


Recent studies in Spain have shown an inadequate iodine intake in a significant proportion of pregnant women. Pregnancy increases thyroid hormone requirements, and adequate iodine intake is therefore needed.
Material and methodsOne hundred and forty-seven women in their third trimester (week 37) of pregnancy provided a blood sample and a 24-h urine sample to test serum and urine iodine levels and completed a food frequency questionnaire to assess iodine intake during pregnancy. Serum TSH levels were measured in the babies born to the 140 mothers in the postpartum group.
ResultsOnly 10.9% of pregnant women consumed more than 250μg iodine daily, and 24.4% of them consumed less than 100μg daily. Mean free T4 levels were 9.37pmol/L, and 74 women (54.41%) had levels below the hypothyroxinemia threshold. TSH levels were normal in 135 newborns (96.4%), while 5 (3.6%) had levels higher than 5μU/mL.
En España, estudios recientes han demostrado que existe una ingesta insuficiente de yodo en un porcentaje importante de mujeres embarazadas. El embarazo supone un aumento en los requerimientos de hormonas tiroideas, para lo que es necesaria una ingesta de yodo adecuada.
Material y métodosSe reclutó una muestra de 147 gestantes en el tercer trimestre de embarazo en las que se determinó la ingesta de yodo, la yoduria y la función tiroidea. Las concentraciones de TSH se determinaron en los 140 recién nacidos hijos de dichas mujeres.
ResultadosSolo el 10,9% de las gestantes consumen más de 250μg de yodo diarios. La media de T4 libre fue de 9,37pmol/L y 74 mujeres (54,41%) presentaban valores por debajo del umbral de hipotiroxinemia. Las concentraciones de TSH fueron normales en 135 recién nacidos (96,4%), mientras que en 5 (3,6%) se observaron concentraciones de TSH superiores a 5μU/mL.
The WHO considers inadequate iodine intake to be the main avoidable cause of mental retardation and cerebral palsy, and it is estimated that it still affects today, to a greater or lesser extent, more than 2000 million people, i.e. one-third of the world population.1–4
The Working Group on Iodine Deficiency Disorders of the Spanish Society of Endocrinology and Nutrition holds regular meetings in Spanish towns and cities where the iodine deficiency problem has not been solved in order to promote or support programs to prevent iodine deficiency. In 2009 the meeting was held in Huelva, and the group issued a statement analyzing the situation in Spain. The statement concluded by saying, among other things, that health authorities have devised and implemented very few public health programs to eradicate iodine deficiency in the population. Such programs have only been implemented in Asturias, Extremadura, Catalonia, Galicia, the Basque Region, and Andalusia, and some of these have had only a limited effect. In addition, most recent studies conducted in the pregnant population have shown that a large number of these women still have an adequate iodine intake. It should also be taken into consideration that iodinated salt consumption is voluntary. Therefore, if programs periodically promoting its use are not undertaken, there is a significant risk of non-use.5
Thyroid hormone requirements increase during pregnancy, and adequate iodine intake is therefore essential. An increased and sustained production of thyroid hormones is more difficult if Iodine deficiency exists, and increased TSH levels and permanent thyroid gland enlargement may be seen at the end of pregnancy. This may compromise the normalization of thyroid function in women after pregnancy. If dietary iodine deficiency exists, the body activates self-regulation mechanisms, in particular the synthesis of T3, requiring three iodine atoms only, instead of T4, requiring four atoms. This causes hypothyroxinemia in the mother, but not hypothyroidism, because circulating T3 levels are usually normal or increased and prevent increases in TSH levels. This maternal hypothyroxinemia during the first half of pregnancy is the main factor responsible for changes in the neurological development of the embryo and fetus.
The purpose of this study was to assess iodine intake and analyze its impact on thyroid function of the mother and newborn.
Subjects and methodsSubject selectionA total of 147 women in their third trimester of pregnancy (week 37) attending the Department of Gynecology and Obstetrics of Clínica Universidad de Navarra were enrolled in the study between January 2002 and March 2003.
Subsequently, in 2007, a sample of 77 postpartum women was enrolled in order to assess the amount of iodine they had taken during pregnancy and compare it to the 2002–2003 pregnant women.
Exclusion criteria included diagnosis of thyroid disease before pregnancy, bowel disease involving intestinal malabsorption, and treatment with drugs affecting the metabolism of thyroid hormones. The study was approved by the ethics committee of the center, and informed consent was obtained from the participants.
Iodine intake in pregnant womenTo assess iodine intake in pregnant women, a semiquantitative food frequency questionnaire (FFQ1) was prepared based on a prior food use frequency questionnaire devised in 1993 by Martín-Moreno et al. to assess intake in the Spanish population.6 For the FFQ1 to be better adapted to the study objectives, a number of changes were made: food items with less than 10μg iodine per 100g of product were removed, and food items which, although not frequently consumed, contain high amounts of iodine were added. The modified questionnaire therefore included a total of 73 foods, classified into five groups: dairy products; eggs, meat and fish; vegetables; fruit; miscellaneous. The question format was based on multiple, closed answers with a total of nine options: never or almost never; 1–3 times monthly; once weekly; 2–4 times weekly; 5–6 times weekly; once daily; 2–3 times daily; 4–6 times daily; more than 6 times daily. The questionnaire was semiquantitative in nature because it did not require the total amount taken to be detailed. A reference serving or portion and a consumption frequency acting as a guide to estimate nutrient content was used instead. The questionnaire also collected data as to whether or not iodinated salt or drugs or multivitamin preparations containing iodine had been used, and the place of residence in the past year.
The FFQ1 was completed during admission to the maternity unit, in the three days following delivery, and referred to the nine months of pregnancy. Daily iodine intake was calculated at the Department of Preventive Medicine of Navarre University based on the questionnaire. Results were as expressed as μg of iodine ingested daily.
To assess iodine intake in pregnant women, in addition to FFQ1, iodine concentration was measured in 24-h urine collected in the third trimester of pregnancy (week 37). Urinary iodine was measured by spectrophotometry using the Sandell–Kolthoff reaction.7,8
Assessment of thyroid function in pregnant womenA blood sample was taken from pregnant women in week 37 of pregnancy. Samples were processed at the chemistry laboratory of the hospital, where serum levels of TSH and free T4 were measured using a microparticle enzyme immunoassay.
The reference values of the abovementioned laboratory were used for the different hormones.
Screening for congenital hypothyroidismA blood sample was taken from the heel of babies born to the study women in their second or third day of life to assess serum TSH levels. The procedure used was a delayed immunofluorescence technique (DELFIA® kits, Wallac Perkin Elmer, Turku, Finland), which measures TSH from blood dried and deposited on filter paper.9,10
Statistical analysisStatistical analysis was performed using software SPSS® for Windows version 15.0 (SPSS Inc., Chicago, USA).
A descriptive analysis was made of both qualitative and quantitative variables using the following descriptive statistics: arithmetic mean and standard deviation for parameters which met normality criteria, and median and interquartile range for those not meeting normality criteria. To assess sample normality, kurtosis and skewness indices were analyzed, and a Kolmogorov–Smirnov test was used.
Differences were considered statistically significant if their associated probability (p) was < 0.05, and highly significant if p<0.01.
A Chi-square test was used to compare the proportion of women who took iodinated salt and iodine-rich multivitamin preparations between the sample of pregnant women recruited in 2002 and the sample of post-partum women recruited in 2007.
A Student's t test for independent samples was used to compare urinary iodine levels in both the samples recruited in 2002/2003 and in 2007 based on the use of non-use of iodinated salt and iodine-rich multivitamin preparations.
ResultsSample descriptionThe sample recruited in 2002 consisted of 147 pregnant women in week 37 of pregnancy. Seven (4.8%) of these women were excluded for undiagnosed hypothyroidism. The pregnant women were aged 22–43 years, with a mean age of 32 (SD 5), and had no relevant medical history or history of prior thyroid disease.
Assessment of iodine intake by pregnant womenSemiquantitative questionnaire on the frequency of use of iodine-rich food itemsIn 2002, 119 (85%) of the 140 study participants adequately completed the dietary habits questionnaire (FFQ1). A mean iodine intake of 151μg/day was found. The questionnaire data revealed that only 10.9% of the women took iodine amounts higher than 250μg/day, and 24.4% took less than 100μg daily.
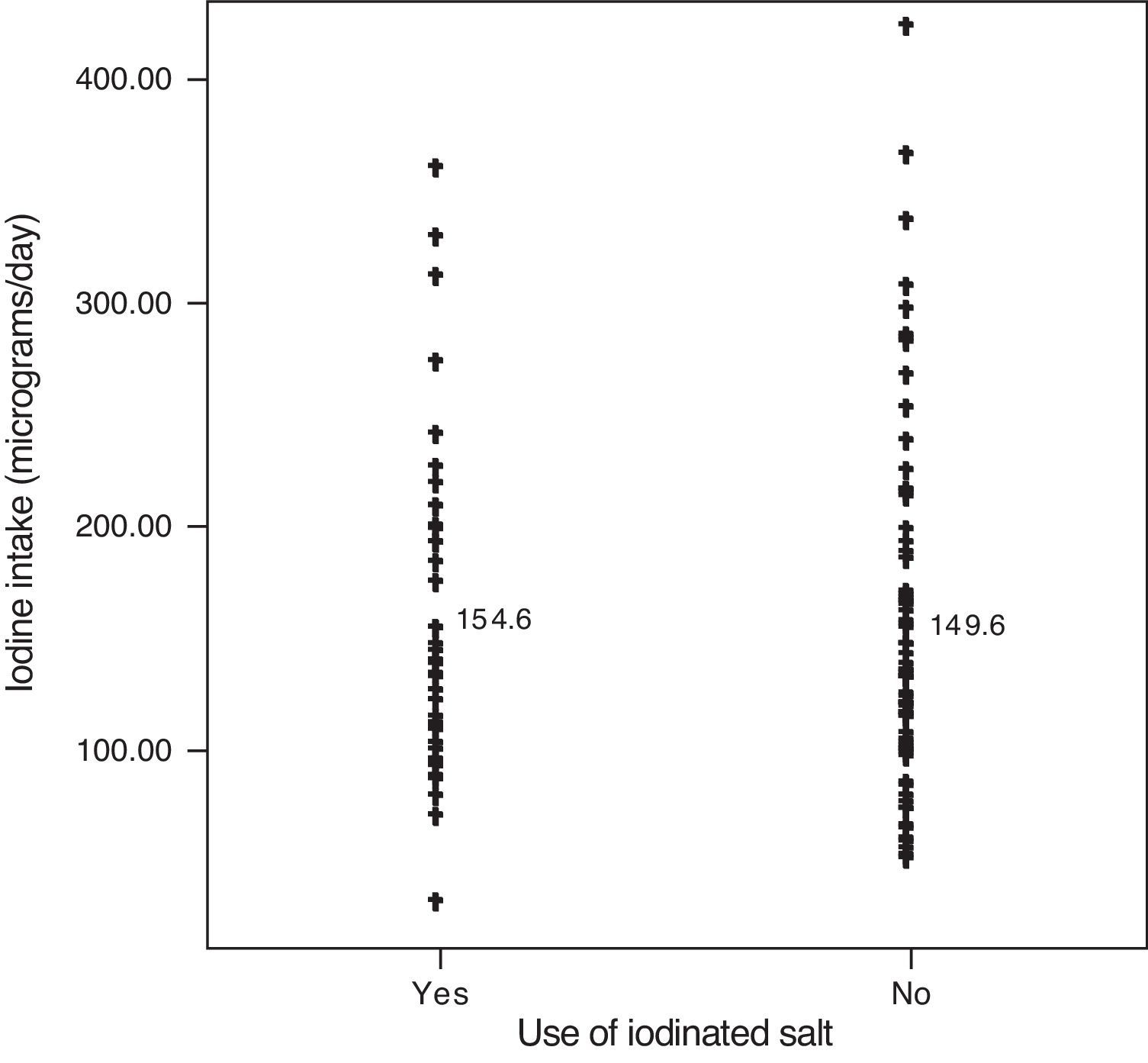
Thirty-seven percent of the women used iodinated salt to flavor meals, while 63% did not. A comparison of mean iodine intake in these two groups of pregnant women showed no statistically significant differences, with mean intake being 154.6μg/day in the first group and 149.6μg/day in the second group (Fig. 1).

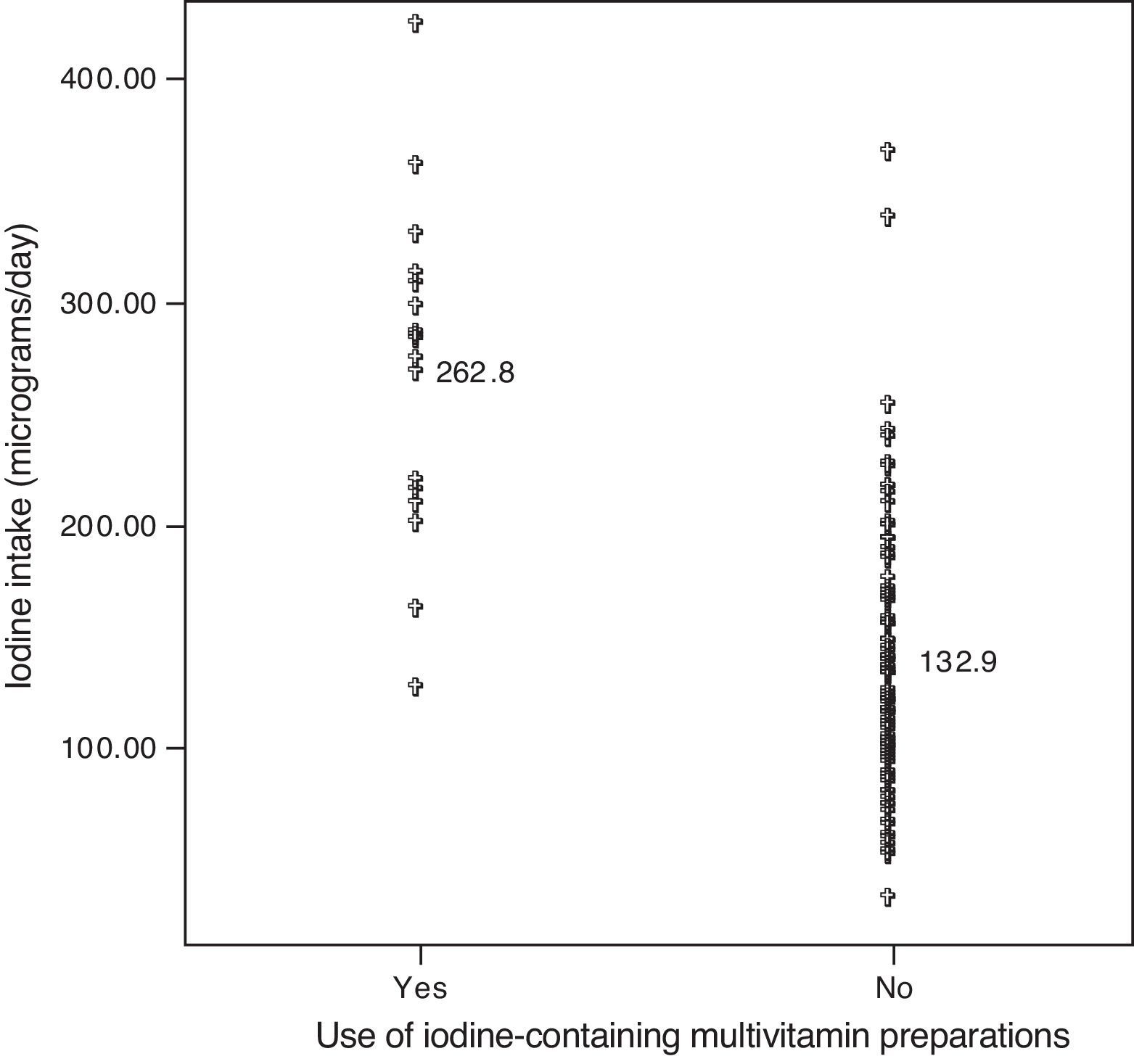
On the other hand, only 14% of the pregnant women had taken iodine-rich multivitamin preparations during pregnancy, with a mean iodine intake of 262.8μg/day. However, women who had not taken such nutritional supplements (86%) took a mean of 132.9μg iodine daily, a significantly lower intake as compared to the group of pregnant women taking the supplements (p<0.001) (Fig. 2).
Urinary iodine levels
Iodine levels were measured in 24-h urine from 121 women (86.5% of participants). The median level obtained was 87μg/L (48–142). In the remaining 19 participants, measurement was not possible due to inadequate urine sample collection.
Fifty-six percent of women in our sample had urinary iodine levels less than 100μg/L, and 24.7% had levels less than 50μg/L. Urinary iodine levels ranging from 150 to 250μg/L, as recommended in pregnancy, were found in only 19.8% of the sample. Urinary iodine levels higher than 250μg/L were measured in five pregnant women (4.1%), with the highest level being 339μg/L.
A comparison of urinary iodine levels between pregnant women using and not using iodinated salt showed no statistically significant differences, so that median levels were 90.6μg/L in the first group and 87.9μg/L in the second group (p=0.470).
As occurred with mean iodine intake, median urinary iodine level in the group of women treated with iodinated multivitamin preparations was 143.9μg/L (101–194), as compared to 84μg/L (47–124) in all other women. This difference in urinary iodine levels between the two groups was statistically significant (p<0.01).
Differences in iodine intake between the pregnant women recruited in 2002 and 2007In the sample recruited in 2007, 38% of pregnant women had an iodine intake lower than 250 μg/day during pregnancy. Of the 77 women who completed the questionnaires, 74% (57 pregnant women) took iodinated salt with meals and 62% (48 women) had received iodine-rich multivitamin preparations.
Pregnant women from the sample recruited between January 2002 and March 2003 had a mean daily iodine intake of 151μg, while the women studied in 2007 had an iodine intake of 299.87μg/day. The difference was statistically significant.
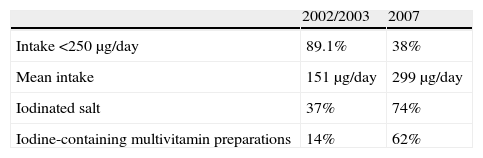
Based on the foregoing, the proportion of women using iodinated salt to flavor meals was higher in the 2007 sample than in the 2002/2003 sample, 74% versus 37%, respectively. The proportion of women taking iodine-rich multivitamin preparations was also significantly higher in the 2007 sample as compared to the 2002/2003 sample, 62% and 14% respectively (Table 1).
Differences in intake of iodine, iodinated salt, and iodine-containing multivitamin preparations between pregnant women recruited in 2002/2003 and in 2007.
| 2002/2003 | 2007 | |
| Intake <250μg/day | 89.1% | 38% |
| Mean intake | 151μg/day | 299μg/day |
| Iodinated salt | 37% | 74% |
| Iodine-containing multivitamin preparations | 14% | 62% |
As noted above, maternal thyroid function was initially assessed by measuring TSH and free T4 in the sample recruited in 2002/2003. The reference values used were those from our laboratory, which considers TSH levels ranging from 0.2 to 5μU/mL and free T4 levels ranging from 9.5 to 23.9pmol/L to be normal.
Based on these values, 7 of the 147 women who started the study in 2002/2003 (4.8%) were excluded for undiagnosed hypothyroidism before pregnancy (TSH levels higher than 5μU/mL and free T4 levels less than 9.5pmol/L). Among the remaining 140 participants, free T4 was measured in 136 (total T4 levels were tested in the other four patients due to an error in the request) and TSH in 139 (one patient was excluded due to inadequate sample drawing). Thr median free T4 level was 9.37pmol/L (8.29–10.47), and 74 of the pregnant women (54.41%) had values below the hypothyroxinemia threshold. The median TSH level was 1.43μU/mL (1.07–1.88), and all participants had values less than 5μU/mL.
Assessment of neonatal thyroid functionNeonatal TSH levels were obtained from the population screening for congenital hypothyroidism performed in the 140 newborns. Normal TSH levels were seen in 135 newborns (96.4%), but values higher than 5μU/mL were found in the remaining five babies (3.6%).
DiscussionIodine intake in pregnant womenUntil 1983, the term “endemic goiter” was used to designate iodine deficiency. In that year, Hetzel, based on studies by other authors and on his own studies in iodine deficient populations, listed the wide spectrum of diseases caused by iodine deficiency and proposed that the term “endemic goiter” should be replaced by “iodine deficiency disorders”.11 This semantic change in the name of a set of diseases broadened the significance of this healthcare problem, highlighting its nature as a multi-systemic condition caused by a deficiency of this element.12
Iodine is an essential micronutrient needed for thyroid hormone synthesis. According to the WHO, UNICEF, and ICCIDD, the recommended daily intake in healthy adults is 150μg.13,14 Thyroxine requirements and, thus, iodine needs increase as the result of changes occurring during pregnancy. It may be assumed that a 50% increase is needed, i.e. from 150 to 225μg iodine daily, which is close to the amounts recommended before 1992. However, increasing epidemiological data suggest that this increase in iodine intake may be insufficient to avoid a depletion of reserves of iodinated compounds in the thyroid gland.15 Accordingly, the currently recommended iodine intake ranges from 250 to 300μg/day in pregnant women and from 225 to 350μg/day during lactation.15,16
The data collected from our questionnaire suggest that the vast majority of pregnant women in our sample recruited between January 2002 and March 2003 took iodine amounts lower than those currently recommended.
It should be noted that iodine deficiency persists in some sectors of the population of certain countries, particularly pregnant women, despite the widespread use of iodinated salt and universal salt iodination programs, as occurs in Spain. Studies conducted in Spain show that in communities where iodine deficiency is in the process of being eradicated, a poor iodine nutritional status persists in more than half the pregnant women.17 This was also seen in our study, which concluded that iodinated salt consumption is not sufficient to meet iodine requirements in pregnancy. Diet supplementation with iodine-rich multivitamin preparations is therefore recommended, because the women who took them had higher urinary iodine levels and a total iodine intake significantly higher than those who did not receive them and because they also met the current recommendations. These data support the relevance of the decision by most Spanish autonomous communities and the American Board of Public Health, amongst others, to implement a program to supplement the diet of pregnant women with drug products, in addition to promoting the use of iodinated salt.
The data collected from the sample of women recruited in 2007 suggest that more than half of them ingested daily iodine amounts which met the current recommendations. Despite this, there were still 38% of pregnant women who could not reach these levels, with the resultant potential impact on the psychomotor development of their children. It should be noted that 73.7% of this 28% of women with deficient iodine provision did not take iodine-rich multivitamin preparations. We may therefore conclude again, in agreement with many other studies, that iodinated salt and exogenous iodine supplements are required to achieve optimum levels of daily iodine intake during pregnancy.18,19 Despite this, both our study and the one conducted by Peris Roig et al. in Valencia in 2008 show that recommendations by Spanish scientific societies are not applied, as there is no universal recommendation to supplement the diet of pregnant women with exogenous iodine.20
It should be stressed that although there has been a substantial increase in the proportions of women who use iodinated salt with meals (from 37% in 2002/2003 to 74% in 2007) and who supplement their diets with exogenous iodine (from 14% in 2002/2003 to 62% in 2007), 38% of women did not meet daily iodine requirements in 2007.
Maternal thyroid functionPeople living in iodine deficient areas do not usually experience clinical or subclinical hypothyroidism, including pregnant women. Circulating TSH levels are normal, even in people who have developed goiter.15 This is because the thyroid gland reacts to decreased circulating levels by activating thyroid self-regulation mechanisms, which act without the need for changes in TSH levels, even in hypophysectomized patients. As the result of these adaptations, the little iodine reaching the thyroid follicles is used for the preferential synthesis and secretion of T3, which only requires three iodine atoms, to the detriment of the secretion and synthesis of T4, for which four atoms are required. This results in a state of hypothyroxinemia without hypothyroidism, because circulating T3 is usually normal or increased, which prevents TSH increase above the normal limit. This hypothyroxinemia pattern was found in over half the pregnant women in our sample, and was due to their low iodine intake.
Screening for congenital hypothyroidismSerum TSH levels in newborns are a particularly sensitive marker of iodine nutritional status during pregnancy and in newborns, and are considered a very helpful tool for monitoring changes over time in countries with mild or moderate iodine deficiency. The reason for this is that the thyroid gland of newborns is highly sensitive to iodine deficiency. Since intrathyroid iodine levels are very low in newborns under normal conditions, TSH levels transiently increase in response to small reductions in iodine provision in order to maintain normal thyroid hormone secretion.4,21 In order to be able to use neonatal TSH as a marker of nutritional iodine status in a population, a neonatal screening system for congenital hypothyroidism should be implemented. Such a system must ensure that samples are taken after 48 h of life of the newborn to avoid the physiological TSH increase occurring in the first hours of life.22,23
According to WHO recommendations, if a population has no iodine deficiency, neonatal TSH levels higher than 5μU/L should appear in less than 3% of newborns. A frequency ranging from 3% to 19.9% suggests mild iodine deficiency, while rates ranging from 20% to 39.9% and those higher than 40% suggest moderate and severe deficiency respectively.21,24
In the population analyzed, TSH levels higher than 5μU/L were detected in 3.6% of newborns, and should therefore be considered to have had a mild iodine intake deficiency. In 2005, the Committee on Metabolic Errors of the Spanish Society of Clinical Chemistry and Molecular Pathology collected neonatal TSH levels from all the autonomous communities. Levels higher than 5μU/L were reported in 3.6% of newborns in Navarre,17 which agrees with our study data.
ConclusionsA high proportion of pregnant women in both the 2002/2003 and 2007 samples did not meet the current iodine intake requirements. This suggests that the Spanish pregnant population continues to be at risk of suffering iodine deficiency disorders. These result in increased comorbidity in both them and their offspring. Therefore, a universal salt iodination program should be implemented in Spain, as well as standardized protocols for the provision of supplemental exogenous iodine to all healthy pregnant women even before conception, similar to that which occurs with folic acid, so that adequate iodine intake can be ensured.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Suárez Rodríguez M, Azcona San Julián C, Alzina de Aguilar V. Ingesta de yodo durante el embarazo: efectos en la función tiroidea materna y neonatal. Endocrinol Nutr. 2013;60:352–357.
