





Anxiety is the most common response to myocardial infarction (MI). The objective of the study is to compare the effect of eye movement desensitization reprocessing (EMDR) and cognitive behavioral therapy (CBT) on anxiety in patients with myocardial infarction.
MethodsIn this clinical trial, 90 eligible patients suffering from MI were selected using the convenience sampling method and randomly assigned to two intervention groups and one control group. The first intervention group attended eight 1-h EMDR sessions in a tranquil environment in a hospital. The second intervention group attended ten 90-min CBT sessions under an identical condition. The control group, on which no intervention was made, merely received prescribed medication by a physician (Oxazepam 10mg) at 10:00 P.M. on a nightly basis. The mean anxiety was measured for all three groups before and after intervention through the Beck Anxiety Inventory (BAI). Data were analyzed using SPSS v.20, and such statistical tests and the chi-squared, analysis of variance (ANOVA), and Tukey's Honestly Significant Difference (HSD) post hoc test. P values are significant at P<0.05.
ResultsResults pointed to a significant statistical difference between the intervention and control groups in terms of the mean anxiety score differences (P<0.001).
ConclusionBoth EMDR and CBT reduced anxiety levels in patients with MI, with the former being the more effective one.
Coronary heart diseases are conditions that occur by the hardening of coronary arteries, i.e. atherosclerosis,1 one of which is MI, which is the leading cause of death in developed countries and Iran.2 Anxiety is the most common response to MI, with a prevalence rate of about 70–80% in patients suffering from acute coronary syndrome.3 It negatively impacts post-MI recovery such that patients who demonstrate anxiety during the first 48h after MI are about 5 times more prone to complications of recurrent MIs, ischemic relapses, ventricular fibrillations and ventricular tachycardia.4 On account of the negative impacts of anxiety on cardiovascular patients, it is vital for physicians and nurses to, first, precisely identify patients with anxiety and, then, take effective control and therapeutic measures.5
Cognitive behavioral techniques are among anxiety treatment methods in cardiovascular patients, one of which is the eye movement desensitization reprocessing (EMDR) method. It is a modern safe method without negative side-effects which does not rely on speech- or pharmaceutical therapy and is rather based on the rapid regular movements of the patient's eyes.2 Gradual EMDR is more effective than pharmaceutical therapy in treating anxiety disorders; although a number of studies point to contradictory results.6 EMDR is inexpensive compared to other methods and has been proven to have long-lasting effects without needing much time to achieve favorable results. EMDR is a psychotherapeutic technique that has been very successful in helping those suffering greatly from trauma, anxiety, fear, painful memories, post-traumatic stress, and other emotional problems.7
Cognitive behavioral therapy (CBT) is another method of anxiety treatment in which the patient is encouraged to regard the relation between his/her negative thoughts and feeling of anxiety as hypotheses that need to be tested and use behaviors induced from negative thoughts as criteria to determine their validity.8
Given the previous studies suggesting a high prevalence rate of anxiety among cardiovascular patients and on account of its adverse effects on all systems of the human body, in particular the cardiovascular system, which can cause life-threatening dysrhythmia, heart attack, and sudden cardiac arrest, it is incumbent upon all medical staff to pay attention to effective methods of treating anxiety. Therefore, the present study was conducted to compare the effect of EMDR and CBT on anxiety levels.
MethodsThe present clinical trial was done on 90 myocardial infarcted patients admitted to Imam Sajjad Hospital of Yasuj, Iran, who were eligible to be included in the study. Sampling was done after the necessary license was obtained from Yasuj University of Medical Sciences’ Ethics Committee (ethics code: ir.yums.rec.1395, 26) and registered in the Iranian Registry of Clinical Trials (registry number: IRCT2016052428017N2). Participants were selected through the convenience sampling method and assigned to two intervention groups and one control group using the randomized block design. The objectives of the study as well as the number of sessions were first explained to participants. Next, they completed the informed consent forms, the demographic information questionnaire as well as the BAI. The above instruments were administered to all three groups before intervention. Then, the EMDR group attended eight 45–90-min sessions, twice a week, in a quiet room in the hospital according to the existing protocol. The other intervention group also attended ten 90-min CBT sessions, twice a week, and their anxiety-related data were scored before and after intervention. The anxiety levels of the third, i.e. control, group were measured during the first and last sessions. They merely received prescribed medication by the physician (Oxazepam 10mg) at 10:00 P.M. on a nightly basis, with no additional intervention made by the researcher.
The inclusion criteria consisted of: 1 – MI diagnosed by a cardiologist, 2 – patients who have suffered MI for more than one occasion and who have prevailed over the acute stage of the disease, 3 – patients with no history of extensive MIs, 4 – patients with stable hemodynamic status, 5 – patients with no history of seizures, 6 – patients with no history of mental disorders, 7 – patients not suffering from drug addiction, 8 – being under 60 years of age, and 9 – patients without strabismus and/or vision problems.
The exclusion criteria were: 1 – patients who could not endure the EMDR method, and 2 – lack of cooperation with the therapist.
The instruments were twofold: 1 – background (demographic) information questionnaire including information about age, sex, education, smoking history, and marital status which was developed by the researcher, and 2 – the BAI,9 a self-report 21-item inventory designed to measure the severity of physical and cognitive symptoms of anxiety in patients during the past week. There are four answers to each item on a scale value of 0–3 indicating an incremental increase in the severity of anxiety. This inventory is predominantly focused on the physiological symptoms of anxiety. Three items are related anxious mood, three to specific panics, and other items measure symptoms of autonomic hyperactivity and motor tension. Answers are scored from 0 to 3 as such: not at all (0), mildly (1), moderately (2), and severely (3). Consequently, the score range is from 0 to 63. A score of 0–21 demonstrates minimal anxiety, 22–35 moderate anxiety, and higher than 36 severe anxiety. Beck et al. reported a 92% internal consistency, a 75% test–retest reliability (1 week), and 30–76% of inter-item correlation for this inventory. In a study conducted in Roozbeh Hospital, Tehran University of Medical Sciences, the internal consistency of the Inventory was reported as 90% (Cronbach's alpha=0.90).10 Data were analyzed using SPSS v.20, descriptive statistics, Fisher's exact test, t-test, paired t-test, analysis of variance (ANOVA) and Tukey's HSD post hoc test.
ResultsPatients fell in the 33–60 years age range. The mean age of patients was 47.62+/−8.93. In terms of gender, 72.22% (65) of patients were male and the rest, i.e. 27.77% (25) were female. In terms of marital status, 91.02% (82) were married and 8.88%8 were single. In terms of education, 57.77% (52) had high school diplomas or lower degrees, 29.97% (27) had bachelor's and 12.21%11 had master's degrees. Results revealed that 60% (54) of patients had no history of smoking, with only 40% (36) were smokers. Using the ANOVA test, it was shown that there was no statistically significant difference among the three groups.
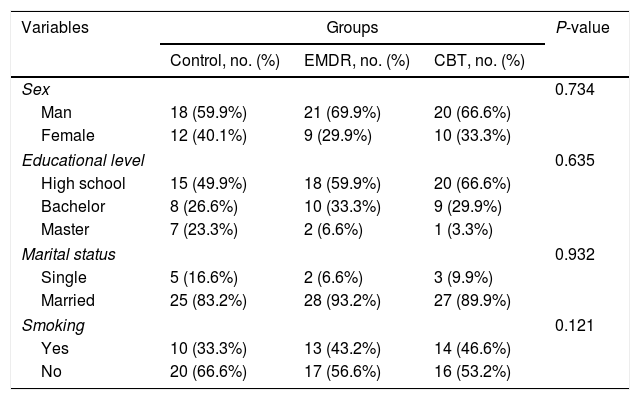
Results from the chi-squared and ANOVA tests demonstrated that the three groups exhibited homogeneity with no statistically significant difference seen in terms of demographic characteristics such as sex, education, marital status, and history of smoking (P>0.05) (Table 1).
Demographic characteristics of the studied patients (N=90)a
| Variables | Groups | P-value | ||
|---|---|---|---|---|
| Control, no. (%) | EMDR, no. (%) | CBT, no. (%) | ||
| Sex | 0.734 | |||
| Man | 18 (59.9%) | 21 (69.9%) | 20 (66.6%) | |
| Female | 12 (40.1%) | 9 (29.9%) | 10 (33.3%) | |
| Educational level | 0.635 | |||
| High school | 15 (49.9%) | 18 (59.9%) | 20 (66.6%) | |
| Bachelor | 8 (26.6%) | 10 (33.3%) | 9 (29.9%) | |
| Master | 7 (23.3%) | 2 (6.6%) | 1 (3.3%) | |
| Marital status | 0.932 | |||
| Single | 5 (16.6%) | 2 (6.6%) | 3 (9.9%) | |
| Married | 25 (83.2%) | 28 (93.2%) | 27 (89.9%) | |
| Smoking | 0.121 | |||
| Yes | 10 (33.3%) | 13 (43.2%) | 14 (46.6%) | |
| No | 20 (66.6%) | 17 (56.6%) | 16 (53.2%) | |
Abbreviations: EMDR: eye movement desensitization reprocessing; CBT: cognitive behavioral therapy.
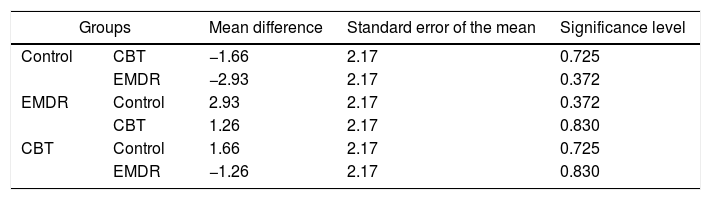
Based on the Kolmogorov–Smirnov Test, all variables were normally distributed. Results from ANOVA, Tukey's HSD post hoc test, and Fisher's Least Significant Difference (LSD) pointed to no statistically significant difference in mean anxiety scores before intervention in all three groups (P>0.05).
Results from ANOVA and Tukey's HSD post hoc tests showed no statistically significant difference in mean anxiety scores before intervention in all three groups (P>0.05) (Table 2). Data analysis using the Tukey's HSD post hoc test demonstrated a significant difference in mean anxiety scores between the control and EMDR groups after intervention (P<0.001) (Table 3). In addition, results showed a significant difference in mean anxiety scores between the control and CBT groups after intervention (P<0.001) and also between EMDR and CBT groups (P<0.001) (Table 3).
Comparison of mean anxiety differences in all three groups before intervention.
| Groups | Mean difference | Standard error of the mean | Significance level | |
|---|---|---|---|---|
| Control | CBT | −1.66 | 2.17 | 0.725 |
| EMDR | −2.93 | 2.17 | 0.372 | |
| EMDR | Control | 2.93 | 2.17 | 0.372 |
| CBT | 1.26 | 2.17 | 0.830 | |
| CBT | Control | 1.66 | 2.17 | 0.725 |
| EMDR | −1.26 | 2.17 | 0.830 | |
Abbreviations: EMDR: eye movement desensitization reprocessing; CBT: cognitive behavioral therapy.
Comparison of mean anxiety differences in all three groups after intervention.
| Groups | Mean difference | Standard error of the mean | Significance level | |
|---|---|---|---|---|
| Control | CBT | −13.16 | 2.14 | 0.001 |
| EMDR | −9.13 | 2.14 | 0.001 | |
| EMDR | Control | 9.13 | 2.14 | 0.001 |
| CBT | 5.39 | 2.14 | 0.001 | |
| CBT | Control | 13.16 | 2.14 | 0.001 |
| EMDR | −5.39 | 2.14 | 0.001 | |
Abbreviations: EMDR: eye movement desensitization reprocessing; CBT: cognitive behavioral therapy.
The comparison of mean anxiety differences in the three groups after intervention using ANOVA showed a statistically significant difference (P<0.001). Results from ANOVA and Tukey's HSD post hoc tests revealed a statistically significant difference in terms of mean difference of anxiety variables between the control, EMDR, and CBT groups (P<0.001). On the other hand, comparison of the effect of EMDR and CBT on the mean anxiety showed that EMDR reduced the mean anxiety to a greater extent compared with CBT (P<0.001), meaning that it was a more effective intervention (Table 4).
Paired comparison of pre-intervention mean anxiety scores in all three groups.
| Groups | Mean anxiety difference | Significance level |
|---|---|---|
| EMDR and CBT | 5.39 | 0.001 |
| CBT and control | 13.16 | 0.001 |
| EMDR and control | 9.13 | 0.001 |
Abbreviations: EMDR: eye movement desensitization reprocessing; CBT: cognitive behavioral therapy.
The present study was conducted to compare the effect of EMDR and CBT on myocardial infarcted patients’ anxiety levels admitted to incentive care units of Imam Sajjad Hospital of Yasuj, Iran. An important finding was that EMDR and CBT were both effective in reducing anxiety in such patients, with the former being more effective than the latter. Results from a review article by Shapiro (2014) revealed that EMDR had positive effects in treating emotional traumas and other negative life experiences in 24 clinical trials. Results from 7 of such studies demonstrated that EMDR led to quicker and more effective results than CBT in helping patients cope with negative experiences and emotions,11 which corresponds to and confirms the results of the present study.
Capezzani et al. (2013) conducted a comparative study titled “the effect of EMDR and CBT on the anxiety and depression levels in patients suffering from cancer”. Results revealed that both methods reduced anxiety and depression in such patients which corresponds to and confirms the results of the present study.12
In the study by Roy et al. (2005), the effect of CBT coupled with pharmaceutical therapy on anxiety disorders was compared with mere pharmaceutical therapy on 232 patients divided into two groups. Results demonstrated that the mixed treatment (CBT plus pharmaceutical therapy) significantly reduced anxiety symptoms in such patients and improved their performance and quality of life. However, the other group who had merely received medication showed little improvement.13 In another study by Yousefy et al. cognitive-behavioral therapy in the case group led to reduced anxiety and improved quality of life in patients with heart disease.14
Narimani et al. (2009) conducted a study titled “comparison of EMDR and CBT in treating post-traumatic stress disorder (PTSD)” in Ardabil, Iran. Fifty-one veterans with PTSD were selected using the simple random sampling method and assigned randomly to three groups, i.e. EMDR, CBT, and control. Results pointed to a statistically significant difference in terms of pre- and post-test mean score differences, and Hospital Anxiety and Depression Scale (HADS) among the three groups (P=0.001).15 Liuva et al. showed that EMDR and CBT were equally effective on treatment of anxiety and depression.12
Results from the study by Arabia et al. (2011) revealed that EMDR resulted in a greater reduction of anxiety and depression in patients who had suffered from life-threatening cardiac events compared with the visual exposure method,16 which corresponds to the findings of this study.
Ashaieri et al. compared EMDR, pharmaceutical therapy and cognitive therapy in reducing anxiety symptoms in students. Results from the analysis of covariance (ANCOVA) showed that all three methods reduced anxiety symptoms, with EMDR and cognitive therapy being more effective than pharmaceutical therapy.17
To account for the collective findings of this study, it can be argued that EMDR accelerates and organizes the information processing system, maintains its dynamism, and abandons peripheral information related to the event. Such delayed learning is made possible by the association of the traumatic memory in question with neurophysiological networks, which retains more favorable information. When adaptive reprocessing occurs as a result of EMDR, traumatic events are desensitized and cognitively reconstructed in an adaptive manner. Therefore, after successful EMDR therapy, irksome memories are so altered that have little emotional power to cause unrest or discomfort. The quick, positive effect of EMDR is a testament to the idea that, using this method, information takes an adaptive form.
Results from the present study revealed that EMDR and CBT were both effective in reducing anxiety in myocardial infarcted patients, with the former being the more effective one.
Ethical considerationThe necessary license was obtained from Yasuj University of Medical Sciences’ Ethics Committee (ethics code: ir.yums.rec.1395, 26) and registered in the Iranian Registry of Clinical Trials (registry number: IRCT2016052428017N2).
Funding/SupportWe received a grant from the Deputy of Research and Technology of Yasuj University of Medical Sciences, Iran.
Conflict of interestNone declared.
The authors appreciate the Research Deputy of Yasuj University of Medical Sciences because of their support, and also thank the nurses of Heart and Vessel Yasuj Hospital who had extended friendly cooperation in all the procedures of this study. Also the authors thank to all patients and Francine Shapiro for the assistance provided with the research.