




Acute respiratory infections (ARI) are a common cause of inappropriate antibiotic prescription (ATB) in pediatrics. FebriDx® is a rapid diagnostic test that differentiates between viral and bacterial infections. The objective is to analyse the impact of FebriDx® on ATB prescription when managing febrile ARI.
MethodsProspective study carried out in patients aged 1–<18 years with febrile ARI in the emergency department. FebriDx® was performed and the impact on management was evaluated at follow-up.
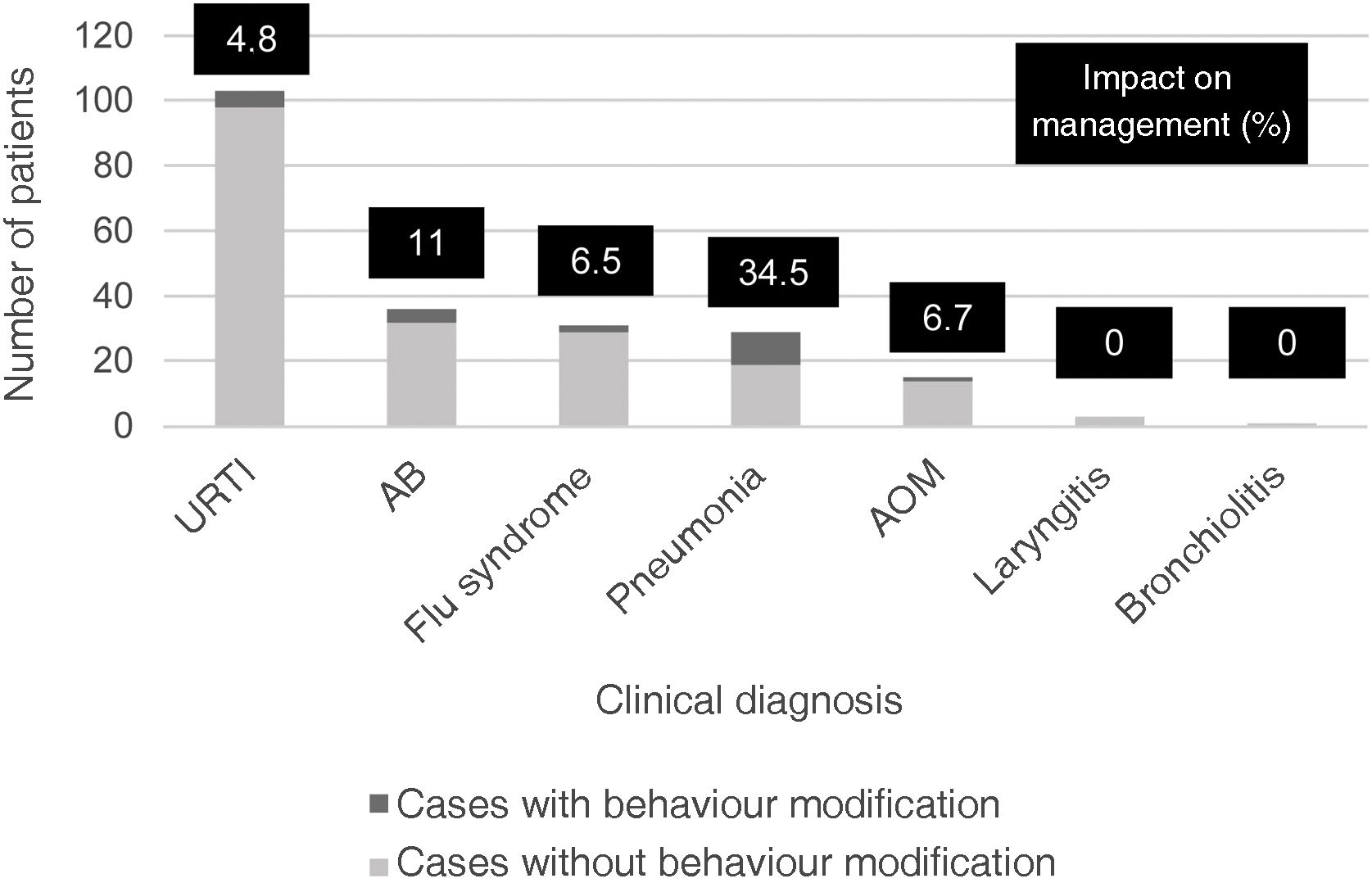
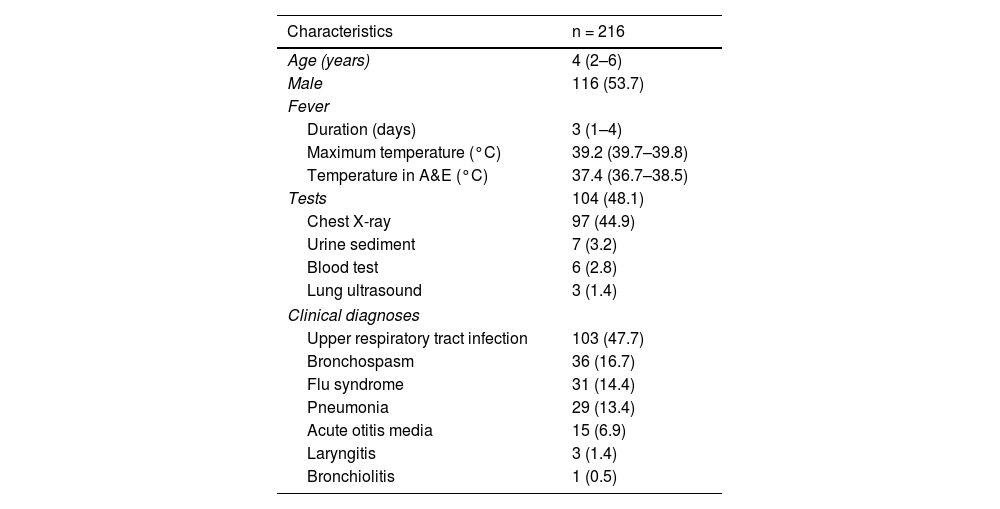
ResultsA total of 216 patients were included. Clinical assessment and FebriDx® result coincided coincided in 174 (80.5%) cases. A modification of the initial therapeutic plan was made in 22 (52.4%) of the 42 discordant ones (10.2% of the overall patients). In pneumonia the impact was 34.5%; in all cases it involved not prescribing ATB.
ConclusionsFebriDx® could be a useful tool in the management of pediatric patients with febrile ARI to optimize ATB prescription.
Las infecciones respiratorias agudas (IRA) son una causa común de prescripción inadecuada de antibióticos (ATB) en pediatría. FebriDx® es una prueba de diagnóstico rápido que diferencia infecciones virales y bacterianas. El objetivo es analizar su impacto en el manejo de niños con IRA febril.
MétodosEstudio prospectivo realizado en pacientes de 1-<18 años con IRA febril en Urgencias. Se realizó FebriDx® y se evaluó su impacto en el manejo en relación con la prescripción ATB.
ResultadosSe incluyeron 216 pacientes. La orientación médica y el resultado de FebriDx® coincidieron en 174 (80,5%) casos. Se realizó modificación del plan terapéutico inicial en 22(52,4%) de los 42 discordantes (10,2% del global de los pacientes). En neumonías el impacto fue del 34,5%; en todos los casos implicó el no prescribir ATB.
ConclusiónFebriDx® podría ser una herramienta útil en el manejo de pacientes pediátricos con IRA febril para optimizar la prescripción ATB.
Artículo
Socio de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
![]()
Para acceder a la revista
Es necesario que lo haga desde la zona privada de la web de la SEIMC, clique aquí
Para realizar los cursos formativos
La actividad estará abierta para socios de la SEIMC. IMPORTANTE, recuerde que requiere registro previo gratuito. Empezar aquí

Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
