dordas J, Espinosa C, Falcón I, Gordillo M, Merino MJ, Mussoll J, Palomera E, Papiol M, Pous E, Pubill M, Puig J, Puig-Domingo M (codirector), Sanahuja J, Serra P, Serra-Prat M (codirector), Serrano C, Vilardebò A, Villarroya I.
