




Infectious diseases have been a major cause of morbidity and mortality throughout human history, and – although it might have seemed in the late 20th century that they would no longer be a global health problem – recent events indicate that infectious diseases continue to be an ever-changing global challenge.1 Just take the examples of the HIV/AIDS disease, avian flu outbreaks, the Ebola virus, the SARS-CoV-2 pandemic and now the monkeypox virus.1–4 Added to this are the complex infections encountered in immunocompromised and transplanted patients, the foreign-body device infections that result from the development of medical technology, and the appearance of infections caused by multi- or extremely drug resistant microorganisms.1 Now more than ever, therefore, Spain needs the Specialty of infectious diseases (ID); it is the only Member State of the European Union without it.5 Accordingly, we have conducted a survey exploring the consequences expected in 2040.
The survey was performed in March 2022 and take part 20 Spanish physicians dedicated to infectious diseases: 10 under 45 years of age (Junior specialists) from the province of Barcelona, 10 over 45 years of age (Senior specialists) from Spain, and 14 senior international infectious disease specialists. All were asked four questions: (1) Will the ID specialty exist in 2040? (Spanish specialists) or, what role will the ID specialty play in 2040? (International specialists), (2) What infectious diseases will be most frequent in 2040? (3) What infectious diseases will have decreased or disappeared in 2040? and, (4) What will be the most important innovations in microbiological diagnosis?
Participation rates at the Spanish and international levels were 100% (20/20) and 71% (10/14), respectively. The proportions of males amongst the respondents were 50%, 90% and 80% in Spanish Junior, Spanish Senior and International Specialists, respectively. Three Spanish specialists were from Madrid, two each from Barcelona and Seville and one each from Córdoba, Granada and Donostia. The International Specialists were from USA in five cases and from Europe (Croatia, France, Italy, Netherlands and Switzerland) in the other five cases.
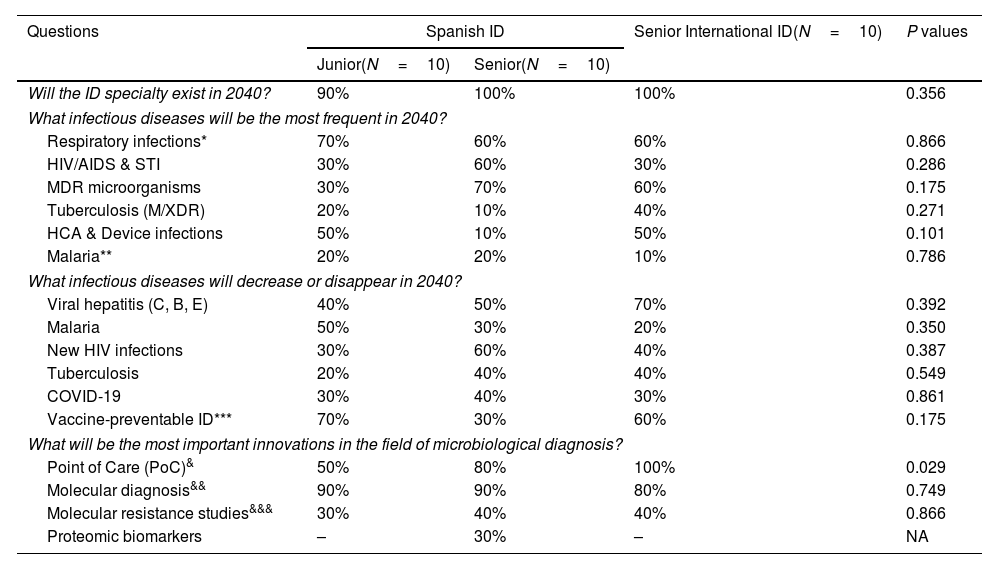
Table 1 depicts the most frequent responses. Ninety-five percent of Spanish Specialists believe the ID Specialty will exist, and all International Specialists believe the ID Specialty will have a more important role at all levels. Regarding emerging infections, the majority believe that respiratory infections (including coronavirus and influenza), HIV and sexually transmitted infections, multidrug/extensively drug resistant microorganisms including tuberculosis, health-care associated infections, device-related infections will be more frequent and that malaria will be diagnosed in non-tropical countries. With regard receding infections, they mentioned the hepatitis viruses (C, B, E) and vaccine-preventable infections, malaria, new HIV infections, tuberculosis and COVID-19. The seeming contradiction of HIV/AIDS infection appearing in both responses is understandable, as on the one hand, universal antiretroviral treatment (treatment as prevention) and HIV pre-exposure prophylaxis (PrEP) mean new HIV infections will decrease, whereas, on the other hand, the life expectancy of people living with HIV will approach that of the general population, increasing the volume of cases and creating an inverted pyramid population with fewer young people affected, but a larger elderly population with HIV, as predicted by UNAIDS.6 Finally, regarding innovation in microbiological diagnosis, all surveyed suggested that point of care (PoC) diagnosis with rapid testing of blood and other biological samples will become part of routine clinical care, as will the molecular diagnosis of infectious diseases and antimicrobial resistance using next-generation or genome-wide sequencing and bacterial, viral and fungal cell free DNA in the blood, and real-time molecular diagnostic panels. Overall, there were not statistically significant differences in all responses among the three groups except in the diagnosis through the point of care, which was less frequent in the Spanish junior specialists.
Main results of the Infectious Diseases challenges for 2040.
| Questions | Spanish ID | Senior International ID(N=10) | P values | |
|---|---|---|---|---|
| Junior(N=10) | Senior(N=10) | |||
| Will the ID specialty exist in 2040? | 90% | 100% | 100% | 0.356 |
| What infectious diseases will be the most frequent in 2040? | ||||
| Respiratory infections* | 70% | 60% | 60% | 0.866 |
| HIV/AIDS & STI | 30% | 60% | 30% | 0.286 |
| MDR microorganisms | 30% | 70% | 60% | 0.175 |
| Tuberculosis (M/XDR) | 20% | 10% | 40% | 0.271 |
| HCA & Device infections | 50% | 10% | 50% | 0.101 |
| Malaria** | 20% | 20% | 10% | 0.786 |
| What infectious diseases will decrease or disappear in 2040? | ||||
| Viral hepatitis (C, B, E) | 40% | 50% | 70% | 0.392 |
| Malaria | 50% | 30% | 20% | 0.350 |
| New HIV infections | 30% | 60% | 40% | 0.387 |
| Tuberculosis | 20% | 40% | 40% | 0.549 |
| COVID-19 | 30% | 40% | 30% | 0.861 |
| Vaccine-preventable ID*** | 70% | 30% | 60% | 0.175 |
| What will be the most important innovations in the field of microbiological diagnosis? | ||||
| Point of Care (PoC)& | 50% | 80% | 100% | 0.029 |
| Molecular diagnosis&& | 90% | 90% | 80% | 0.749 |
| Molecular resistance studies&&& | 30% | 40% | 40% | 0.866 |
| Proteomic biomarkers | – | 30% | – | NA |
*Mostly viral infections (influenza, coronavirus, other respiratory viruses, including pandemic strains); **In non-tropical countries due to climate change; ***Measles, rubella, mumps, poliomyelitis, meningococcus, pneumococcus, tetanus, varicella and human papillomavirus-induced cervical cancer; &Rapid tests on blood and other biological samples; &&NGS: Next-Generation Sequencing; GWS: genome-wide sequencing, bacterial, viral and fungal cell free DNA in blood; real-time molecular diagnostic panels; &&&Real-time resistance diagnosis.
Abbreviations: HCA: health-care associated infections; HIV: human immunodeficiency virus; ID: Infectious Diseases; STI: sexually transmitted infections. MDR: multidrug-resistant; XDR: extensively drug resistant; NA: not applicable.
Spain must prepare for all of these ID challenges, working closely with Spanish microbiologists. The Specialty must be created and its specialists trained through the national medical interns and residents’ program (MIR), following the infectious diseases section of the European Union of Medical Specialists (UEMS-ID) guidelines.5 In addition, future Spanish ID specialists should pass the European Board of Infectious Diseases Examination to be able to practice ID in any European Union Member State. The recent approval of the Royal Decree on Specialties in Spain7 should make this possible. Spanish society cannot wait any longer; it cannot be at a disadvantage compared to other European countries. Spain needs ID specialists to deal with current and future global health challenges.
FundingJMM received a personal 80:20 research grant from Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain, during 2017–23.
Conflict of interestJMM has received consulting honoraria and/or research grants from Angelini, Contrafect, Genentech, Gilead Sciences, Jansen, Medtronic, Lysovant, MSD, Novartis, Pfizer, and ViiV Healthcare, outside the submitted work. Other authors no conflicts.
The content of this article was presented in part at the Catalan Society of Infectious Diseases and Clinical Microbiology Society (SCMIMC) in Barcelona, Spain on March 17th 2022.
We are especially grateful for the selfless collaboration of the following specialists:
Spanish Junior infectious diseases specialists from Barcelona city and province hospitals: Ambrosioni J, Boix L, Cuervo G, Gasch O, Grillo S, Hernández-Meneses MM, Pericas JM, Puerta P, Suazes P, Torres B.
Spanish Senior infectious diseases specialists from the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC): Arribas JR, Canton R, Cisneros JM, García F, Iribarren JA, Moreno-Camacho A, Moreno-Guillén S, Rivero R, Rodriguez-Baño J, Trilla A.
International infectious diseases specialists from the International Society of Cardiovascular Infectious Diseases (ISCVID) executive committee: Barsic B (Croatia), Bayer A (USA), Chu V (USA), Durack D (USA), Durante-Mangoni E (Italy), Fowler V (USA), Hasse B (Switzerland), Hoen B (France), Karchmer AW (USA), van der Meer J (Netherlands). We are indebted to Dr. Jaume Llopis (Department of Genetics, Microbiology and Statistics, Faculty of Biology, University of Barcelona, Barcelona, Spain) for perform the statistical analysis
