



To identify the relationship of unmet supportive care needs with quality of life of patients with gynecological cancer undergoing therapy.
MethodThis study used a cross-sectional design. A total of 153 patients with gynecological cancer undergoing therapy were recruited using consecutive sampling methods. The participants completed the questionnaire of Supportive Care Needs Survey to identify their supportive care needs, EORTC-QLQ 30 to assess their general quality of life, and EORTC-QLQ-CX 24 or - OV 28 to determine cancer-specific quality of life in cervical cancer and ovarian cancer, respectively.
ResultsMost of the participants (96.1%) reported their unmet needs of supportive care predominantly in the physical domain (80.4%). Unmet supportive care needs were found to be statistically significantly related to quality of life in the global health, functional, and symptom domains (p value 1=0.003, p value 2=<0.001, and p value 3= 0.001; r1=-0.235, r2=0.306, and r3=0.268, respectively).
ConclusionsPatients with gynecological cancer needs various supportive care during treatment. These supportive care needs should be identified early at the time of diagnosis and continued throughout the disease and treatment trajectory to the survivorship point. Otherwise, unmet supportive care needs may lead to a low quality of life.
Gynecological cancer remains one of the most prevalent cancers in women. According to the data released by Globocan in 2012, cervical cancer and ovarian cancer are the two gynecological cancers with the highest occurrence in Indonesia. The incidence rates of cervical cancer and ovarian cancer are 17.3 and 8.4, respectively, among 100,000 women per year1.
The effects of cancer pathology and its treatments are so poignant and multidimensional that supportive care is highly needed. For example, impaired physical function is usually associated with symptoms of distress, both of which may bring issues on daily activities and eventually result in unmet supportive care needs2. This seemingly vicious cycle should be anticipated by the early identification of supportive care needs in cancer patients, so that the quality of life (QOL) of cancer patients would be improved.
Supportive care needs refer to the management of cancer symptoms and side effects, empowering of patients’ adaptability and coping, optimization of understanding and information on decision making, and minimizing of body deficiencies3. Supportive care needs are broad in dimension, ranging from physical to sexual4.
QOL is an important goal in the treatment of cancer. Concerns about the physical, psychological, body image disturbance, and symptoms that can cause distress should be anticipated to improve the QOL of cancer patients. A previous study in Indonesia found that the QOL of cancer patients decreased after chemotherapy5. Improving the QOL of cancer patients during treatment improves their adherence to cancer care and treatment and strengthens their ability to overcome cancer-related symptoms or complaints6.
To reach the QOL at its most favorable level, strong supportive care service is the key2,6. Quality nursing care should meet this aim not only to address the accompanying symptoms of cancer and its treatments but also to increase patient satisfaction.
The identification of supportive care support for cancer patients undergoing chemotherapy remains an uncommon practice in Indonesia. Supportive care service mostly addresses cancer survivors and overlooks those currently suffering from cancer7,8. To encourage action in providing supportive care for gynecological cancer patients during therapy, more solid evidence is needed to examine how supportive care needs relates to the QOL of gynecological cancer patients undergoing therapy, thus explaining the objective of this study. In this article, we present a part of a large study with emphasis on the association between supportive care needs and QOL.
MethodThis work was a cross-sectional correlation study. The sample comprised 153 patients with cervical cancer and ovarian cancer undergoing treatment at two central hospitals in Jakarta, Indonesia, from May to June 2016. The respondents were selected through the consecutive sampling method. The number of the sample was calculated using the cross-sectional sample size formula9, with the standard deviation taken from a prior relevant study10.
We used Supportive Care Needs Survey (SCNS-SF34) to measure the need for supportive services. This questionnaire consists of 34 question items under five domains: physical, psychological, supportive care, health system and information, and sexuality11. This tool had a validity score of 0.302-0.792 and a reliability score of 0.933. The QOL was measured using the European Organization of Research and Treatment of Cancer Quality of Life Q-C30 (EORTC QLQ-30), Quality of Life Questionnaire Module Cervical Cancer (EORTC QLQ-CX 24), and Quality of Life Questionnaire ovary Cancer Module (EORTC QLQ-OV28). These instruments underwent forward translation from English to Bahasa Indonesia by an academic language center and an expert panel review. All questionnaires were piloted for validity and reliability testing among 30 respondents in a different setting.
Ethical approval was granted by the Institutional Review Board of Faculty of Nursing, Universitas Indonesia, and Dharmais Cancer Hospital. We adhered to ethical principles, including the right to self-determination, anonymity and confidentiality, and protection from discomfort and harm.
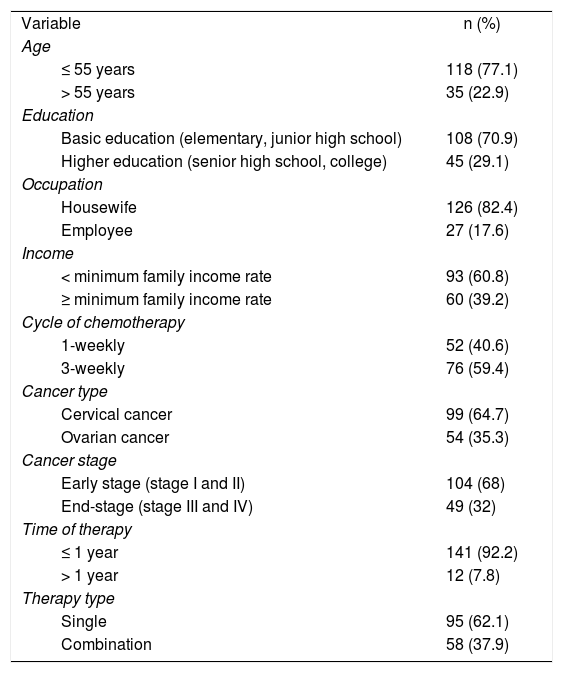
ResultsThe demographic characteristics of the respondents are presented in Table 1. The table shows that most respondents were 55 years and below, worked as housewives, and were of a low socioeconomic status, as shown in their family income rate. More than half of the respondents were diagnosed with stages I and II cervical cancer, with less than a year of cancer treatment.
Characteristics of the respondents (n=153).
| Variable | n (%) |
| Age | |
| ≤ 55 years | 118 (77.1) |
| > 55 years | 35 (22.9) |
| Education | |
| Basic education (elementary, junior high school) | 108 (70.9) |
| Higher education (senior high school, college) | 45 (29.1) |
| Occupation | |
| Housewife | 126 (82.4) |
| Employee | 27 (17.6) |
| Income | |
| < minimum family income rate | 93 (60.8) |
| ≥ minimum family income rate | 60 (39.2) |
| Cycle of chemotherapy | |
| 1-weekly | 52 (40.6) |
| 3-weekly | 76 (59.4) |
| Cancer type | |
| Cervical cancer | 99 (64.7) |
| Ovarian cancer | 54 (35.3) |
| Cancer stage | |
| Early stage (stage I and II) | 104 (68) |
| End-stage (stage III and IV) | 49 (32) |
| Time of therapy | |
| ≤ 1 year | 141 (92.2) |
| > 1 year | 12 (7.8) |
| Therapy type | |
| Single | 95 (62.1) |
| Combination | 58 (37.9) |
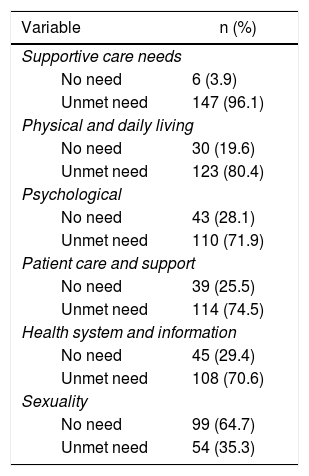
The unmet supportive care needs of the respondents are summarized in Table 2. The highest unmet need was identified as the physical domain (80.4%) and the lowest was sexuality.
Unmet supportive care needs (n=153).
| Variable | n (%) |
|---|---|
| Supportive care needs | |
| No need | 6 (3.9) |
| Unmet need | 147 (96.1) |
| Physical and daily living | |
| No need | 30 (19.6) |
| Unmet need | 123 (80.4) |
| Psychological | |
| No need | 43 (28.1) |
| Unmet need | 110 (71.9) |
| Patient care and support | |
| No need | 39 (25.5) |
| Unmet need | 114 (74.5) |
| Health system and information | |
| No need | 45 (29.4) |
| Unmet need | 108 (70.6) |
| Sexuality | |
| No need | 99 (64.7) |
| Unmet need | 54 (35.3) |
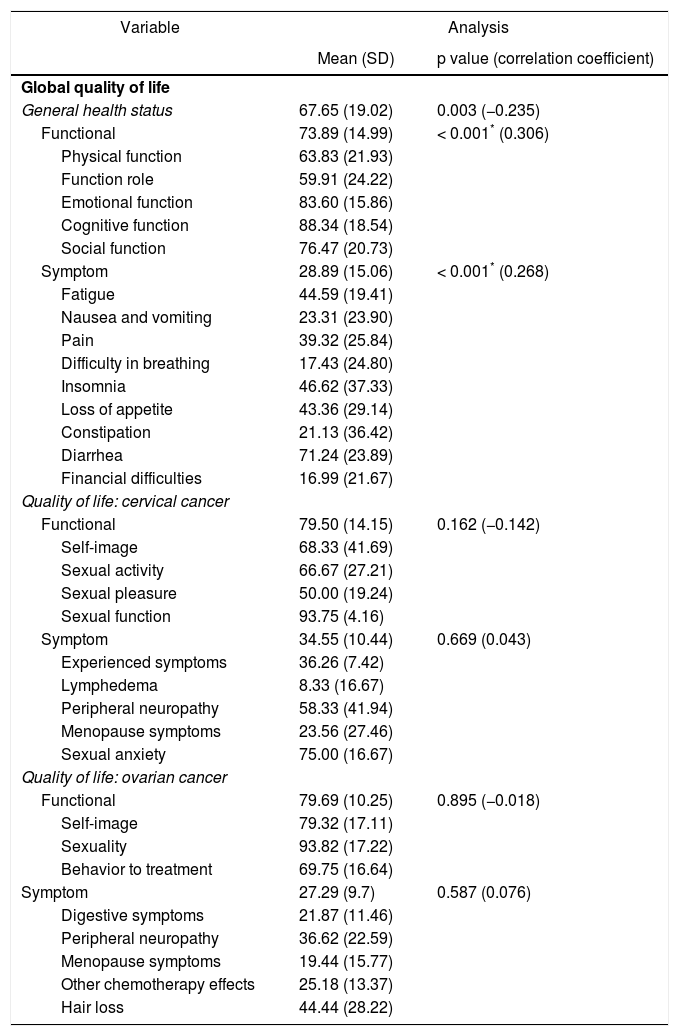
Table 3 presents the bivariate analysis that determines the relationship between the need for supportive services and the QOL of gynecological cancer patients undergoing therapy.
Relationship between the need for supportive services and quality of life (n=153).
| Variable | Analysis | |
|---|---|---|
| Mean (SD) | p value (correlation coefficient) | |
| Global quality of life | ||
| General health status | 67.65 (19.02) | 0.003 (−0.235) |
| Functional | 73.89 (14.99) | < 0.001* (0.306) |
| Physical function | 63.83 (21.93) | |
| Function role | 59.91 (24.22) | |
| Emotional function | 83.60 (15.86) | |
| Cognitive function | 88.34 (18.54) | |
| Social function | 76.47 (20.73) | |
| Symptom | 28.89 (15.06) | < 0.001* (0.268) |
| Fatigue | 44.59 (19.41) | |
| Nausea and vomiting | 23.31 (23.90) | |
| Pain | 39.32 (25.84) | |
| Difficulty in breathing | 17.43 (24.80) | |
| Insomnia | 46.62 (37.33) | |
| Loss of appetite | 43.36 (29.14) | |
| Constipation | 21.13 (36.42) | |
| Diarrhea | 71.24 (23.89) | |
| Financial difficulties | 16.99 (21.67) | |
| Quality of life: cervical cancer | ||
| Functional | 79.50 (14.15) | 0.162 (−0.142) |
| Self-image | 68.33 (41.69) | |
| Sexual activity | 66.67 (27.21) | |
| Sexual pleasure | 50.00 (19.24) | |
| Sexual function | 93.75 (4.16) | |
| Symptom | 34.55 (10.44) | 0.669 (0.043) |
| Experienced symptoms | 36.26 (7.42) | |
| Lymphedema | 8.33 (16.67) | |
| Peripheral neuropathy | 58.33 (41.94) | |
| Menopause symptoms | 23.56 (27.46) | |
| Sexual anxiety | 75.00 (16.67) | |
| Quality of life: ovarian cancer | ||
| Functional | 79.69 (10.25) | 0.895 (−0.018) |
| Self-image | 79.32 (17.11) | |
| Sexuality | 93.82 (17.22) | |
| Behavior to treatment | 69.75 (16.64) | |
| Symptom | 27.29 (9.7) | 0.587 (0.076) |
| Digestive symptoms | 21.87 (11.46) | |
| Peripheral neuropathy | 36.62 (22.59) | |
| Menopause symptoms | 19.44 (15.77) | |
| Other chemotherapy effects | 25.18 (13.37) | |
| Hair loss | 44.44 (28.22) | |
SD, standard deviation.
The results of this study indicate a relationship between unmet supportive care needs and the global QOL in the domains of global health, functional, and symptoms in patients with gynecological cancer undergoing chemotherapy. Conversely, no significant association was found when the QOL was measured specifically against cervical cancer and ovarian cancer QOL. A consistent result was reported by a previous study assessing a similar hypothesis in a different cancer population12. The present study affirms the previous finding that patients with more unmet supportive care needs are more likely to have lower QOL.
The QOL of cervical cancer patients is affected by general health status and good relationships between the patients and healthcare professionals13. Cervical cancer patients receiving chemotherapy may experience a number of side effects, such as pain, fatigue, nausea, vomiting, and poor appetite, and they affect the QOL of these patients14. Poor management of the treatment's side effects and inadequate self-care negatively affect the QOL of patients6,15. Increasing the QOL of cancer patients during therapy increases patient compliance with the treatment and contributes to their self-efficacy6.
Similar to patients with cervical cancer, ovarian cancer patients also struggle with their interrelated physical and emotional changes, such as anxiety or depression, which may deteriorate their QOL. Simultaneous interactions worsen the existing symptoms and lead to other symptoms16.
In this study, unmet supportive care needs in the physical domain were found to be strongly related to the QOL of the patients. This finding is consistent with that of Effendy et al7, who found that physical problems constituted the most dominant unmet need in Indonesian patients with advanced cancer. An earlier study among Chinese patients also showed a similar result17. The physical symptoms commonly experienced by cancer patients undergoing therapy include decreased appetite, change in the taste of food, hair loss, nausea, vomiting, and fatigue18. Patients need support to cope with these physical symptoms to improve their condition and QOL.
Psychological health status also contributes to the QOL of patients undergoing treatment for cervical cancer19. In their study on supportive care needs, psychosocial status, and QOL of survivors of gynecological cancers, Hodgkinson et al. found that psychological distress is a predictor of unmet supportive care needs and low QOL20. Therefore, cancer patients undergoing therapy need emotional support to cope with their anxiety, sadness, and fear during the process of diagnosis and treatment21. Patients need reassurance and motivation to remain optimistic throughout their cancer experience18.
Conflicts of interestNone declared.
This study was funded by the Directorate of the Research and Community Service, Universitas Indonesia.
