





Bariatric surgery is one of the treatments that provides a significant, sustained weight loss,1 but several complications may arise.2
Lactobacillus species are Gram-positive rods, catalase-negative, facultative anaerobic, non-motile and non-spore-forming bacteria, which produce lactic acid as the main metabolic end product from glucose fermentation.3 These bacteria are part of the human microbiota and can be found in the gastrointestinal tract, oral cavity and female genital tract. They are usually isolated as contaminating microbiota in clinical samples. The clinical significance of these organisms isolated from normally sterile sites is subject to controversy.4
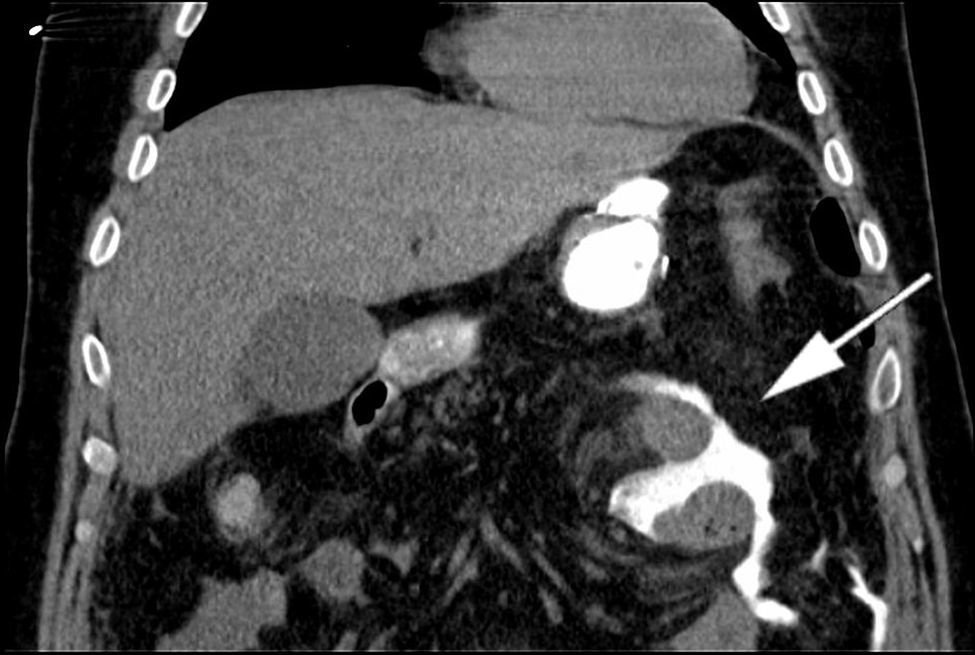
Case presentationA 41-year-old man was admitted to our hospital to undergo a laparoscopic Roux-en-Y gastric bypass as treatment for morbid obesity. During the immediate perioperative period, the patient presented with fever, hypovolemic shock and anemia due to an intraluminal gastrointestinal bleeding from the staple lines at the gastrojejunostomy. The abdominal and pelvic CT scan showed an intra-abdominal abscess and pneumoperitoneum, which required an open surgical procedure (Fig. 1). Some CT slides allowed us to confirm the anastomotic leak of oral contrast into the peritoneal cavity (Fig. 2). Surgical intervention was promptly performed.
, which turned out to be an infected hematoma, and the drainage catheter (arrow B), not actually draining the hematoma.")
 into the abdominal cavity.")
The surgeons reported a gastric perforation due to a new anastomotic leak and a right subhepatic hematoma that was drained. Blood cultures samples, as well as samples of the hematoma, intra-abdominal and pelvic fluid were sent to the microbiology laboratory.
Blood cultures were negative. Samples taken during surgery were cultured on blood agar, chocolate agar, MacConkey agar and thioglycolate broth, and incubated at 37°C in a CO2-enriched atmosphere. They were also cultured on Schaedler agar that was incubated at 37°C in anaerobic atmosphere. After 48h of incubation, a Gram-positive rod appeared in the anaerobic culture. It was identified by mass spectrometry (MALDI-TOF MS) as Lactobacillus salivarius.
Antimicrobial susceptibility testing was performed using the gradient diffusion method (E-Test) on blood agar and incubated at 37°C in a CO2-enriched atmosphere for 24h. According to the EUCAST (European Committee on Antimicrobial Susceptibility Testing) cut-off points, the strain was resistant to vancomycin and susceptible to ampicillin and clindamycin. The EUCAST does not provide cut-off points for levofloxacin and linezolid, but since MICs were 0.5mg/L for both antimicrobials, we considered that our isolate was susceptible.
The isolation of Lactobacillus spp. in pure culture from the hematoma was the only isolate grown. Cultures from intra-abdominal samples and pelvic fluid were negative.
Empirical treatment with piperacillin/tazobactam 4/0.5g every 6h was initiated. When the microbiological results were obtained, the treatment was not modified, as it should cover the intra-abdominal infection, as well as any non-identified bacteria. Antibiotic therapy was ceased after 24 days, when the intra-abdominal hematoma resolved. The patient was then successfully discharged.
DiscussionThe laparoscopic Roux-en-Y gastric bypass is one of the most common bariatric procedures worldwide,2 but life-threatening complications such as anastomotic leak and gastrointestinal hemorrhage may arise.2,5
When intra-abdominal abscesses occur, drainage and antibiotic therapy are usually required.5 Foreign matter such as gastrointestinal content or blood may facilitate the development of the infection, which is usually polymicrobial from the gastrointestinal tract, including both aerobic and anaerobic Gram-negative bacilli, as well as anaerobic Gram-positive microorganisms. However, Lactobacillus species are a significant part of the human microbiota, and are used as a probiotic supplement that has proven to be effective in the treatment of acute diarrhea in adults and infants, antibiotic-associated diarrhea and in female genital tract infections.4
There is a controversy regarding the clinical significance when isolating this microorganism from normally sterile sites. Nevertheless, its involvement in serious infections has been demonstrated.4 The risk factors related to Lactobacillus spp. infection include underlying diseases such as immunosuppression, recent surgery and prolonged antibiotic use. The most common infection caused by Lactobacillus spp. is bacteraemia either with or without endocarditis, with L. rhamnosus being the main species isolated in Europe,6 and L. salivarius in Asia.3 Identification of Lactobacillus spp. can be challenging. The variable Gram stain morphology and the slow and minimal growth on routine cultures, in association with their anaerobic requirements, can lead to an incorrect identification.7 Nevertheless, the MALDI-TOF MS method has shown a high discriminatory power when identifying these bacteria. A study comparing genomic identification versus MALDI-TOF MS showed a concordance of 96%.8
In our patient, the isolation of L. salivarius as the only bacteria can be explained by its high tolerance to gastric acid and by the fact that they produce substances such as bacteriocin, which is capable of inhibiting the growth of other bacteria.9L. salivarius is intrinsically resistant to vancomycin, as are the majority of the species in this genus. Therefore, recommended therapy consists of high doses of penicillin or ampicillin.4 However, a review of 200 cases showed that only 55% were inhibited by penicillin and 63% by ampicillin.4 This data conveys the need to study the resistance pattern of any isolate with clinical relevance. In some cases, surgery can be more effective than antibiotic treatment.10 In the case report described herein, draining the hematoma, cleaning the abdominal cavity and antibiotic treatment based on piperacillin/tazobactam was enough for the resolution of the intra-abdominal abscess.
Conflicts of interestThe authors declare that they have no conflict of interest.

