


To provide practical recommendations for evaluation and follow-up of patients with normocalcemic primary hyperparathyroidism.
ParticipantsMembers of the Bone Metabolism Working Group of the Spanish Society of Endocrinology.
MethodsA systematic search was made in MEDLINE (PubMed), using the terms normocalcemic primary hyperparathyroidism and primary hyperparathyroidism, for articles in English published before 22 November 2012. Literature was reviewed by 2 members of the Bone Metabolism Working Group of the Spanish Society of Endocrinology, and after development of recommendations, the manuscript was reviewed by all other members of the Group, and their suggestions were incorporated.
ConclusionsThe document provides practical recommendations for evaluation and follow-up of patients with normocalcemic primary hyperparathyroidism. There is however little evidence available about different aspects of this disease, mainly progression rate and clinical impact. More data are therefore needed before definite recommendations may be made.
Proporcionar unas recomendaciones prácticas para la evaluación y seguimiento de los pacientes con hiperparatiroidismo normocalcémico.
ParticipantesMiembros del Grupo de Trabajo de Metabolismo Mineral de la Sociedad Española de Endocrinología y Nutrición.
MétodosSe realizó una búsqueda sistemática en MEDLINE de la evidencia disponible usando las siguientes palabras clave: normocalcemic primary hyperparathyroidism y primary hyperparathyroidism. Se revisaron artículos escritos en inglés con fecha de inclusión hasta el 22 de noviembre de 2012. La bibliografía fue revisada por 2 miembros del Grupo de Trabajo de Metabolismo Mineral de la Sociedad Española de Endocrinología y Nutrición, y tras la formulación de recomendaciones el manuscrito fue revisado por el resto de los integrantes del Grupo con incorporación de las sugerencias realizadas.
ConclusionesEl documento establece unas recomendaciones prácticas acerca de la evaluación y seguimiento de los pacientes con hiperparatiroidismo normocalcémico. No obstante, y dada la escasa evidencia disponible acerca de diferentes aspectos de esta situación (tasa de progresión y repercusiones clínicas, fundamentalmente), son necesarios más datos antes de poder establecer recomendaciones definitivas.
- -
Normocalcemic primary hyperparathyroidism (PHP) is considered to be a new phenotype of the disease characterized by persistently elevated parathyroid hormone (PTH) levels and normal calcium levels in the absence of identifiable causes of secondary hyperparathyroidism or PTH elevation.
- -
The underlying biological mechanism is not known exactly. It could be a first stage of the disease or a specific condition characterized by renal and bone resistance to the action of PTH.
- -
This is an increasingly diagnosed condition, detected particularly during the evaluation of perimenopausal women with decreased bone mass or in the evaluation or follow-up of patients with osteoporosis.
- -
Normocalcemic PHP has a heterogeneous and variable phenotype which varies from the absence of typical PHP features to symptomatic cases with specific complications.
- -
The diagnostic approach should focus on the exclusion of all causes of secondary hyperparathyroidism, particularly vitamin D deficiency (25-OH vitamin D levels less than 30ng/mL) and kidney function impairment (glomerular filtration rate less than 60mL/min as estimated by CKD-EPI). The role of potent anti-catabolic drugs should also be taken into consideration.
- -
Treatable causes of secondary hyperparathyroidism should be corrected: vitamin D supplements should be administered to maintain levels higher than 30mg/dL of 25-OH vitamin D (monitoring calcium levels for the potential development of mild hypercalcemia if it is PHP); treatment with low hydrochlorothiazide doses (12.5–25mg/d) if hypercalciuria exists, especially in the presence of nephrolithiasis; treatment with calcium citrate (after meals) in the event of low calcium intake or malabsorption. In patients with renal failure, the effect of low doses of 1.25-dihydroxyvitamin D (0.125–0.25mcg/48h) may be tested, while in those treated with potent anti-catabolic drugs, these may be discontinued for 12–24 weeks before repeat testing (for denosumab, repeat 7–9 months after the last drug administration).
- -
Its natural history is not well known. Some patients evolve to hypercalcemia, but most of them (more than 75%) do not. No predictors of the development of hypercalcemia appear to exist, and annual monitoring with measurement of total and corrected calcium levels is therefore recommended. Although ionic calcium measurement is part of the definition of normocalcemic PHP, and according to some authors is indicated during follow-up, it has a number of practical limitations that should be borne in mind.
- -
As regards bone mass measurement by DXA, there is no clear evidence for recommending it to all patients. However, it appears reasonable to perform DXA at least in patients with an age close to that recommended in the general population (65 years in women and 70 years in men), or from 50 years in patients with other risk factors for low bone mass and/or fractures.
PHP is a common endocrinological disorder characterized by excess and incompletely regulated PTH secretion by one or more parathyroid glands. Asymptomatic PHP with mild or intermittent hypercalcemia and an absence of classical symptoms such as lithiasis, cystic fibrous osteitis, or symptoms of marked hypercalcemia, is currently the most common presentation (80%). When patients with osteoporosis and other mineral metabolism changes are studied, cases with elevated PTH levels in the presence of normal total and ionic calcium levels are increasingly common. This condition is called normocalcemic PHP, and in these cases it is essential to distinguish whether it is a secondary hyperparathyroidism or an early form of PHP, because the biochemical findings may be similar in both cases. The wide availability of automated PTH tests has caused this condition to emerge as one of the most common reasons for consultation in our specialty, and warrants preparation by the Working Group on Mineral Metabolism of the SEEN of a consensus document to provide a consistent approach to its diagnosis and management.
MethodsIn order to formulate these recommendations, a systematic search of the evidence available was made in MEDLINE using the terms normocalcemic primary hyperparathyroidism and primary hyperparathyroidism. Articles written in English included up to 22 November 2012 were reviewed. The literature was reviewed by two members of the Working Group on Mineral Metabolism of the SEEN and, once their recommendations were formulated, the manuscript was reviewed by all the other members of the group and their further recommendations were included.
Definition of normocalcemic primary hyperparathyroidismThe third international workshop on the management of asymptomatic PHP officially recognized for the first time normocalcemic PHP, defined as documented elevated serum PTH levels in the presence of normal serum calcium levels after the strict ruling out of all potential causes of secondary hyperparathyroidism.1 It should be noted that serum (and ionic) calcium levels should be normal at all times because in PHP, especially when asymptomatic, hypercalcemia may be intermittent.
DiagnosisDiagnosis is based on elevated PTH levels, confirmed at least two times, in the absence of hypercalcemia (normal total and ionic serum calcium levels). However, the measurement of ionic calcium poses a number of practical difficulties to be considered (precision problems, lack of standardization, the need for special sample management, and its high cost).2
Another significant aspect is the cut-off point for considering that PTH elevation exists, because this varies depending on the measurement method used. The most widely used procedure is second-generation immunoradiometric assay and its variants, introduced by Nichols in 1987. This is a dual antibody assay directed against both the regions PTH 1–34 and PTH 39–84. It has the disadvantage that it detects long C-terminal PTH fragments accounting for 20–44.8% of PTH immunoreactivity in normal subjects. The most recent third-generation methods, which detect “complete” PTH, use an antibody directed against epitope PTH 1–4 and another antibody against PTH 39–84 and provides values 20% lower than the second-generation procedures. Its sensitivity in detecting PTH increases is similar to that of second-generation assays, but it is technically more cumbersome.3 It should be noted that PTH levels do not allow for differential diagnosis between normocalcemic and hypercalcemia PHP because individual PTH levels greatly overlap.4
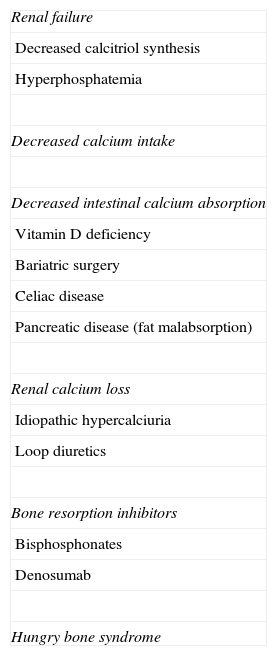
For the diagnosis of normocalcemic PHP, it is essential to rule out the causes of secondary hyperparathyroidism (Table 1). Among these, vitamin D deficiency is the most common cause of elevated PTH and normal serum calcium. Concentrations of 25-OH vitamin D defining this state of insufficiency are not universally established. Deficiency has recently been defined as a value less than 20ng/mL (50mmol/L); insufficiency is defined as 25-OH vitamin D levels ranging from 21 to 29ng/mL (52.5–72.5mmol/L), while vitamin D values above 30ng/mL are considered sufficient.5 In the range of 30–40ng/mL, the exponential relation between 25-OH vitamin D and PTH levels starts to flatten.6 The potential impact of 25-OH vitamin D levels in the general population when establishing PTH reference limits is controversial.7,8
Causes of secondary hyperparathyroidism.
| Renal failure |
| Decreased calcitriol synthesis |
| Hyperphosphatemia |
| Decreased calcium intake |
| Decreased intestinal calcium absorption |
| Vitamin D deficiency |
| Bariatric surgery |
| Celiac disease |
| Pancreatic disease (fat malabsorption) |
| Renal calcium loss |
| Idiopathic hypercalciuria |
| Loop diuretics |
| Bone resorption inhibitors |
| Bisphosphonates |
| Denosumab |
| Hungry bone syndrome |
Based on the mentioned criteria for the diagnosis of normocalcemic PHP, 25-OH vitamin D levels should be higher than 30ng/mL.5 There are also data showing that these are the values of 25-OH vitamin D allowing for adequate osteoid mineralization.9 For this, vitamin D may have to be administered for a short time period (two or three months) until vitamin D sufficiency is achieved. If PTH continues to be elevated and calcium is still normal, a diagnosis of normocalcemic PHP may be made after all potential causes of secondary hyperparathyroidism have been ruled out. When vitamin D is administered, laboratory monitoring should be performed because of the possibility that vitamin D is masking hypercalcemia.
As regards the dosage scheme required for correcting vitamin D deficiency, there is no specific recommendation in PHP patients. It seems therefore reasonable to use a scheme similar to that recommended for patients with vitamin D deficiency: 16,000IU of calcifediol (Hidroferol® 0.266mg, one vial) weekly for 8 weeks, followed by maintenance treatment with 1000–1500IU/day (Hidroferol® 0.266mg, one vial every 10 or 15 days).
In addition to vitamin D deficiency, the most common causes of PTH increase include idiopathic hypercalciuria and a decreased glomerular filtration rate (less than 60mL/min as estimated by CKD-EPI), although PTH elevation has been reported with glomerular filtration rates of 75–80mL/min.9 Anti-catabolic drugs (bisphosphonates and denosumab) widely used for the treatment of osteoporosis are a common cause of a moderate increase in PTH levels without hypercalcemia.10 The presence of treatment with these drugs should be assessed, because they have a very long inhibitory effect on bone resorption, especially the most potent aminobisphosphonates.11 Denosumab is an anti-RANKL monoclonal antibody with a potent anti-catabolic effect, and it also causes marked, although transient, PTH increases detectable in the first month of treatment.12
Other causes of secondary hyperparathyroidism include malabsorption, treatment with lithium, thiazide diuretics, or phosphates and hypomagnesemia. A less common cause is pseudohypoparathyroidism type Ib, which associates secondary hypocalcemia with PTH resistance in peripheral tissues. Therefore, PTH levels are usually very high. In some cases, normocalcemia may exist in the presence of moderately elevated PTH levels.
Some authors have proposed that stimulus and suppression tests should be performed in order to make a differential diagnosis between normocalcemic PHP and secondary hyperparathyroidism.13,14 Such tests are not however easy to perform in clinical practice, and are therefore usually done in the clinical research setting only.
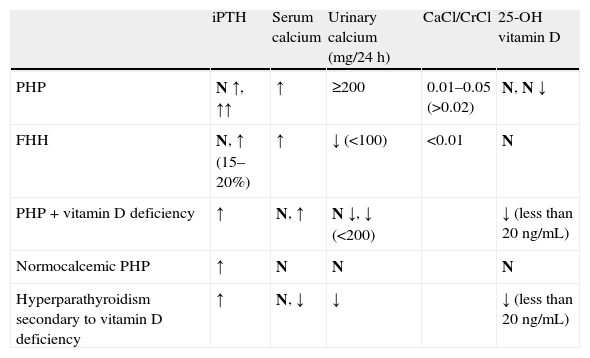
Table 2 shows the typical laboratory data for differential diagnosis of the different forms of PHP (hypercalcemic, normocalcemic, with associated vitamin D deficiency) and secondary hyperparathyroidism.
Differential diagnosis of primary hyperparathyroidism: characteristic laboratory data.
| iPTH | Serum calcium | Urinary calcium (mg/24h) | CaCl/CrCl | 25-OH vitamin D | |
| PHP | N ↑, ↑↑ | ↑ | ≥200 | 0.01–0.05 (>0.02) | N, N ↓ |
| FHH | N, ↑ (15–20%) | ↑ | ↓ (<100) | <0.01 | N |
| PHP+vitamin D deficiency | ↑ | N, ↑ | N ↓, ↓ (<200) | ↓ (less than 20ng/mL) | |
| Normocalcemic PHP | ↑ | N | N | N | |
| Hyperparathyroidism secondary to vitamin D deficiency | ↑ | N, ↓ | ↓ | ↓ (less than 20ng/mL) |
CaCl/CrCl: calcium clearance/creatinine clearance; FHH: familial hypocalciuric hypercalcemia; PHP: primary hyperparathyroidism; N: normal; iPTH: intact parathyroid hormone; 25-OH vitamin D: 25-hydroxyvitamin D.
If only studies where the causes of secondary hyperparathyroidism have been ruled out adequately are considered, normocalcemic PHP has been reported in 0.7% of a cohort of 1504 men over 65 years of age,15 in 16.7% (17.4% in women and 15% in men) of a cohort of 1305 women and 566 men (aged 31–97 years) from a population-based study, the Canadian Multicentre Osteoporosis Study,16 and in 6% of a group of healthy postmenopausal women.17
PathophysiologySome data suggest that normocalcemic PHP is a mild form of hypercalcemic PHP, characterized by somewhat lower PTH secretion, but with a similar pathological substrate (adenoma) in a majority of cases. In this regard, subjects with normocalcemic PHP had lower PTH levels and smaller adenoma sizes as compared to patients with PHP with hypercalcemia, although adenoma rates in patients undergoing surgery were similar (100% in PHP with hypercalcemia and 92% in normocalcemic PHP).4 Other authors have also shown the presence of adenoma in 100% of patients with normocalcemic PHP undergoing surgery, although the subject sample was small (n=30).18
By contrast, resistance to the effect of PTH on calcium tubular resorption specific to normocalcemic PHP has been postulated.4,19 A lower effect of PTH on bone, reflected by lower levels of bone remodeling markers and lower urinary calcium has also been reported.4 Although the cause of the decreased sensitivity of renal tubule to PTH has not been identified, the potential contribution of high sodium intake, low phosphate levels, or high estrogen levels has been reported. Finally, no CaSR expression changes have been found in parathyroid tissue from patients with normocalcemia PHP.20
Clinical pictureThe absence of hypercalcemia does not imply that patients are asymptomatic. In fact, a significant proportion may have similar signs and symptoms to those found in the hypercalcemic form of the disease, representing a variant of symptomatic PHP, in which case the consideration of surgery could be indicated. Thus, it has been proposed that the incidence of lithiasis may be similar to that seen in hypercalcemic PHP (20%). In a series of 34 patients with normocalcemic PHP, the most common clinical sign was nephrolithiasis (35% of patients). Eighteen percent of patients had hypercalciuria, 18% osteoporosis, and 6% chondrocalcinosis.4 In another group with normocalcemic PHP (59 years of mean age, 95% women, 16% postmenopausal), osteoporosis was the most common symptom (59%), 11% had fragility fractures, and 14% kidney stones. However, unlike hypercalcemic PHP, where the radius was the predominantly affected bone, lumbar (38%) and femoral (41%) osteoporosis were more common than that of the distal third of the radius (22%).21
Similarly to hypercalcemic PHP, common metabolic changes have been found in normocalcemic PHP. As compared to controls, these patients had greater body mass, as well as higher glucose, VLDL cholesterol, LDL/HDL cholesterol, triglyceride and uric acid levels, and lower HDL cholesterol levels.18 In these patients, parathyroidectomy improved total cholesterol and LDL cholesterol levels, and the LDL/HDL ratio. The prevalence of cardiovascular risk factors (high blood pressure, hyperlipidemia, glucose metabolism changes) was similar to that in hypercalcemic PHP, but the prevalence of cardiovascular disease appeared to be lower.22 Finally, another form of normocalcemic PHP where the patients are fully asymptomatic may very possibly exist. Such a form could be the initial stage of the asymptomatic hypercalcemic form of PHP, which is the most common form. To detect these patients and ascertain the actual prevalence, serum calcium and PTH would have to be measured in a cohort of subjects not referred for the assessment of osteoporosis or decreased bone mass.
To sum up, the diagnosis of normocalcemic PHP encompasses a significant clinical heterogeneity, and better clinical characterization of this disorder is therefore needed.
CourseFew data are available about the course of normocalcemic PHP, although the logical evolution to hypercalcemia does not appear to always occur. Thus, Tordjman et al. followed up 20 patients with normocalcemic PHP not undergoing surgery for a period of 4.1±3.2 years (range 1–13), none of whom experienced hypercalcemia during the follow-up time.22 Similarly, PTH and urinary calcium levels also remained stable throughout the period. In the Columbia University series of 37 patients, follow-up time was 4±0.3 years (range, 1–9), during which 22% (8 patients) experienced hypercalcemia.21 Those patients who experienced hypercalcemia during follow-up had significantly higher baseline serum and urinary levels (although within the normal range) than the group who remained normocalcemic. They also had lower baseline levels of 25-OH vitamin D, but were within the normal limits. Forty percent of patients had evidence of disease progression, thus meeting some of the requirements for parathyroidectomy included in the current clinical guidelines. Finally, in a recent study in a group of postmenopausal women with normocalcemic PHP, no progression of hypercalcemia was seen at one year of follow-up.17
This demonstrates that these patients should be regularly monitored, because the progression to hypercalcemia cannot be reliably predicted.
Risk of fractureLittle information is available about the risk of fracture in normocalcemic PHP. In a cohort of 1097 perimenopausal women from the Danish Osteoporosis Prevention Study followed up for 16 years, those with baseline PTH in the highest tertile had an increased risk of some kind of fracture (hazard ratio 1.41, 95% CI 1.11–1.79) and osteoporotic fracture (hazard ratio 1.59, 95% CI 1.2–2.1) as compared to those with lower baseline PTH. 25-OH vitamin D levels per se did not affect the risk of fracture, but elevated PTH levels were only associated with an increased risk of fracture in women with 25-OH vitamin D levels less than 50nmol/L (20ng/mL) and with those ranging from 50 to 80nmol/L (20–32ng/mL), while PTH elevation in the presence of 25-OH vitamin D values higher than 80nmol/L was not associated with an increased risk of fracture or lower bone mass in these women.23 However, the lack of consideration of low vitamin D levels as a cause of secondary hyperparathyroidism prevents these results from being generalizable to all patients with normocalcemic PHP.
To sum up, normocalcemic PHP is an increasingly diagnosed condition as the result of routine PTH measurement for the evaluation of different situations, particularly in patients assessed for osteoporosis and other mineral metabolism diseases. The scarce evidence available regarding its clinical course and impact warrants biochemical monitoring of these patients.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Martínez Díaz-Guerra G, Jódar Gimeno E, Reyes García R, Gómez Sáez JM, Muñoz-Torres M, en representación de Grupo de Trabajo de Metabolismo Mineral y Óseo de la Sociedad Española de Endocrinología y Nutrición. Hiperparatiroidismo primario normocalcémico: recomendaciones acerca del manejo y seguimiento. Endocrinol Nutr. 2013;60:456.
