




The COVID-19 pandemic has been accompanied by uncertainty. The need for tests to diagnose it in real time has led to tests being developed in record time, without the validation that would have been required in other circumstances.
Techniques based on protein detection offer theoretical advantages over those based on RNA amplification (which are more costly, slow and require sophisticated equipment)1 and were included in the COVID-19 diagnostic protocols.2
SARS-CoV-2 antigen (Ag) determination (2019-nCoV Ag Test Fluorescence IC Assay® Shenzhen Bioeasy Biotechnology CO LTD, China, read with Bioeasy Immunofluorescence Analyzer mod EASY-11 Ref YRLE1105), which detects nucleocapsid protein, became available at the beginning of April. According to the manufacturer, the sample needed to be transported in a specific medium and preferably processed within 30 min of being taken, although the summary of product characteristics allows it to be carried out within 24 h and describes a sensitivity (SE) and specificity (SP) of 92% and 100%, respectively.
Our centre's COVID-19 working group decided to include this determination in patients with respiratory symptoms of less than 7 days' evolution, following expert recommendations.3 Nasal samples were collected and processed within a maximum of 30 min. If the result was negative, a polymerase chain reaction (PCR) test was performed. After one week of using the Ag test, doubts arose concerning its accuracy (positive results in asymptomatic patients for whom Ag tests had been ordered in spite of their not being included in the protocol's indications). It was therefore decided a posteriori to confirm all results with PCR.
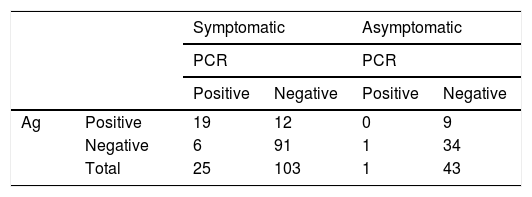
Between 6 and 17 April, Ag detection was performed in 193 patients (44 asymptomatic, not anticipated in the protocol). In 172, samples were available for PCR (Table 1).
Taking the PCR as a benchmark, the SE, SP, positive predictive value (PPV) and negative predictive value (NPV) of the Ag test in symptomatic patients were 76%, 88.33%, 61.3% and 93.8%, respectively. The concordance in asymptomatic patients was much lower.
Cases with discordant results were analysed using clinical/radiological assessment, earlier/later PCR results and serological data where available. Of the 21 patients with positive Ag/negative PCR, 13 were considered Ag false positives (FPs) (9 asymptomatic and 4 symptomatic with subsequent negative serology). In the remaining 8 patients, the clinical and epidemiological picture was compatible with a COVID-19 diagnosis, no other microbiological tests were carried out and they were considered PCR false negatives (FNs).
Of the 7 patients with negative Ag/positive PCR, one case was asymptomatic and in the rest the duration of the symptoms ranged from one to 18 days (median 4 days). In 4 patients, subsequent positive serology was available. All were considered to be Ag FNs.
If we consider clinical and radiological criteria, serology and earlier/later PCRs to define COVID cases, the SE, SP, PPV and NPV of Ag in symptomatic patients were 79.4%, 95.7%, 87.1% and 92.8%.
The discrepancies in the results may be because the Ag/PCR determinations were performed on different samples (although obtained on the same day) and because neither of the techniques has 100% SE and SP, with PCR, according to Börger's meta-analysis, having an SE of 73.3% (95% CI: 68.1–78.0).4
At our centre, the Ag determination was withdrawn due to the discordance of the results with PCR, the difficulties entailed by the limited time for processing and the need for a different transport medium than PCR, which required two samples to be taken. These disadvantages should be reconsidered in light of recent studies: Porte et al.5 kept samples refrigerated for 48 h with excellent results, thereby overcoming the time limitation, and other studies used a universal viral transport medium5,6 instead of that proposed by the manufacturer, thereby saving material, time and discomfort for the patient, there being no need to obtain a second sample for PCR.
The WHO currently recommends PCR as the technique of choice for COVID-19 diagnosis,7 but knowledge of the performance, advantages and limitations of tests taken at different times/on different samples/in different pandemic settings may help in developing suitable strategies for future situations. Based on our results and those of recent publications, Ag determination may be useful in symptomatic patients.
FundingThis study was partially funded through a call for proposals by the Department of Health of the Autonomous Government of Catalonia, code 6-17, principal investigator: Francesc Vidal.
Please cite this article as: Parada-Ricart E, Gomez-Bertomeu F, Picó-Plana E, Olona-Cabases M. Utilidad del antígeno para el diagnóstico de infección por SARS-CoV-2 en pacientes con y sin síntomas. Enferm Infecc Microbiol Clin. 2021;39:357–358.
