




This study aimed at identifying the acceptance of women living with HIV in relation to status disclosure.
MethodThis cross sectional study involved 235 women with HIV positive in Public Health Centre in Jakarta, Indonesia, who were chosen with a consecutive sampling. We used a modified Acceptance of Disease and Impairments Questionnaire (ADIQ) as the instrument.
ResultsThe median score of acceptance was 3 (SD 0.72) in the range of 2.79 to 2.98 at 95% confidence interval. More than half of the respondent (65%) are housewives and 50% of them got infected from their spouses. It was also found that status disclosure was associated with the women acceptance towards HIV (p < 0.05)
ConclusionsThe acceptance of HIV-positive women is influenced by status disclosure which can be positive or negative. This study suggests nurses to consider the grief response of the women with HIV positive to facilitate their acceptance and better adaptation to the illness.
Currently there are 16 million women living with HIV positive or 50% out of the total patient1. Data from the Directorate General of Research and Health Development Ministry of Health of the Republic of Indonesia shows that men are 1.3 times more likely to get infected by HIV than women. However, housewives appear to be the largest part of the woman population infected by HIV, as much as 6539 patients2. Based on the aforementioned data, the spread of HIV to women has been considered to be critical since it has affected housewives and children.
It is hard for women to accept their HIV positive status considering their ability to get pregnant and raise their child. Women affected by HIV from his husband have been showing rage towards God3. They tend to feel anxious towards their baby’s safety4. Women with HIV would likely face multiple losses, such as losing partners, children, family, household, and even environment. This has been considered to be a source of stress for women with HIV to accept their status. A mother has to be in grief of losing her child who died because of AIDS5. They also need to struggle to raise their children after being left by their husbands in the middle of stigma6.
Every woman has experienced the same grief and been influenced by different factors to accept their status. In a chronic disease like HIV positive, the acceptance process is influenced by support from spouse, family, and health staff7,8. However, the acceptance process and specific factors influencing the acceptance of women living with HIV remain unclear. Therefore, this study aimed at identifying the women acceptance, as a phase of sorrow, and its relation to their HIV positive status disclosure.
MethodThis cross sectional study involved 235 women with HIV which were selected with a consecutive sampling method. The instruments used in this study were status disclosure questionnaire and acceptance. We modified the Acceptance of Disease and Impairments Questionnaire (ADIQ)9 to measure acceptance in people living with HIV AIDS and the results is 0.88 for Cronbach’s Alpha and 0.27-0.79 for correlation coefficient. The data were analyzed using linear regression. Ethical approval from The Ethics Committee of Faculty of Nursing Universitas Indonesia was obtained for this study before the data collection started.
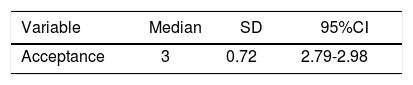
ResultsThe result shows that the median score of acceptance was 3 (SD 0.72) in the range of 2.79 to 2.98 at 95% confidence interval (Table 1). It means women acceptance towards their HIV status has been approaching full acceptance. Most respondents were housewives (65%) married (56%) and half of the respondents were HIV transmitted from their husbands.
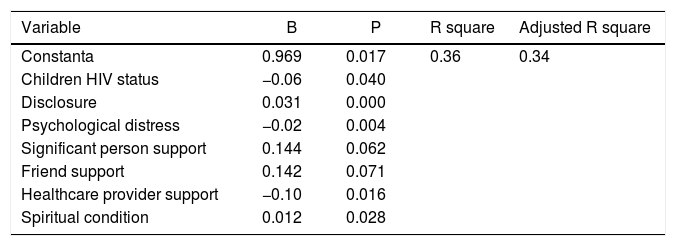
The multivariate analysis linear regression showed that children HIV status, disclosure, psychological distress, significant person support, friend‘s support, healthcare staff support, and spiritual condition were able to predict 34% of acceptance, while the rest was determined by other factors (Tables 2-4).
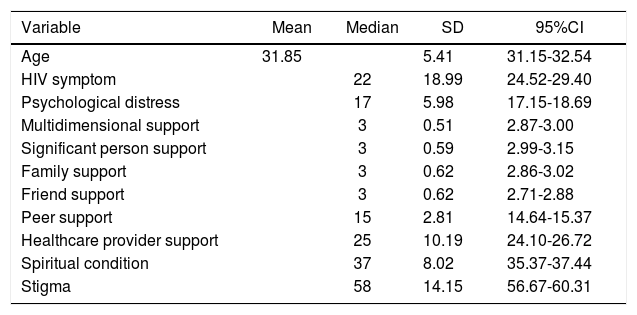
Average and median based on age, HIV symptom, psychological condition, multidimensional support, spiritual condition, and stigma towards women with HIV (n=235).
| Variable | Mean | Median | SD | 95%CI |
|---|---|---|---|---|
| Age | 31.85 | 5.41 | 31.15-32.54 | |
| HIV symptom | 22 | 18.99 | 24.52-29.40 | |
| Psychological distress | 17 | 5.98 | 17.15-18.69 | |
| Multidimensional support | 3 | 0.51 | 2.87-3.00 | |
| Significant person support | 3 | 0.59 | 2.99-3.15 | |
| Family support | 3 | 0.62 | 2.86-3.02 | |
| Friend support | 3 | 0.62 | 2.71-2.88 | |
| Peer support | 15 | 2.81 | 14.64-15.37 | |
| Healthcare provider support | 25 | 10.19 | 24.10-26.72 | |
| Spiritual condition | 37 | 8.02 | 35.37-37.44 | |
| Stigma | 58 | 14.15 | 56.67-60.31 |
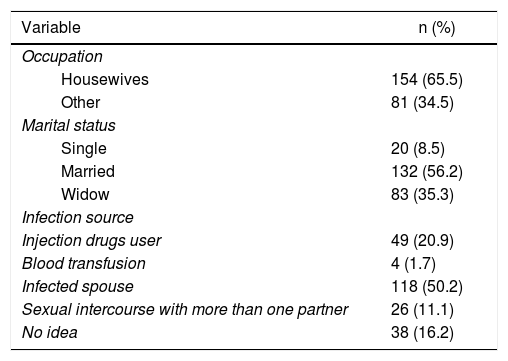
Frequency distribution based on occupation, marital status, and infection source of women with HIV (n=235).
| Variable | n (%) |
|---|---|
| Occupation | |
| Housewives | 154 (65.5) |
| Other | 81 (34.5) |
| Marital status | |
| Single | 20 (8.5) |
| Married | 132 (56.2) |
| Widow | 83 (35.3) |
| Infection source | |
| Injection drugs user | 49 (20.9) |
| Blood transfusion | 4 (1.7) |
| Infected spouse | 118 (50.2) |
| Sexual intercourse with more than one partner | 26 (11.1) |
| No idea | 38 (16.2) |
Acceptance model of women living with HIV.
| Variable | B | P | R square | Adjusted R square |
|---|---|---|---|---|
| Constanta | 0.969 | 0.017 | 0.36 | 0.34 |
| Children HIV status | −0.06 | 0.040 | ||
| Disclosure | 0.031 | 0.000 | ||
| Psychological distress | −0.02 | 0.004 | ||
| Significant person support | 0.144 | 0.062 | ||
| Friend support | 0.142 | 0.071 | ||
| Healthcare provider support | −0.10 | 0.016 | ||
| Spiritual condition | 0.012 | 0.028 |
The average of respondents’ age is 32 years old, which is a reproductive age. Meanwhile a data showed that in Indonesia AIDS is more likely to infect people in their 20-29 years old2. Furthermore, the study also revealed that the most infected respondents were housewives. Previous studies showed that the group with the highest probability to be infected by HIV (59.7%) is married and having HIV infected sexual partners10. These show that most women living with HIV are in their reproductive age and infected by their partners or spouses. Women living with HIV, especially those in their productive age, tend to transmit the disease to their children. This fact will likely bring loss and grief to women. However, this study shows that most respondent are in their full acceptance. This is a result of acquired value that being infected by HIV is a destiny3 and a fact of past experience that cannot be repeated. The future of the children is also a consideration for women to accept their condition. This is due to women’s role that they are not only individuals but also mothers who have to raise and take care of their kids5. Social support from the healthcare provider and closest relatives are also factors supporting women to accept their status. This can be seen from the correlation between social support and acceptance in this study. Previous study reported that women living with HIV in India received double burden by taking care of their sick husbands and children, getting the stigma, and experiencing financial difficulties. Nevertheless, they were able to cope with all the condition effectively with the social and religious supports11.
Close relationship between women living with HIV and the healthcare provider will also increase patients’ efficacy and improve their obedience in taking medication8. Medication, information, and counseling received by the patients will motivate them and give them hope to continue their live and have healthy children. Women living with HIV and have good selfefficacy will be able to continue their daily life and consume medicines regularly12. Such condition will be able to improve body immune and life quality of the patient. This can be seen from the fact that these respondent are mostly in good condition, because all of the respondent are patients who get healthcare treatment in each respective healthcare provider.
The result of this study also shows the disclosure status that influenced the acceptance. This reveals that the more the women tend to disclose their HIV status, the higher of their acceptance will be. The preceding studies found out that the status disclosure was a sensitive issue for the people living with HIV. They thought that disclosing their status as people living with HIV is more frightening than the disease itself13. However, some of them prefer to disclose their status in order to gain supports and to prevent others to get infected. Referring to the findings of this study, women with HIV-positive tend to be cautious to close their HIV status because of fear from stigma of HIV will attack them and their children. The majority of respondents in this study only tell their spouse, some have been able to tell their parents because they need emotional support when they or their children have seriously ill related to HIV.
The result of this study is in line with the prior studies that stated the women tend to easily disclose their HIV status to their partners so that their partners will not get affected14. This status disclosure leads to the possibility to obtain psychological support15. The acceptance from their family member, moreover, is the most important thing to the HIV patient in living their life and in taking their treatment16. Almost all respondents complied with the treatment because they always reminder by their families for treatment regularly. Most respondents in this study has been able to live healthily and regularly taking the drugs either with the help of alarm cell phone or frequently reminded by their husbands or their parents. All respondents expressed that support from her husband and family is very important for them to constantly remind and motivate them for better life. This is in accordance with the Indonesian culture that still holds family values to maintain and care for sick family members.
The majority of the women who were the subjects of this study have disclosed their status to their husband and parents. This shows the same result as the previous studies that revealed the positive impact to the women with HIV that disclosed her status to her mother17. This is considered as a maternal bond between the mother with her daughter which lead to the acceptance and support given by the mother. These may help the HIV patients to accept their status particularly for women with HIV. This will help them to live their live rather than to keep their status to themselves18.
The earlier studies also revealed that the HIV status disclosure to the other people living with HIV will also give encouragement to each other19. Social support from their colleagues will also encourage them to take their medicine regularly. Moreover, the support may also help the patients to have a more constructive attitude than those who do not have any support from their colleagues and health department8,12. The subjects of this study have received health service and obtained social support particularly in information and psychological support.
This study was funded by Direktorat Penelitian dan Pengabdian Masyarakat of Universitas Indonesia. We would like to thank to Ikatan Perempuan Positif Indonesia, Kotex Foundation, Health Division of Jakarta, Tegak Tegar Foundation for their help in data collection. Thanks go to Ariesta Milanti and team in Maternal and Women’s Health Departemen, Nursing Faculty Universitas Indonesia for their grateful support.
Conflicts of interestNone declared.
