


The American Diabetes Association issues annually its recommendations for diabetes mellitus screening. Although there is a high proportion of people with undiagnosed diabetes in the general population, it is suspected that many of these screening tests could be needless.
An analysis was made of the number of venous blood glucose measurements that did not meet the American Diabetes Association requirements performed in 150 people seen in primary care.
On average, an unnecessary venous blood glucose measurement is performed every 15 months. The number is significantly higher in people over 45 years of age, and also in women as compared to men (although with a p value slightly higher than 0.05).
La Asociación Americana de Diabetes publica anualmente sus recomendaciones para el cribado de diabetes mellitus. Aunque en la población general hay un porcentaje notable de diabéticos no diagnosticados, en nuestro medio la realización de análisis de cribado de diabetes es frecuente, y sospechamos que muchos de esos análisis podrían ser prescindibles.
En una muestra de 105 personas atendidas en atención primaria hemos analizado el número de glucemias venosas realizadas sin ninguna de las indicaciones establecidas por la Asociación Americana de Diabetes.
Por término medio se pide una glucemia venosa que se puede calificar como prescindible cada 15 meses. Su número es significativamente superior en personas mayores de 45 años y también superior (aunque con una probabilidad de error ligeramente mayor de 0,05) en las mujeres que en los varones.
The American Diabetes Association (ADA) publishes annually its Standards of Care and Recommendations regarding the diagnosis and treatment of this significant worldwide disease.1 One of its topics concerns the screening of diabetes in asymptomatic patients, and recommends the following:
- •
In adults without any risk factors for diabetes, testing should begin at the age of 45 years.
- •
In adults who are overweight or obese (BMI>25kg/m2) and who have one or more additional risk factors for diabetes (see Table 1) testing should be performed at the time in which both circumstances coexist.
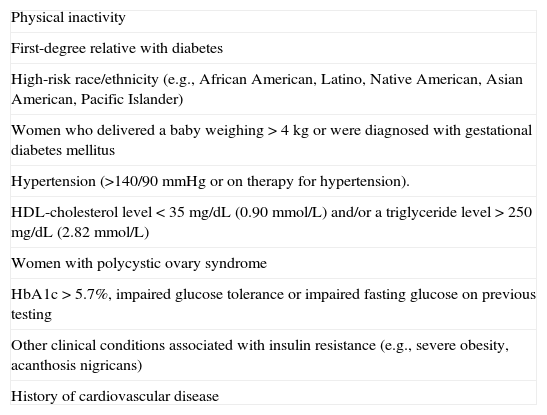
Table 1.Risk factors for development of diabetes.
Physical inactivity First-degree relative with diabetes High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander) Women who delivered a baby weighing>4kg or were diagnosed with gestational diabetes mellitus Hypertension (>140/90mmHg or on therapy for hypertension). HDL-cholesterol level<35mg/dL (0.90mmol/L) and/or a triglyceride level > 250mg/dL (2.82mmol/L) Women with polycystic ovary syndrome HbA1c>5.7%, impaired glucose tolerance or impaired fasting glucose on previous testing Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans) History of cardiovascular disease - •
If tests are normal, screening for carbohydrate metabolism alterations should be repeated every 3 years.
Consequently, the ADA suggests that screening for diabetes in asymptomatic patients below 45 years who have no associated risk factors is not necessary. And above this age, or in patients with associated risk factors, screening should be repeated every 3 years.
It is frequently acknowledged that a considerable number of patients with diabetes are not diagnosed,2,3 and the ADA itself addresses this issue. In fact, two recent studies in Spain and Portugal report that up to 50% of patients with diabetes are not correctly identified4,5 even when the ADA's screening recommendations are strictly followed. However, we believe that screening for diabetes is quite frequent, and that many of the analyses performed are, according to ADA criteria, in fact unnecessary.
There are three ways in which screening for diabetes can be accomplished: glycosylated hemoglobin, a 75g oral glucose tolerance test, and fasting glucose level. The latter is the one most generally used in our clinical practice, and will be the one that we will consider in this study.
Patients and methodsWe performed a systematic sampling of patients with no glycemic alterations or classic symptoms of hyperglycemia (polyuria, polydipsia, weight loss), who attended 2 Primary Care Centers in Vigo during the months of May–June 2011. We used the following exclusion criteria:
- •
Glucose metabolism alterations (impaired fasting glucose or diabetes in a previous analysis).
- •
People under 14 years of age.
- •
Treatment with any drug with known hyperglycemic effects: glucocorticoids, sexual steroids, growth hormone, GnRH analogs, tacrolimus, cyclosporine, alpha-interferon, protease inhibitors, thiazides, beta-blockers and calcium-channel antagonists.
- •
Treatment with a demonstrated hypoglycemic effect: acetylsalicylic acid, cotrimoxazole, pentamidine, quinine, quinidine, disopyramide.
- •
Oncologic patients.
- •
Patients with chronic hepatopathy, nephropathy or cardiopathy.
Each patient was assigned to one of two groups:
- •
Group 1: patients under the age of 45 years, with no associated diabetes risk factors. According to ADA recommendations, screening for diabetes is not necessary in these patients.
- •
Group 2: patients over 45 years of age with no associated risk factors, or adults of any age who were overweight or obese and had at least one additional risk factor. In this case, screening for diabetes with evaluation of a fasting serum glucose level was indicated every 3 years.
We reviewed all fasting serum glucose levels measured during the previous 3 years for each of the patients included in our study. We excluded analytical data obtained from the emergency room or during hospitalizations. We considered as probably unnecessary all fasting glucose levels measured over this period of time in the patients included in Group 1, and all such measurements, from the second one onwards, obtained from the patients in Group 2.
Quantitative variables are expressed as mean±standard deviation. Comparisons were performed using two-tailed Student t-test. Significant differences were considered if p<0.05.
ResultsWe obtained data from 105 patients (mean age 49±18 years old; body mass index [BMI] 26.35±5.44kg/m2). 58% were women. A total of 44 individuals were under the age of 45 years; their mean age was 31.38±6.72 years, 47.72% were male, their mean BMI was 25.23±6.06kg/m2, and the number of fasting glucose levels measurements performed was 1.79±1.30. Of the 61 patients who were aged 45 years or older, their mean age was 62.61±12.47 years, their BMI was 27.21±4.81kg/m2, and the number of fasting glucose levels obtained was 4.13±3.80.
The overall mean number of unnecessary fasting glucose levels performed during the previous 3 years was 2.3±2.4.
In the group of people under the age of 45 years, the number of probably unnecessary fasting glucose levels measured during the study period was 1.5±1.5; and in the group of patients aged 45 years or more, the result was 2.9±2.9. These differences were statistically significant (p<0.01).
Regarding the male patients, the number of probably unnecessary fasting glucose levels performed over the 3-year period was 1.7±1.8, in comparison to 2.7±2.8 in women (p=0.054).
DiscussionOn average, in our study population, more than 2 probably unnecessary fasting glucose levels are measured every 3 years, which means one avoidable fasting glucose level every 15 months.
This indicates a relatively high number of unnecessary serum glucose determinations, which probably arises as a consequence of pre-formatted analytical packages, such as the so-called “general profile” used in our center, which includes the evaluation of fasting venous glycemia.
- •
As we have previously mentioned, several publications acknowledge that a significant number of individuals with diabetes remain underdiagnosed. However, this does not seem to be the case in asymptomatic patients without associated risk factors who consult their general practitioner, at least in our area. Our data suggest that it is likely that at least one fasting serum glucose level is evaluated in these patients.
- •
The cost of performing an isolated fasting glycemia in our area, without considering the additional infrastructure and laboratory costs, is 0.06€. In other words, it is not free. Other reports have evaluated the overall analytical costs involved in screening for diabetes.6
- •
The predictive value of a positive result depends on the a priori probability of obtaining such a result; in other words, it depends on the prevalence of diabetes in this particular case. Therefore, if a test is not correctly indicated, the likelihood of a positive result turning out to be a false positive increases.7
- •
We consider that in pre-formatted analytical packages, there are probably many other determinations which are actually unnecessary and that they generally imply an even greater cost than fasting serum glucose itself. We suggest that this issue be addressed in future studies.
- •
We decided to evaluate patients under 45 years of age separately, following the ADA's recommendations for considering this age as a threshold for screening. It was not surprising that the number of probably unnecessary fasting serum glucose levels measured in the older group was significantly higher than in the younger one, since the former were more likely to be followed-up for other medical reasons which required compound pre-formatted analytical profiles in which glycemia was included.
However, what we did find surprising was that the number of probably unnecessary glycemic levels obtained in women was higher than in men, and that it almost reached statistical significance (p=0.054). We have not been able to find an explanation for this outcome, so we suggest future studies in order to clarify this issue, confirming or ruling out our results.
We excluded from our study all of those individuals who were receiving treatment with drugs which are known to have either hyper- or hypoglycemic effects,3,8 since we considered that it was reasonable for these patients to have their glycemic levels monitored. Patients with chronic liver, renal or cardiac failure, where the risk of hypoglycemia is increased, were also excluded.3,9 Finally, as we recognized that emergency care could require that patients’ glucose levels be known, these measurements were also excluded from the overall count. In general, our exclusion criteria allowed us to achieve a homogeneous sampling of patients, whose main indication for having their serum fasting glucose levels evaluated was, in fact, screening for alterations in glucose homeostasis.
In our study, there were more women than men, with an approximate ratio of 6:4. We do not consider this difference to be relevant for the overall purpose of our study.
We carried out this study under the prior impression that fasting serum glucose levels were measured more often than was really necessary, and our results have justified our suspicions. Therefore, it seems that, at least in our area, patients with diabetes are by no means underdiagnosed.2–5
Given these results, we recommend evaluating why serum fasting glucose levels are requested so frequently, especially for women of all ages and for men over 45 years of age, and we also encourage further investigation into whether these indications are correctly warranted.
Conflict of interestAll authors declare that there are no conflicts of interest.
Please cite this article as: Díez Pérez C, Rodríguez Ferro R, Penín Álvarez M. Prevalencia y coste de glucemias venosas posiblemente innecesarias en atención primaria. Endocrinol Nutr. 2013;60:513–516.
