





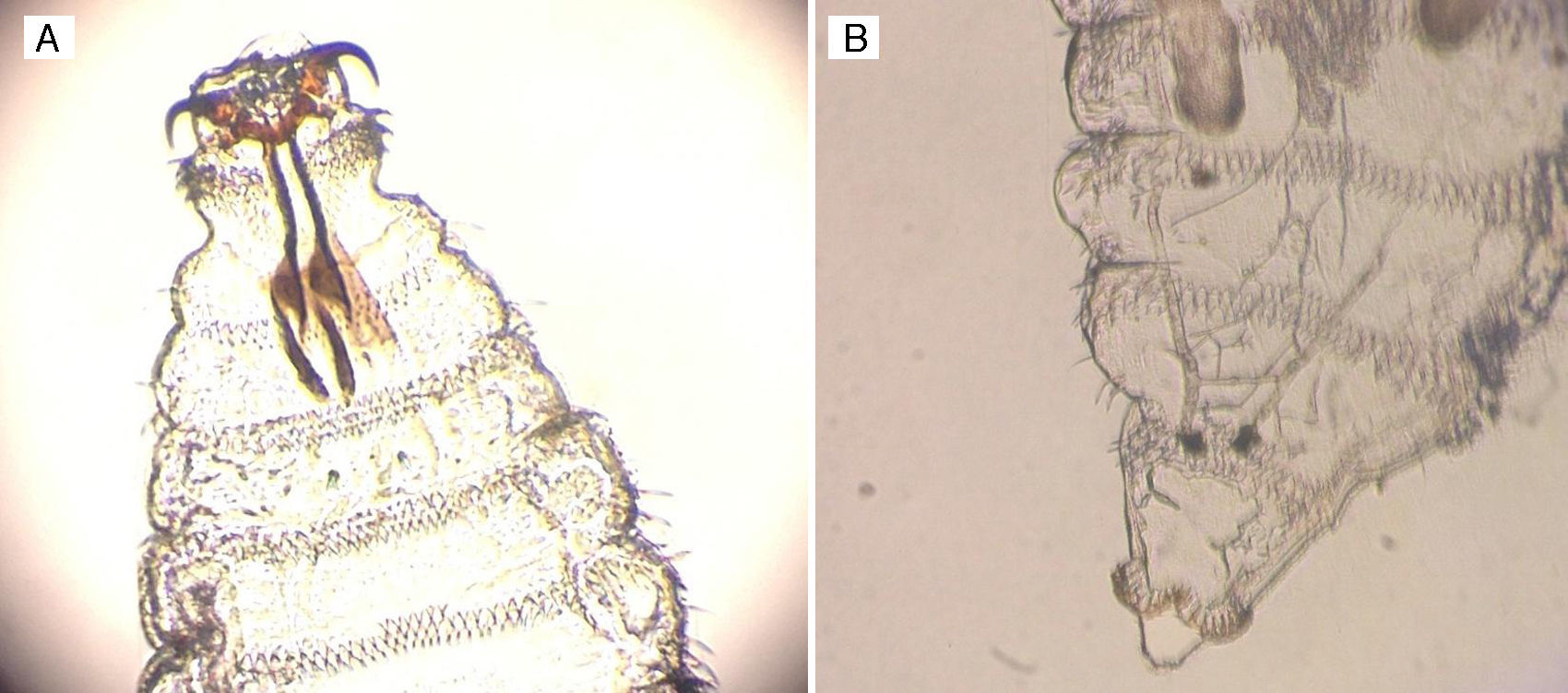
43-Year-old woman residing in the urban area of Tenerife, with no regular contact with livestock and no recent trips abroad; seen due to a foreign body sensation, pain and redness in the conjunctiva of the right eye over the course of 24h, after accidental ocular contact with a fly. Following examination, the presence of eight transparent larvae measuring 1mm in length was observed in the nasal and temporal conjunctiva, which were extracted and sent to the medical microbiology department. Here, following examination under a microscope, translucent larvae were observed, presenting an upper pole with horn-shaped mouth hooks attached to a prominent cephalopharyngeal skeleton and a caudal end with a double bulge and several hooks. They were identified as first-stage larvae (L1) of the Oestrus ovis1 species (Figs. 1 and 2).
Clinical course
 An upper pole with well developed, horn-shaped mouth hooks attached to a prominent cephalopharyngeal skeleton can be observed. (B) A caudal end can also be seen, with two terminal bulges and several spikes.")
With the diagnosis of ocular myiasis caused by Oestrus ovis and after full larvae extraction, treatment with two drops of tobramycin 3mg/ml eye drops per day and one drop of artificial tears four times daily were prescribed for one week. Fifteen days after the ocular myiasis episode, the patient reported symptoms of rhinitis which were treated with rupatadine 10mg/day for seven days, with no visible improvement, and so was referred for an ear, nose and throat consultation where, after an additional examination with a video fibrescope, the presence of a first-stage larva was observed in the left nasal cavity around the middle meatus. Following this finding and the possibility of the patient developing nasal myiasis, a single dose of ivermectin 12mg was administered, alleviating symptoms with no new episodes.
CommentsOestrus ovis is one of the species most known to cause myiasis in sheep. Their distribution is cosmopolitan, with a high prevalence in areas with warm and humid climates.2 Adult females deposit their L1 larvae in the nasal orifices of livestock, subsequently invading the paranasal sinuses and becoming stage L2 and L3 larvae. The L3 larvae then return to the nasal cavity and are expelled onto the ground through sneezing, where they continue developing into adults.2 This species occasionally causes zoonosis in humans, particularly in subjects involved in livestock farming. Ocular myiasis is the most common clinical manifestation and is primarily reported in Central America,3 South Africa4 and the Mediterranean basin,5 as well as Spain6 during the spring-summer season. This infection occurs after L1 larvae are projected onto the eyeball during the flight of adult flies, giving rise to irritative conjunctivitis caused by the action of the spikes present in the larvae on the cornea and palpebral conjunctiva.7 Nasal myiasis may also potentially develop, either due to an initial nasal infection8 or a complication of ocular myiasis. The latter is caused by the migration of L1 larvae from the eyeball to the nasal cavity,9 through the nasolacrimal duct. The case described suggests an episode of external ocular myiasis along with a probable initial case of nasal myiasis due to complications from the former. Most cases of ocular myiasis are resolved with full larvae extraction, applying anaesthetic to the conjunctival sac in order to immobilise the parasite. Topical corticosteroids and antibiotics may be used in order to prevent potential bacterial superinfections.5 However, given the possibility of developing subsequent nasal myiasis and the difficulty per se of full larvae extraction, clinical follow-up is fundamental, enabling early diagnosis of the aforementioned complication and its treatment with ivermectin.9 In the Canary Islands, reported cases of myiasis are uncommon in both humans and animals.10 However, it could be an underdiagnosed emerging disease, given the need to ship samples to the medical microbiology department for their identification. Myiasis prevention measures must be applied and considered in animals.2,7
FundingThe authors declare that they did not receive funding to complete this study.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Sante Fernández L, Hernández-Porto M, Tinguaro V, Lecuona Fernández M. Oftalmomiasis y miasis nasal por Oestrus ovis en paciente residente en las Islas Canarias con características epidemiológicas poco frecuentes. Enferm Infecc Microbiol Clin. 2017;35:461–462.
