




Acute respiratory infections of viral cause are very frequent entities. The difficulty in evaluating the detection of a virus in these entities could be solved by determining the viral load.
MethodsA prospective study on the mean Ct value (cycle threshold value) detected against RSV-A, RSV-B and influenza A (H1N1)pdm09, A (H3N2) and B viruses in patients of different origin and age was performed. Detection was performed using a commercial molecular amplification (RT-PCR) technique.
ResultsDifferent mean Ct values were detected for each virus. In RSV infections, no differences were observed between those caused by RSV-A or RSV-B in children. Depending on the patient's age, the only statistical significance was observed in those included in the 0–4 month groups for RSV-A and this group and the 5–12 months group for RSV-B (higher values). A lower viral load was detected in adult patients than in paediatric patients. In influenza infections, no statistical significance was observed in the mean values detected in patients from the Red Centinela (“sentinel network”, a Spanish network of doctors aimed at research and surveillance of diseases), those diagnosed in the adult emergency room or in hospital admissions. In the adult patients admitted to the ICU, only a slightly lower mean value was observed in those infected with influenza A (H1N1)pdm09, but without statistical significance. There were no patients admitted to the ICU with influenza B infection.
ConclusionThe detection of viral load could be a good tool for the evaluation, monitoring and prognosis of acute viral respiratory infections. With the exception of those caused by RSV, no significant differences were observed in influenza infections except in younger paediatric patients.
Las infecciones respiratorias agudas de causa viral son unas entidades muy frecuentes. La dificultad para valorar la detección de un determinado virus en estas entidades podría solucionarse con la determinación de la carga viral.
MétodosSe ha realizado un estudio prospectivo sobre el valor medio de los Ct (cycle threshold value) detectados frente al VRS-A, VRS-B y los virus gripales A (H1N1)pdm09, A(H3N2) y B en pacientes de diferente procedencia y edad. La detección se ha realizado mediante una técnica de amplificación molecular (RT-PCR) comercial.
ResultadosSe han detectado valores medios de Ct distintos para cada virus. En las infecciones por VRS, no se han observado diferencias entre las causadas por el VRS-A o VRS-B en pediatría. De acuerdo con la edad de los pacientes solo se ha observado significación estadística en los incluidos en los grupos de 0-4 meses para el VRS-A y este grupo y el de 5-12 meses para el VRS-B (valores más elevados). En los pacientes adultos se ha detectado una carga viral menor que en los pediátricos.
En las infecciones gripales no se ha observado significación estadística en los valores medios detectados en los pacientes procedentes de la Red Centinela, en los diagnosticados en las urgencias de adultos ni en los ingresados hospitalarios. En los pacientes adultos ingresados en la UCI solo se ha observado un valor medio algo más bajo en los infectados por el virus gripal A (H1N1)pdm09 pero sin significación estadística. No hubo ningún paciente ingresado en la UCI con infección por gripe B.
ConclusiónLa detección de la carga viral podría ser una buena herramienta para la evaluación, seguimiento y pronóstico de las infecciones respiratorias agudas víricas. A excepción de las causadas por el VRS, no se han observado diferencias significativas en las infecciones gripales, salvo en los pacientes pediátricos de menor edad.
Acute respiratory infections (ARIs) of viral cause are entities which affect the entire population, although their morbidity peaks at the start or end of life. Most of these infections occur each year during the winter, resulting in the so-called epidemic seasons, basically assigned to those caused by the respiratory syncytial virus (RSV) in the infant population1 and to that caused by influenza in the general population.2
Molecular biology techniques applied to establishing the viral aetiology of ARIs has made it possible in recent years to determine the range of viruses involved in these conditions.3 Despite this, RSV and influenza are the viruses with the greatest impact on public health, which should be actively monitored.1,2
Detection using molecular techniques, generally reverse transcription polymerase chain reaction (RT-PCR), of a specific virus in a respiratory sample of a patient with an ARI is usually considered to be a definitive aetiological diagnosis, as it is detected in less than 2% of asymptomatic patients.4 However, the clinical translation of this virus means that its presence can be detected both in mild catarrhal or respiratory processes as well as severe respiratory symptoms with a risk of associated mortality.1,2
One option for trying to predict or determine the significance of a virus in these patients would be the quantification of the viral load in the respiratory sample. The hypothesis would be that with a higher viral load there is higher morbidity or mortality associated with the infectious process.5–7
For the past three years, we have been using a commercial RT-PCR technique for this viral diagnosis. It is initially qualitative, i.e. it detects whether the viruses are present or absent. However, the Ct (cycle threshold) value is presented in the final result. This expresses the cycle in which the detection system considers that the sample is positive for a certain virus (its value ranges between 0 and 40).3 In this way, the samples with a high viral load have a low Ct value and those with a low viral load have a higher Ct value (they need more amplification cycles to cross the positivity threshold).
With this concept and the Ct value obtained in each respiratory sample, we studied the ARIs caused by RSV and influenza viruses, and analysed its mean value in different age groups and hospital location.
Material and methodsA prospective study was carried out on the mean Ct value of patients with an ARI caused by RSV and influenza viruses. All respiratory samples, nasopharyngeal aspirate for children <3 years-old and pharyngeal smears for children <3 years-old, were analysed using a commercial molecular technique (RT-PCR), which simultaneously and differentially detects 19 different respiratory viruses (Allplex, Seegen; North Korea). In addition to the sample being positive, the Ct value, in which the automated detection system considered the sample of a specific virus to be positive, was recorded. RSV antigen detection was performed in 77 samples using commercial immunochromatography (Binax RSV, Alere, Barcelona).
To avoid bias, the first 150 respiratory samples positive for RSV-A, RSV-B, influenza A (H1N1)pdm09, influenza A (H3N2) and influenza B (total 750 samples) were analysed. For this, the influenza A (H1N1)pdm09 and influenza B values corresponded to the 2015–2016 influenza season (due to its predominance) and the influenza A (H3N2) values corresponded to the cases from the 2016–2017 season (for the same reason). To avoid interference, samples which had co-infections with any of the viruses studied were removed. The Ct values of patients with RSV-A and RSV-B corresponded to both seasons.
The patients were classified according to age, children (<14 years) or adults (>14 years). In the ARIs caused by RSV, a classification was made between those that presented with a single viral infection and those that presented with a mixed infection (co-infection). Similarly, the mean value of the Cts was evaluated in relation to the samples which were previously positive in the antigen detection test (only in the paediatric population).
Patients with an ARI caused by the influenza viruses were classified in terms of their location at the time positivity was detected, into the following groups: those from the influenza sentinel surveillance network (SN), those from adult hospital emergency departments (AHED), those admitted to the Intensive Care Unit (ICU) and paediatrics.
Statistical analyses were performed using the SPSS 21 program (http://www.spss.com), considering p<0.05 as a significant value.
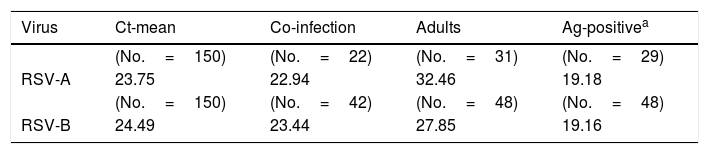
ResultsThe mean Ct value detected in the samples positive for RSV-A was 23.75 (range 17.02–33.76) and 24.49 for RSV-B (range 15.29–36.68). In patients with co-infection with another respiratory virus, its mean value was 22.94 for RSV-A and 23.44 for RSV-B.
A significant difference was noted between the mean Ct value observed and that observed in adult patients infected with RSV-A (32.46; p<0.05) and with RSV-B (27.85; p<0.05). This significance was also observed in those samples which were positive in the antigen detection test, both for RSV-A (19.18; p<0.05) and for RSV-B (19.16; p<0.05) (Table 1).
Ct values detected in the samples with presence of respiratory syncytial virus.
| Virus | Ct-mean | Co-infection | Adults | Ag-positivea |
|---|---|---|---|---|
| (No.=150) | (No.=22) | (No.=31) | (No.=29) | |
| RSV-A | 23.75 | 22.94 | 32.46 | 19.18 |
| (No.=150) | (No.=42) | (No.=48) | (No.=48) | |
| RSV-B | 24.49 | 23.44 | 27.85 | 19.16 |
RSV-A: respiratory syncytial virus type A; RSV-B: respiratory syncytial virus type B.
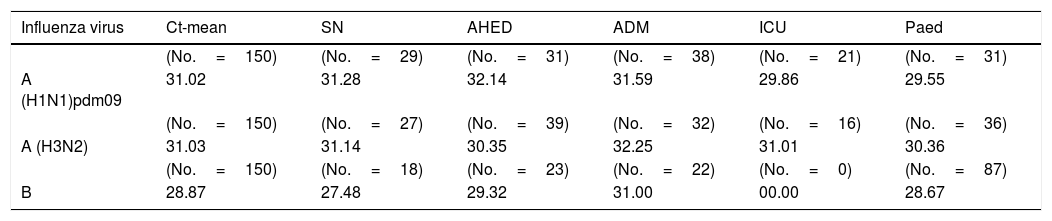
The mean Ct value observed in the patients with infection caused by the influenza A virus (H1N1)pdm09 was 31.02 (range 19.09–38.59), 31.03 for influenza A virus (H3N2) (range 21.74–39.34) and 28.87 for influenza B virus (range 21.16–38.72).
For influenza infections, no statistical significance was observed in the mean values detected in patients from the SN, in those diagnosed in AHEDs or in those admitted to hospital. In the adult patients admitted to the ICU, only a somewhat lower mean value was observed in those infected with influenza A virus (H1N1)pdm09, but with no statistical significance. No patient admitted to the ICU had influenza B infection (Table 2).
Ct values detected in the samples with presence of influenza A and B viruses.
| Influenza virus | Ct-mean | SN | AHED | ADM | ICU | Paed |
|---|---|---|---|---|---|---|
| (No.=150) | (No.=29) | (No.=31) | (No.=38) | (No.=21) | (No.=31) | |
| A (H1N1)pdm09 | 31.02 | 31.28 | 32.14 | 31.59 | 29.86 | 29.55 |
| (No.=150) | (No.=27) | (No.=39) | (No.=32) | (No.=16) | (No.=36) | |
| A (H3N2) | 31.03 | 31.14 | 30.35 | 32.25 | 31.01 | 30.36 |
| (No.=150) | (No.=18) | (No.=23) | (No.=22) | (No.=0) | (No.=87) | |
| B | 28.87 | 27.48 | 29.32 | 31.00 | 00.00 | 28.67 |
ADM: admitted patients; AHED: adult hospital emergency department; ICU: intensive care unit; Paed: paediatric patients (<14 years of age); SN: sentinel network.
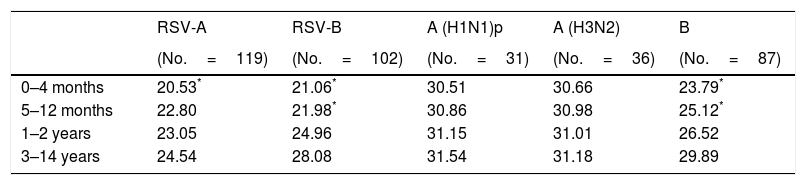
In accordance with the age of the paediatric patients, statistical significance was only observed in the mean Ct value of the patients included in the 0–4 months group for RSV-A and this group and the 5–12 months group for RSV-B (Table 3).
Mean Ct values detected in samples positive for respiratory syncytial virus and for influenza viruses in paediatric patients.
| RSV-A | RSV-B | A (H1N1)p | A (H3N2) | B | |
|---|---|---|---|---|---|
| (No.=119) | (No.=102) | (No.=31) | (No.=36) | (No.=87) | |
| 0–4 months | 20.53* | 21.06* | 30.51 | 30.66 | 23.79* |
| 5–12 months | 22.80 | 21.98* | 30.86 | 30.98 | 25.12* |
| 1–2 years | 23.05 | 24.96 | 31.15 | 31.01 | 26.52 |
| 3–14 years | 24.54 | 28.08 | 31.54 | 31.18 | 29.89 |
RSV-A: respiratory syncytial virus type A; RSV-B: respiratory syncytial virus type B.
Paediatric influenza infections also failed to show overall significant differences in Ct values. By age group, only patients included in the 0–4 months and 5–12 months groups and those infected by the influenza B virus showed a lower mean value (p>0.05) (Table 3).
DiscussionThe mean Ct values detected in ARIs caused by RSV-A and B showed similar results with no significant differences. It is difficult to compare these values with those reported in other studies as it is likely that the values may vary in each molecular detection system. Despite this, Fuller et al.6 obtained a mean value of 27.20 for RSV without differentiating the viral type.
In the study conducted by Borg et al.,8 a relationship was established between the RSV load (copies/ml) and the Ct value obtained in the amplification process. According to this study, a mean value of 24 (similar to ours) would correspond to a mean load of 1×105copies/ml.8 Also using the number of copies/ml, Do et al.5 confirmed that the RSV viral load is higher in paediatric patients who require admission to intensive care (3.8×107copies/ml) than those who are not admitted (2.5×106copies/ml).
In our study, we were not able to observe Ct values of RSV-A or RSV-B that were lower in co-infections with other respiratory viruses as reported in other studies.9 However, we did not check the value for the associated virus.
ARIs caused by RSV in the adult population continue to be an uncommon entity, although it seems that it is increasing, probably due to the use of molecular detection techniques.10 The mean Ct values detected in adult patients with an ARI caused by RSV were found to be significantly higher, both for RSV-A and RSV-B, than the mean value of these viruses. This finding seems to indicate that the viral load in this group of patients is lower than that observed in paediatric patients and that the underlying conditions of these patients are probably the predisposing factor for these infections.
However, in a study on 123 patients, Lee et al.11 observed that hospitalised adults presented high concentrations of RSV RNA at the time of admission, and also that the higher viral load was related to the development of complications and admissions to the ICU.
We studied the mean Ct value detected in paediatric patients with positive antigen detection before performing molecular amplification. The mean value was very similar in both types of RSV (19.18 vs 19.16) and significantly lower, and therefore with a higher viral load, than the overall mean value. This result is logical as the sensitivity of most rapid techniques is not very high. According to the study by Borg et al.,8 1×106copies/ml would correspond to this mean value. This could be the limit of detection of our antigen technique. In the study by Moesker et al.,12 in which they used the same commercial system as us in the antigen detection for RSV, they established that the false-negative samples are due to high Ct values, i.e. to low viral loads, confirming our results.
We have not found studies that make it possible to compare results obtained for RSV in different age groups. Our data support the general idea that at a younger age there is a higher viral load, and this seems to be confirmed in this study. The age groups with a lower mean Ct value, compared to the overall value, are younger than 12 months, both for RSV-A and RSV-B.
In our study, the mean Ct value of the influenza A (H1N1)pdm09 and A (H3N2) viruses was very similar; while that observed for influenza B virus (28.87) was lower, although they should probably not be compared with each other as different amplification targets were used. No differences were observed in patients from the community (sentinel network, SN), with mean values similar to those detected in patients who were diagnosed in the AHEDs. Spencer et al.7 observed that the mean Ct value of patients with influenza A (without specifying) was 26.9 and with influenza B was 25.3. As has been mentioned, the use of different molecular techniques does not allow comparisons to be made.
We also did not observe differences between admitted patients and those treated in AHEDs. Only those patients who required admission to the ICU showed a mean Ct value somewhat lower for influenza A (H1N1)pdm09 virus, but not for A (H3N2) virus. These data seem to indicate that the value of the viral load present in the respiratory samples is not the decisive factor for hospital or ICU admission, but probably the age and underlying conditions which these patients present with.13
In the case of influenza B, no significant differences were observed in any of the groups studied. Even in admitted patients the mean Ct value was somewhat higher than the mean (lower viral load). As with influenza A, Lee et al.14,15 also reported a higher load of this virus in patients who were admitted to hospital. We did not analyse any patient with influenza B admitted to the ICU, as it preferentially affects the paediatric population.
The analysis of influenza infections in the paediatric age group did not show significant differences in any of the influenza types. For the influenza A viruses the value was somewhat lower, but not significant, and for the B virus it almost matched the mean value. This is due to the fact that 58% of all patients in this study were under 14 years of age.
When analysing the paediatric influenza infections by age groups, significant differences were only observed in influenza B virus in the 0–4 months and 5–12 months groups. This means that patients less than one-year-old seem to present a higher viral load than all other patients. No other studies in which the viral load of paediatric patients with influenza B is analysed have been found. This means that these data cannot be compared with other previous data.
In summary, in the case of ARIs caused by RSV, we were able to show how the viral load seems to be higher in children than in adults, and that direct antigen detection could only be positive with values below the mean. In influenza infection, we detected minimal differences between the different Ct values of the groups studied.
Conflicts of interestThe authors declare that they have no conflicts of interest.
We would like to express our gratitude to all the technical personnel who have collaborated with the Virology Unit of the Hospital Universitario Son Dureta/Son Espases over the past 23 years.
Please cite this article as: Reina J, Morales C, Busquets M, Norte C. Utilidad del valor Ct en las infecciones respiratorias agudas causadas por el virus respiratorio sincitial A y B y los virus gripales A (H1N1)pdm09, A (H3N2) y B. Enferm Infecc Microbiol Clin. 2018;36:332–335.
