


Ovarian carcinoid tumors are extremely rare tumors very frequently occurring on a cystic teratoma. They may develop carcinoid syndrome in the absence of liver metastases by avoiding enterohepatic circulation.
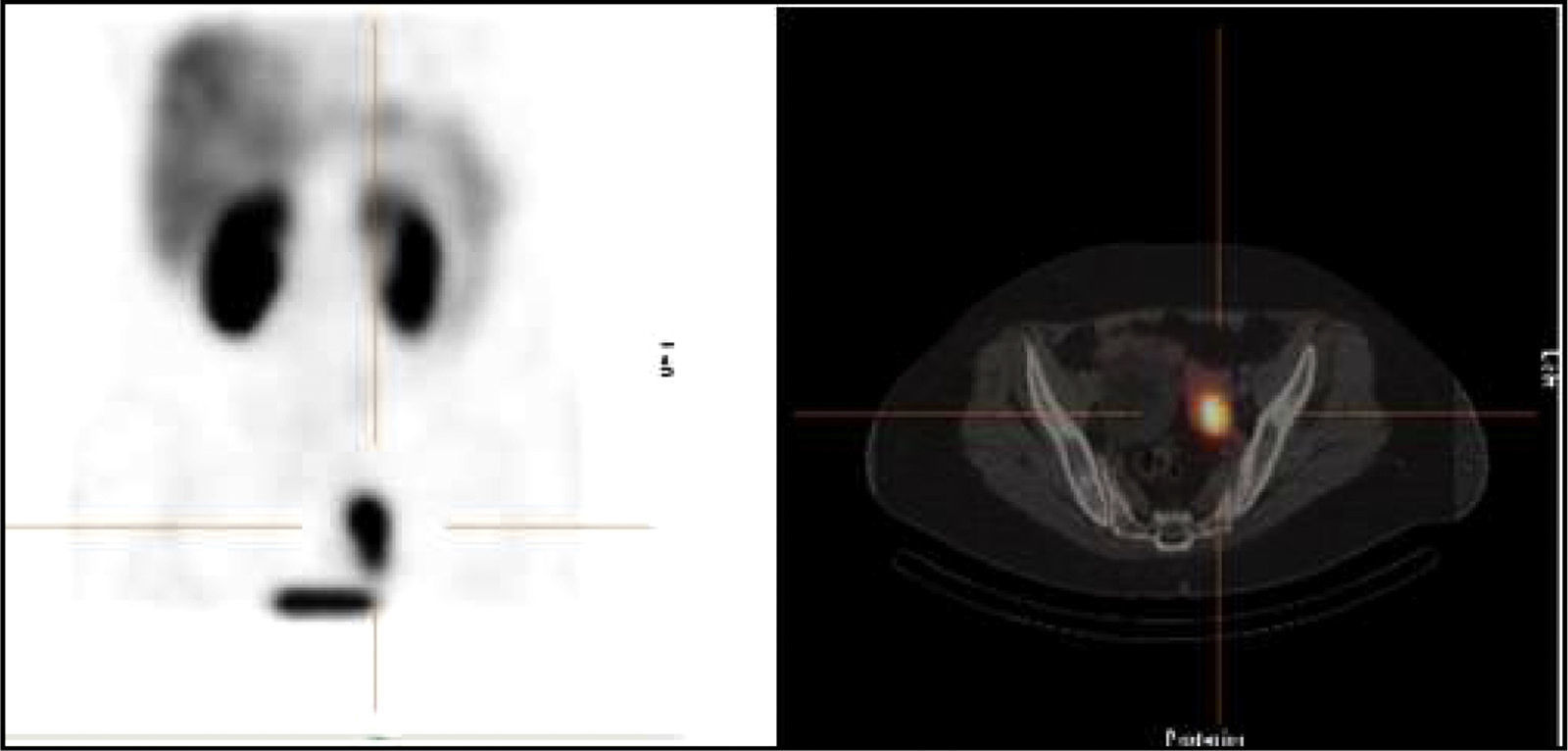
We report the case of a 59-year-old female patient with history of high blood pressure controlled with enalapril and gastroesophageal reflux on long-term treatment with omeprazole and cinitapride who reported almost daily episodes of facial flushing starting two years before. Episodes were self-limited, lasted approximately 5–10min, followed no time pattern, and were not related to drug or food intake. They were not associated to high or low blood pressure, headache, diarrhea, or bronchospasm, but patient reported palpitations during them. Patient differentiated these episodes from the vasomotor symptoms she had previously experienced after menopause at 52 years of age. These symptoms included a generalized hot sensation not associated to sweating or facial erythema which spontaneously resolved at 55 years (two years before the start of current symptoms). The patient reported no associated constitutional symptoms. Physical examination findings were normal. Measurement of calcitonin levels in blood and metanephrines, normetanephrines and 5-hydroxyindoleacetic acid in urine was requested. Repeatedly high 5-hydroxyindoleacetic acid levels were found, together with a mild, discontinuous elevation in normetanephrines (Table 1). Calcitonin levels were normal. Based on these findings, chromogranin A was tested in plasma, and a value of 265ng/mL (No.<134) was reported. Based on the suspicion of a carcinoid tumor, a computed tomography (CT) scan and magnetic resonance imaging of the chest and abdomen were performed, showing a 6cm right adnexal lesion reported as a possible teratoma. On the other hand, transabdominal pelvic ultrasonography revealed a 3.5cm×4cm tumor related to the left ovary. Because of heterogeneity of the results, a 111In-Pentetreotide scan (Octreoscan®) was requested, showing a tracer hyperuptake site in the left paramedial pelvic region (Fig. 1). In order to relieve symptoms while planning surgery, treatment was started with a somatostatin analogue (lanreotide 60mg every 28 days by the deep subcutaneous route), which decreased the frequency and severity of episodes. After ruling out cardiac valve involvement by echocardiography, bilateral adnexectomy was performed. Histological examination found a low-grade (G1) insular carcinoid tumor on a mature cystic teratoma in left adnexum with Ki-67 1–2%, low mitotic index, and positive staining for chromogranin and synaptophysin in immunohistochemistry. The right ovary had a mature teratoma with no associated carcinoid tumor. After surgery, flushing episodes disappeared, and 5-hydroxyindoleacetic acid and normetanephrine levels normalized. Octreoscan® and CT performed six months after surgery were normal. Although serum chromogranin A levels markedly decreased, values remained slightly elevated (150–154ng/dL; No.<134). Since all other supplemental tests did not suggest tumor recurrence, such increased levels were attributed to a drug interaction. Omeprazole treatment was therefore discontinued three weeks before control laboratory tests, and chromogranin A levels normalized (63.3 and 37ng/mL; No.: 19.4–98.1). Three years after surgery, patient continues to be symptom-free, and results of supplemental tests have been normal to date.
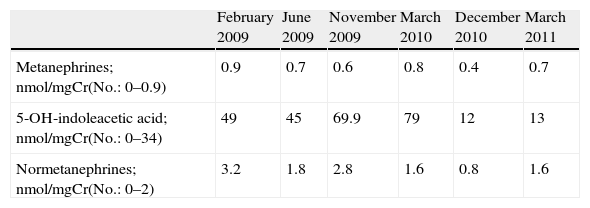
Metanephrine, normetanephrine, and 5-hydroxyindoleacetic acid levels in urine.
| February 2009 | June 2009 | November 2009 | March 2010 | December 2010 | March 2011 | |
| Metanephrines; nmol/mgCr(No.: 0–0.9) | 0.9 | 0.7 | 0.6 | 0.8 | 0.4 | 0.7 |
| 5-OH-indoleacetic acid; nmol/mgCr(No.: 0–34) | 49 | 45 | 69.9 | 79 | 12 | 13 |
| Normetanephrines; nmol/mgCr(No.: 0–2) | 3.2 | 1.8 | 2.8 | 1.6 | 0.8 | 1.6 |
Surgery performed on October 2010.

Carcinoid tumors are uncommon, with an annual incidence of approximately 8 cases per 100,000 population.1 Only 1–2% of these tumors originate in ovarian tissue,2 where they often seat, as in the reported case, on a cystic teratoma or dermoid tumor.3 According to some studies, this confers them a better prognosis as compared to tumors not occurring on a germ cell tumor.4
Although symptoms of carcinoid syndrome are highly characteristic, the syndrome only occurs in a small proportion of carcinoid tumors. Insular ovarian carcinoid tumor, the histological subtype of our patient, is most common and is the only one that is associated to carcinoid syndrome in one-third of cases.5,6
In the reported case, menopause had to be included in differential diagnosis of flushing because of patient age. Although hot flashes spontaneously disappear in most women a few years after the start of menopause, they may persist in up to 30% of women older than 60 years, and in 9% of those over 70 years of age.7 However, hot flashes had disappeared in our patient three years after menopause, and had never been associated to facial erythema as the one she subsequently experienced in the setting of carcinoid syndrome.
Chromogranin A is a protein found in neurosecretory vesicles of neuroendocrine tumor cells. It is currently considered to be the best biochemical marker for follow-up of these tumors because of its high sensitivity.8 It is however less specific, and there are various conditions where slight chromogranin A elevations may occur, such as kidney or liver insufficiency. Long-term use of proton pump inhibitors is considered the main cause of increased chromogranin A levels unrelated to a neuroendocrine tumor. Decreased acidity leads to increased gastrin release and enterochromaffin cell hyperplasia, with a resultant increase in chromogranin A. In the case reported, long-term omeprazole treatment hindered interpretation of chromogranin A during follow-up. As recommended by the literature, omeprazole was discontinued to obtain a reliable value of the marker.9
Please cite this article as: Tomé Fernández-Ladreda M, Martínez de Pinillos Gordillo G, Pichardo López de Haro F, Cózar León MV. Tumor carcinoide sobre teratoma ovárico quístico. Endocrinol Nutr. 2014;61:434–436.
