








Cases of trauma still becomes a health problem in almost all countries causing death in few cases. In some developing countries, the insidences of head injury tend to increase. One of the reasons for the many death and disability may be due to the inavailability and inadequacy of pre-hospital first aid.
AimThe general objective of this study is to find out the description of community first responder in providing pre-hospital first aid to head injuries.
MethodsThis study uses qualitative descriptive method.
ResultsMost of the respondents have variety of educational backgrounds and do not have sufficient knowledge and skills to provide first aid. The average respondents provided help by performing initial assessment, managing effective airway and controlling bleeding. Limited pre-hospital facilities become one of the reasons for respondent not getting help so the efforts provided are not maximal. Respondents prefer to send patients directly to health facilities.
ConclusionRegular education and training programs for the community first responders should be initiated so that the number of death and disability can be minimized.
Head injury is a traumatic disorder of brain function accompanied by or without interstitial hemorrhage in the brain without the continuation of discontinuation of the functioning of the brain. The consequence of the injury varies in grade and may result in many other effects including death and disability in children and adults in their productive age.1 These often lead to complex health problems as their long periods of care and recovery which consequently leads to high cost even problems in social as well as economic stability and other problems.2 Elderly people are one of the age group that are very vulnerable to head trauma. The research conducted by Rubenson Wahlin et al. (2016)3 showed that injuries in the third order were high among elderly to about 26.84% (n=102). This finding is reinforced by other studies4 where out of 1000 head injury patients, 31.2% (n=312) patients were aged between 21 and 40 years who constitute the highest number followed by age 41–60 years (28.6%) and third place aged 0–20 years (21.1%). Traffic accidents almost dominate the causes of trauma in almost all countries, followed by falls, riots, sports injuries and other causes. Another study2 also found that 41.7% of the injuries were caused by traffic accidents. The success of help is greatly influenced by various things, one of which is pre-hospital emergency care. The speed of finding help, providing the right help and proper referral to appropriate and safe health services greatly determines the success of help. First aid for head injuries plays an important role in saving the victim from disability even from death. When pre-hospital first aid is not provided approprietely, it will reduce the quality of care. By early initial assessment and appropriate emergency care it may reduce death or disability.
The human brain contains various commands that are integrated into the body's functions and movement.5 There are several factors that can affect the level of intelligence and ability to function depending on brain size. Disease and sudden changes such as trauma can caused brain injuries. Brain disorders can occur suddenly due to a significant trauma process or primary trauma or can also occur following long process of trauma for several days.2 Therefore, it is not surprising when the brain is injured, then some or all the processes in the body will be affected as well. Head injuries can be categorized into several types including mild, moderate and severe based on three measurement parameters, namely Glasgow Coma Scale (GCS), the period of post-traumatic amnesia and period of loss of consciousness.6 Each class shows little different manifestation, depending on the severe of the injury.
Trauma to the head causes the skull and its contents to vibrate. The damage caused depends on the amount of vibration. The vibrations from the collision will proceed to galea aponeurotica causing damage to brain's protection. This causes the cerebral blood vessels to tear and epidural, subdural and intracranial hematomas. The bleeding will affect the blood circulation to the brain resulting in decreased oxygen supply and tissue hypoxia occurs causing cerebral edema. As a result, distortion of the brain occurs as the contents of the brain are pushed in the opposite direction. This leads to an increase in intracranial pressure which stimulates the pituitary gland and adrenal steroids. Finally, the secretion of stomach acid increases causing nausea even vomiting.7
The vital role of the first responders is to handle pre-hospital trauma to prevent further harm or prevent death. It is necessary to take careful steps in first aid, especially related to a decrease consciousness, decrease in body temperature and bleeding. These steps include providing initial assessment, basic life support and various other emergencies as well as the process of evacuating or transporting clients.
MethodsThis study has been conducted from March to October 2018 in 7 emergency units of public hospitals in Central Java including Surakarta, Klaten, Sukoharjo, Wonogiri, Sragen, Karanganyar and Boyolali. The sampling technique in this study is total sample technique, where all population is recruited as a sample meeting the inclusion criteria. Ethical clearance was gained from the School of Nursing of Health Polytechnic of Surakarta in order to ensure the ethic regulation.
ResultsFrom 155 questionnaires delivered, 130 (84%) were returned. After selecting and editing, 116 (74%) questionnaire met the final decision for continuing data analysis. Demographic data from this study comprises of gender, aged and educational background as can be seen in Table 1.
Distribution of respondent according to gender, aged and educational background.
| No | Gender | Frequency | Percentage (%) |
|---|---|---|---|
| 1 | Male | 92 | 79.3 |
| 2 | Female | 24 | 20.7 |
| Total | 116 | 100% | |
| No | Age | Frequency | Percentage (%) |
| 1 | <30 year | 38 | 32.8 |
| 2 | 30–50 year | 45 | 38.8 |
| 3 | >50 | 33 | 28.4 |
| Total | 116 | 100% | |
| No | Education | Frequency | Percentage (%) |
| 1 | Elementary school | 8 | 6.9 |
| 2 | Junior high school | 23 | 19.6 |
| 3 | Senior high scool | 48 | 41.4 |
| 4 | Three year degree | 18 | 15.5 |
| 5 | Bachelor | 19 | 16.4 |
| Total | 116 | 100% |
As can be seen from Table 1, male dominated as the first responder providing first help that contribute to 79.3%. Respondent at the age between 30 and 50 years old leads the number by 38.8% followed by age under 30 years old 32.8% and more than 50 years old 28.4%. Respondent with Senior High School educational background are the majority responders (41.4%) followed by respondent in Junior High School (19.6%). The interesting finding is from bachelor background, where from 19 respondents, there are 1 general practitioner, 6 nurse and 1 security with first aid training.
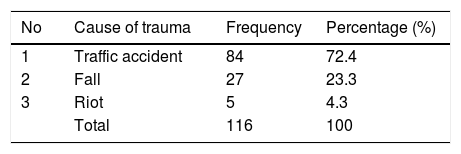
The following results are grouped into four categories such as cause of trauma, initial assessment, stabilization and referral. The initial assessments are illustrated in Table 2.
It is clear from Table 2 that the most common cause of head injury was traffic accident (72.4%). Fall is the second highest (23.3%) cause of trauma.
Table 3 shows that all responder performed initial assessment by calling the victims (93.1%). Eight respondents performed assessment by checking pain, pulse and breath. After checking the level of consciousness, victims were positioned as supine. (61.2%; n=71). In order to get enough oxygen, it is important to remove helmet safely. Only 27.6% respondents (n=32) performed this steps. Most of them did not remove helmet as major reason being they were not sure of the steps to be taken. They did not remove helmet being afraid of negative effect from the removal manuver. The majority of the respondents (69.8%) did maintain proper ventilation. Most of the respondent did not now what to do to and did not know the way to maintain open airway.
Distribution of respondent according to the initial assessment and management.
| No | Initial assessment | Frequency | Percentage (%) |
|---|---|---|---|
| 1 | Call the victims | 108 | 93.1 |
| 2 | Pain sensation, check for pulse and breating | 8 | 6.9 |
| Total | 116 | 100 | |
| No | Positioning victim on supine | Frequency | Percentage (%) |
| 1 | Yes | 71 | 61.2 |
| 2 | No | 45 | 38.8 |
| Total | 116 | 100 | |
| No | Removing helmet | Frequency | Percentage (%) |
| 1 | Yes | 32 | 27.6 |
| 2 | No | 84 | 72.4 |
| Total | 116 | 100 | |
| No | Maintaining open airway | Frequency | Percentage (%) |
| 1 | Yes | 81 | 69.8 |
| 2 | No | 35 | 30.2 |
| Total | 116 | 100 |
The next findings respondents were asked to stabilize the victim, prevent foreign object penetration, control bleeding and closing wound as described in Table 4.
Distribution of respondent according to providing stabilization.
| No | Head and neck Immobilization | Frequency | Percentage (%) |
|---|---|---|---|
| 1 | Yes | 57 | 49.1 |
| 2 | No | 59 | 50.9 |
| Total | 116 | 100 | |
| No | Removing foreign object | Frequency | Percentage (%) |
| 1 | Yes | 57 | 49.1 |
| 2 | No | 59 | 50.9 |
| Total | 116 | 100 | |
| No | Controling bleeding | Frequency | Percentage (%) |
| 1 | Yes | 75 | 64.7 |
| 2 | No | 41 | 35.3 |
| Total | 116 | 100 | |
| No | Clossing wound | Frequency | Percentage (%) |
| 1 | Yes | 69 | 59.5 |
| 2 | No | 47 | 40.5 |
| Total | 116 | 100 |
Table 4 shows about half of the respondent 57 (49.1%) performed head and neck stabilization. Most of the respondents secured the head and neck to prevent further worsening of the situation. However, the rest of respondents were afraid due to insufficient knowledge and skill. About equal number of responders removed unwanted object and rest just ignored the object. Interesting reasons for not removing the object, as they were afraid of resulting bleeding. The other respondent did not perform anything as they were concerned about the legal aspect or were frightened of what to do.
It is also clear that more than half of respondent (64.7%) tried to control bleeding and followed by closing the wound (59.5%). The reason was to prevent blood loss and to prevent infection. However, 35.3% did not perform any action to stop bleeding and did not close the wound (40.5%). The consistent reasons were because they did not have sufficient knowledge and skill to stop bleeding and to close the wound.
Table 5 shows that most of respondents (59.5%) check vital sign and even maintain in line position (46.6%) also prevent dangerous movement (70.7%). Moving victim following log roll also was implemented (45.7%) before applying LSB (397%) and referring to appropriate health care.
Distribution of respondent according to referral.
| No | Checking vital sign periodically | Frequency | Percentage (%) |
|---|---|---|---|
| 1 | Yes | 69 | 59.5 |
| 2 | No | 47 | 40.5 |
| Total | 116 | 100 | |
| No | Keeping victims in line position | Frequency | Percentage (%) |
| 1 | Yes | 54 | 46.6 |
| 2 | No | 62 | 53.4 |
| Total | 116 | 100 | |
| No | Prevent any movement | Frequency | Percentage (%) |
| 1 | Yes | 82 | 70.7 |
| 2 | No | 34 | 29.3 |
| Total | 116 | 100 | |
| No | Log roll procedure | Frequency | Percentage (%) |
| 1 | Yes | 53 | 45.7 |
| 2 | No | 63 | 54.3 |
| Total | 116 | 100 | |
| No | Long Spine Board (LSB) application | Frequency | Percentage (%) |
| 1 | Yes | 46 | 39.7 |
| 2 | No | 70 | 60.3 |
| Total | 116 | 100 |
Availability of the first responder in the community is an important concern in order to increase the speed of response to emergency events. The need for appropriate initial assessment and accurate intervention are to minimize disability and improve the chance of survival.8 In term of gender, male would be more dominant in participating as first responder. The finding of this study showed similarity with another study9 which showed that only 4 women (25%) were community respondents and the rest were men. The same trend was also found in previous studies10 where 76% of the respondents were male. Male dominate in almost every activity should also have enough competency, so that they can provide first aid appropriately and quickly to patients with trauma.
One problem often found in the community regarding pre-hospital first aid is the lack competence and knowledge, and the intensity to interact in dealing with patients and the environment in general.11 Educational background, professional background and age can also affect the accuracy in providing first aid. Lay rescuers are no longer perceived to be able to meet the needs of rescuers during many disaster.12 Knowledge is a fundamental factor so that there is awareness for the community to be a helper and at the same time improve their abilities in the first aid midwife. Thus, the resilience of the community in facing disasters can be realized. Mature adults will be more prepared to make decisions and make quick responses compared to immature individuals. However, at an advanced age, the preparedness response in providing relief will tend to slow down.
From various trauma cases in various countries, traffic accidents are still the most frequent cause. The development of transportation modes, population growth on one hand is a factor that accelerates economic turnover but on the other hand has a risk impact on various accidents. The high number of accidents as a cause of head trauma also occurred in previous,2 where traffic accidents were ranked first with 85 accidents (41.7%). This shows that the development of transportation is still in line with the high number of road accidents. The high number of accidents on the road requires fast and precise rescue efforts. Early assessment or initial assessment to help victims determine is necessary for patient safety.10 Responders with appropriate knowledge like doctors, nurses and security officers who have been trained indicated efforts like starting with early assessment by providing pain relief in order to assess consciousness, check pulse and breathing. When vital organs such as the heart, lungs and brain get the right initial treatment will improve chances of patients to survival, avoid the risk of disability and eventually will end for better relief.
Immobilization of victims is an important step to prevent injuries or worsen the condition of the victim. In addition, the patient's condition is expected to be calmer so that the body's metabolism is back to normal. Changes in blood pressure, pulse and respiration are expected to be relatively normal unless extraordinary injuries occur so that it is difficult to overcome. Only half of all respondents in this study made efforts to immobilize patients. In a study10 there were various reasons for not helping the victim. The most dominant reason (81.4%) is not having adequate skills and lack of knowledge about first aid. Some other reasons are fear of creating more danger and less prominent is the fear of being associated with legal aspirations (30%) and various other reasons. Some other respondents stated that they did not provide assistance because they did not know what to do (29.8%), were afraid to cause problems or worsen health conditions (19.6%) and were due to the absence of adequate equipment (7.6%). This shows that education and training for ordinary people about giving first aid to trauma is very important. The impact of this negligence may cause decrease in life expectancy of patients with the possibility of disability after help and a longer treatment process, even it has impact on family members as they bear the burden of the suffering of the victims and the family economy.
The next step after resting the patient is to make sure the functioning of the respiratory system begins by checking whether the airway is functioning properly. The use of a helmet is very important for head safety from various collisions. It also helps to maintain neck stability so that the airway is relatively sustained during an accident. However, if at the time of an accident the patient is still wearing a closed helmet it will make it difficult for the helper to ensure proper ventilation.13 Apart from making it difficult for the examination process it is also difficult for the process of giving breathing assistance. Therefore, if an unconscious patient with head trauma is wearing a closed helmet, it is advisable to immediately release it safely, following right method. The helmet is released to maintain the stability of the neck position. Nearly 75% of respondents in this study did not remove the helmet from the victims because of lack of knowledge and skill to do it properly.
This step must be followed to ensure the safety or patency of the airway and the strength of the ventilation of victims.6 More than the maintenance of ventilation it is important to maintain cerebral perfusion to avoid hypoxemia. In similar studies,10 25.5% performed airway patenting had normal breathing. Vital organs such as the brain and heart have a very poor recovery period from a state of inadequate oxygen. Ischemia of these organs may occur, and rapid fluid resuscitation should be done immediately.
Some respondents in this study according to the limits of their abilities, recognized potential sources of bleeding. Attempts to stop bleeding were also carried out by respondents, by tying simple bandages and splinting on the location of injuries as needed. Respondents with higher educational backgrounds (doctors, nurses and officers) and with proper training, provided help in accordance with the knowledge and skills they already have for example by closing and dressing wounds. Periodically examining the vital status of the patient is one of the important actions taken to monitor the status of the victim. Examination can be done by occasionally calling the victim, checking respiratory status, observing body temperature, blood circulation and so on.
The technique of lifting and removing victims should be done safely. Victims with head trauma especially with a decreased consciousness may have injuries in other parts of the body, especially along the spine to the neck. The application of the log roll technique has been carried out by some of the respondents even though with a simple understanding. Most of the respondents who did not apply this technique were at risk of occurrence of potential new injuries, especially for unconscious victims because of the difficulty in evaluating responses to the relief actions.
Consistent with this data is the use of tools that can function like a long spine board (LSB) to maintain the stability of the victim's position. Less than half of the respondents use LSB or makeshift tools that function to maintain the stability of the victim's body. Respondents like doctors and nurses understand the function and importance of these stabilization aids so that they can help minimize the risk of injury until the victim gets further help. Most respondents do not understand importance of these stabilization aids.
Community as first responder are pivotal to guaranty pre-hospital emergency for any victims experiencing trauma especially head injury cases. Based on the findings of this study, structural training is needed to be scheduled and evaluated periodically to make sure knowledge and skill is adequate. The government, schools and community members need to sit together to discus the need of first responders to develop a plan together. In addition, periodical review is important to adjust new evidence so that the treatment delivered is more accurate and disability along with death can be minimized. However, further studies are needed to explore in relation to education models need, local wisdom, and some matters related to ethical issues.
There are several weaknesses in this research. This study does not provide first aid guidelines for standardized pre-hospital injury. So, stakeholders must develop pre-hospital injury management guidelines for first responder. Moreover, this research does not explore the forum for volunteers who are dedicated in providing first aid for injuries. It is hoped that the results of this study will be a preliminary work to help further study in various developed countries.
Conflict of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Conference on Healthcare and Allied Sciences (2019). Full-text and the content of it is under responsibility of authors of the article.
