





Casos Clínicos en Gastroenterología y Hepatología
Más datosSEMS are a palliative alternative for dysphagia secondary to extrinsic compression, in order to allow nutritional intake and to improve the patients’ quality of life. The most frequent causes of esophageal extrinsic compression share a malignant etiology.1
We present the case of a 61-year-old female patient diagnosed stage IV lung adenocarcinoma in April 2020. Chemotherapy and immunotherapy were initiated. In May the patient started with dysphagia secondary to extrinsic compression from mediastinal adenopathies visualized.
A palliative esophageal stent placement was requested. Upper endoscopy was performed. Stenosis secondary to extrinsic compression was observed 20cm from the incisors. With the aid of fluoroscopy, a SEMS (Wallflex-Esophageal 18mm×103mm) was correctly placed distal to the upper esophageal sphincter. No intraprocedural complications were notified and the patient was discharged 24h post-procedure asymptomatic.
One day later, the patient was admitted referring sudden dyspnea, stridor, dysphonia and oxygen desaturation. Chest-X-rays were performed, identifying the stent correctly positioned and without any apparent complications (migration or perforation). Laryngoscopy revealed bilateral vocal cord paralysis (BVCP). Urgent tracheostomy was performed and intravenous corticosteroids were administered. However, BVCP persisted on the control fibrolaryngoscopy. Withdrawal was requested. It was easily removed five days later with a foreign body forceps. Another fibrolaryngoscopy was performed revealing a moderate improvement in vocal cord movement. Nevertheless, three weeks later the patient died of persistent respiratory insufficiency.
Correct placement of esophageal SEMS is achieved with a success rate of almost 100%. Proximal strictures may be more challenging, but still, several alternatives are available, as for example using narrow-diameter SEMS or even placing biliary SEMS.2 However, severe complications may develop, mainly recurrence of dysphagia, aspiration pneumonia, hemorrhage, fistulas, perforation or migration.3
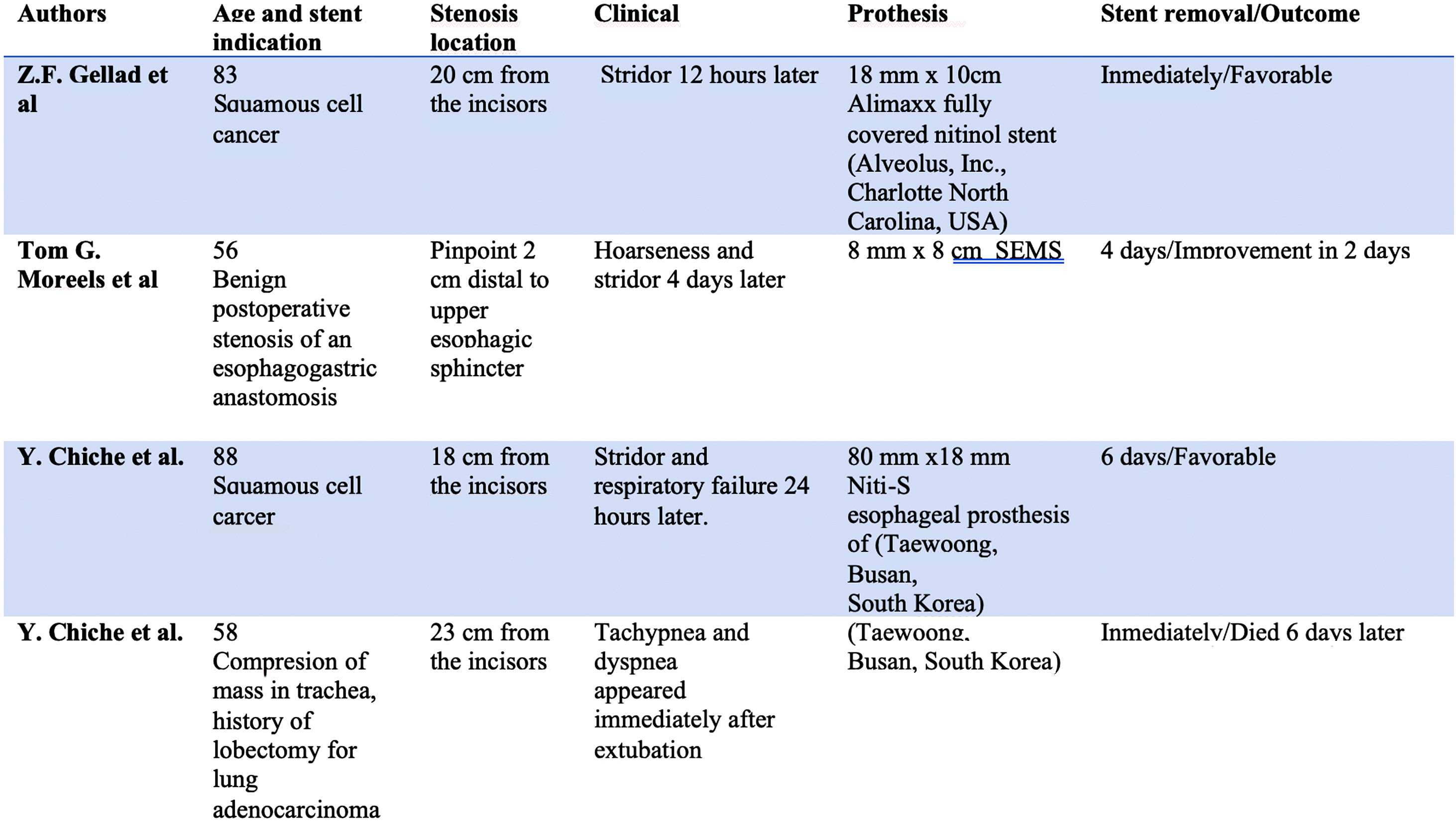
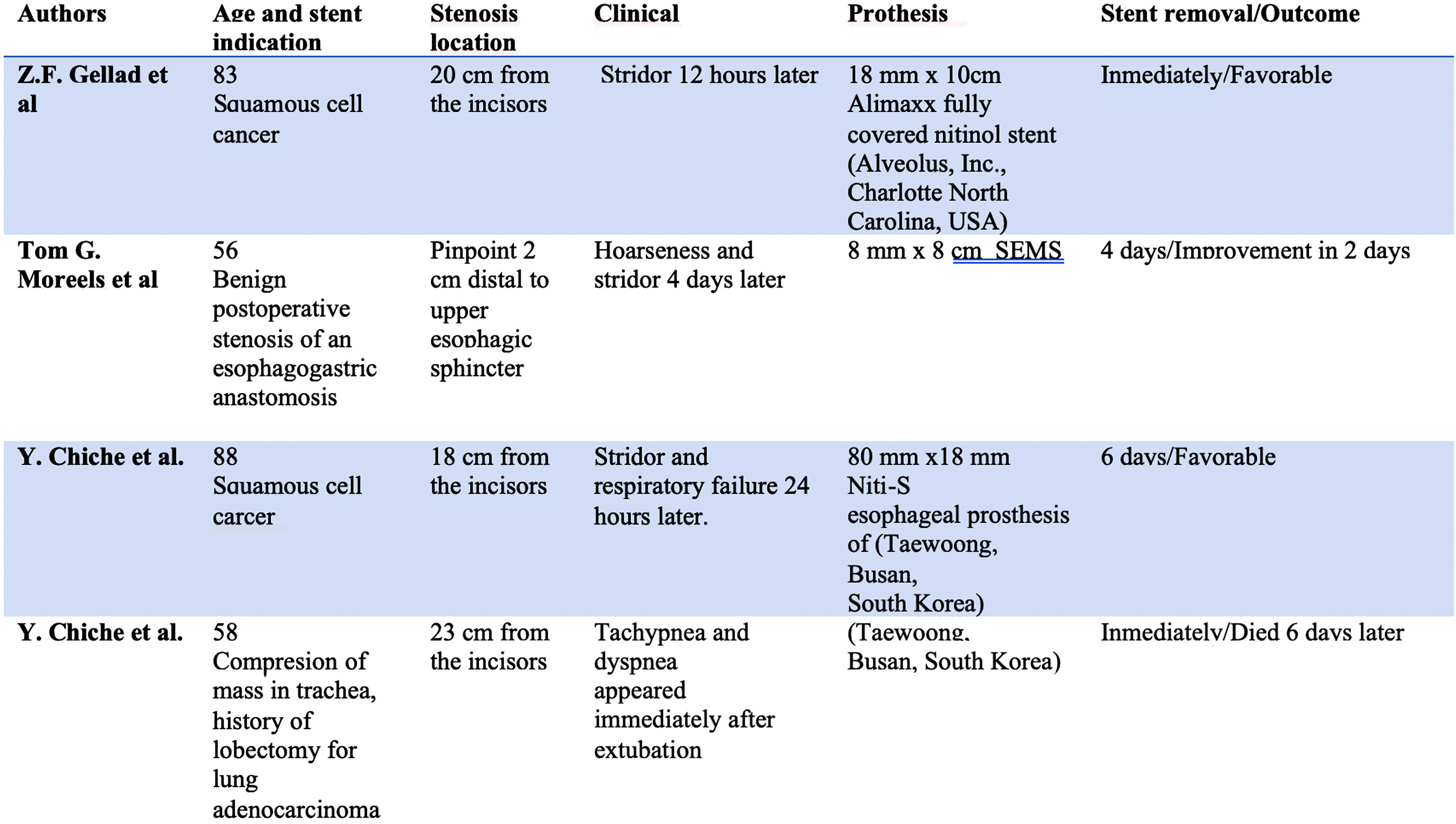
Transient BVCP secondary to SEMS placement is a very rare complication, with only four cases described in literature (Table 1).3 Fortunately, a favorable recovery should be expected when treated promptly. Therefore, it must be beared in mind by endoscopists when placing esophageal SEMS.
Physiopathological mechanisms include direct compression from the esophageal stent inducing neuropraxia of the posterior branch of the recurrent laryngeal nerve and/or spasms secondary to local inflammation in the interarytenoid muscles.4,5
No recommendations on the therapeutic approach are available but tracheostomy should be aware of respiratory symptoms after SEMS placement in order to remove the stent as soon as possible.

