





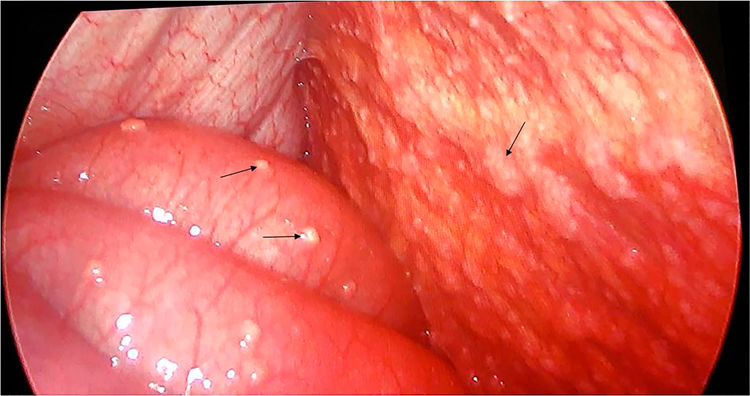
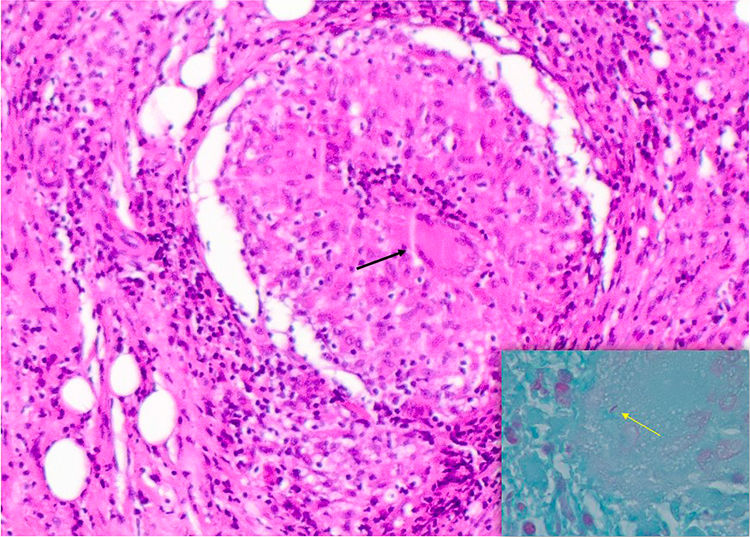
A 26-year-old man with a 3-week history of mesogastric and left-lower-quadrant abdominal pain with vomit and fever. He had abdominal distension and pain in the left lower quadrant. Laboratory studies showed a white-cell count of 15,000ml3 (reference range 4000–10,000) and C-reaction protein value of 15mg/dl (reference range 0–0.5). Abdominal computed tomography revealed free intraabdominal fluid and contrast capture in the peritoneum (Fig. 1) that suggests peritonitis. The exploratory laparoscopy revealed miliary implants throughout the peritoneal cavity and parietal and visceral peritoneum (Fig. 2). The presence of necrotizing granulomatous inflammation with multinucleated giant cells (Fig. 3A) and acid–alcohol resistant bacillus (Fig. 3B) in histological examination of miliary implant biopsy confirms the diagnosis of intestinal tuberculosis (TB). The patient was treated with a 6-month course of anti-tubercular drugs with a good evolution.
.")
.")
 Hematoxiline–eosine stain with necrotizing granulomatous inflammation with multinucleated giant cells (black arrow). (B) Ziehl Neelsen stain with presence of acid–alcohol resistant bacillus (yellow arrow).")
Abdominal TB is the sixth most frequent extrapulmonary site and only in 20% of cases the lung is involved. An inespecifical abdominal pain is present in 80–90% of patients, and less frequently fever, weight loss, small bowel obstruction.1,2 The most common CT findings include high-density lymphadenopathy, ascites and thickening and/or nodularity of the peritoneal surfaces. These CT findings are non-pathognomonic.3 Antituberculous drugs are the primary treatment.4
Conflicts of interestThe authors have no conflicts of interest to declare.

