




An 18-year-old male presented to the emergency department with a chief complaint of lower abdominal pain of severe intensity for 8h. His medical history revealed a left diaphragmatic hernia repair two years earlier. Physical examination was unremarkable except for inconclusive Blumberg's sign. Blood tests showed high levels of C-reactive protein [266mg/dL] and leukocytosis [15,130cells/mm3].
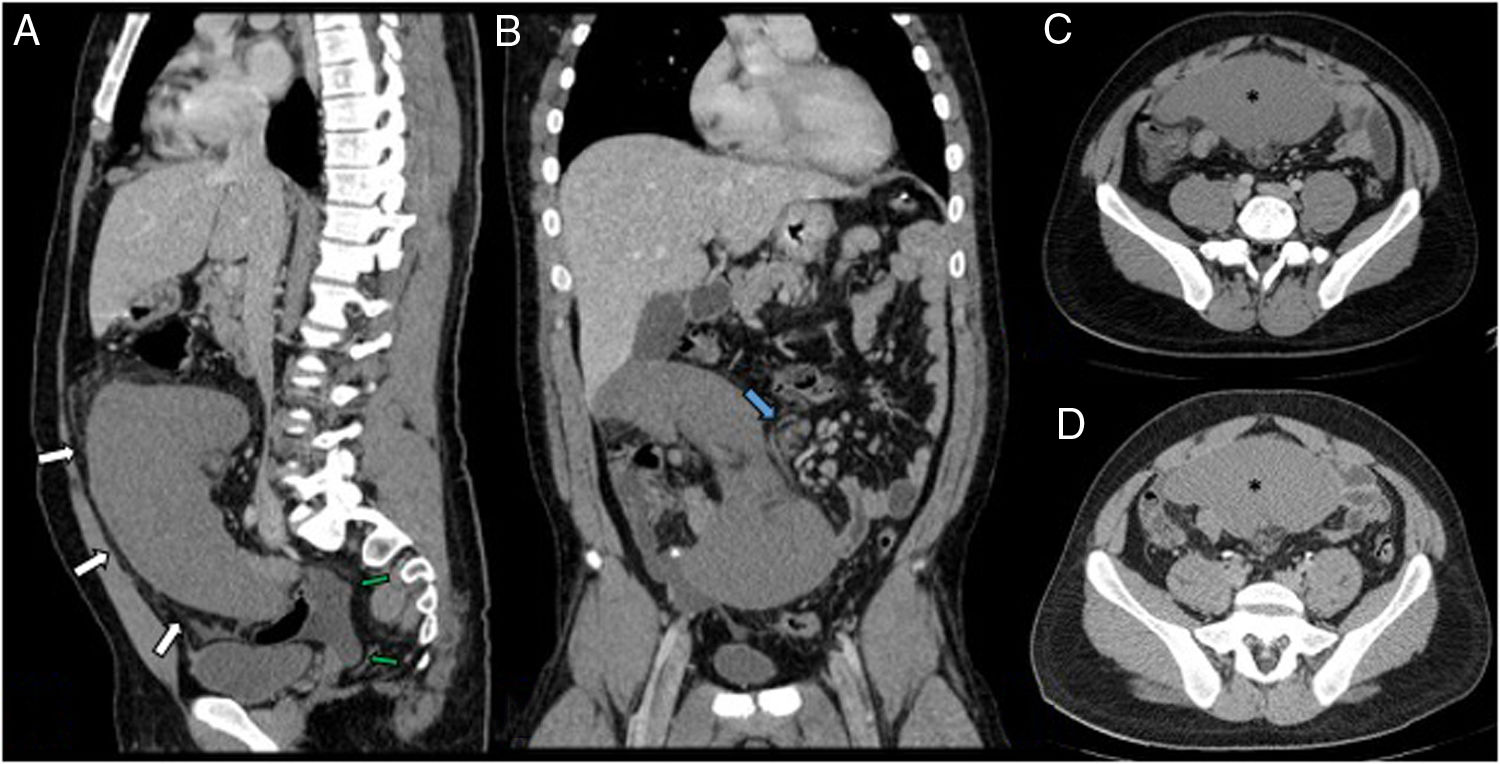
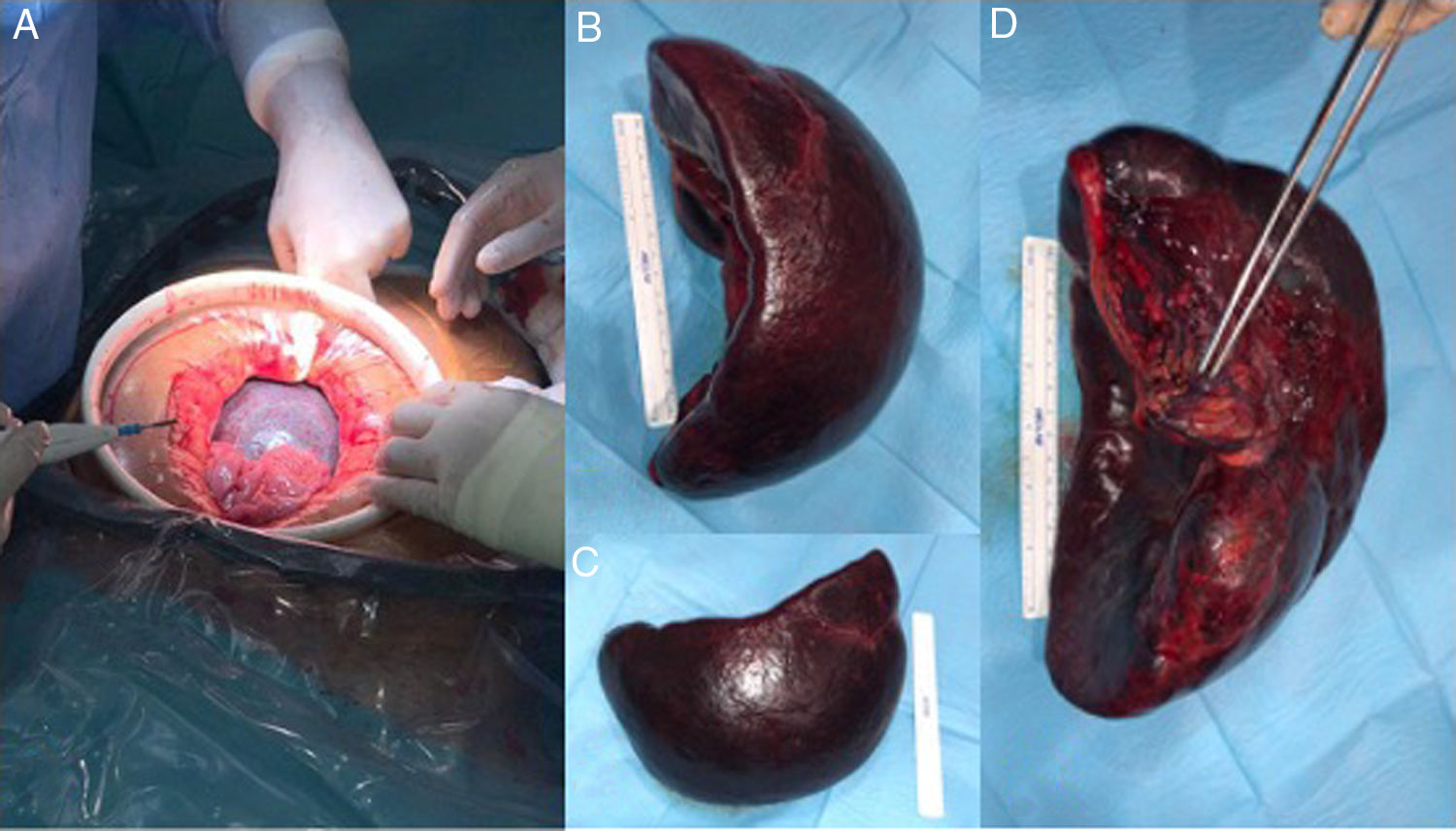
Abdominal ultrasound and subsequent CT scan (Fig. 1) revealed that the spleen was not located in the left upper quadrant. A low-enhancing, comma-shaped mass was observed in the hypogastric region showing twisting of its pedicle (“swirl” sign). These findings were consistent with torsion of a wandering spleen with established infarction, thus emergent splenectomy was performed (Fig. 2). The patient evolved favourably and has remained asymptomatic to date.
 and delayed (D) phases. Sagittal (A) and coronal (B) reformatting. Hypogastric mass corresponding to enlarged spleen. Inflammatory changes and peri-splenic fluid (green arrows) can be seen. In the coronal view, torsion of the splenic vessels with abnormal surrounding fat is shown (blue arrow). No significant differences in the enhancement pattern between the portal and delayed phases are observed (asterisk in C and D).")
Contrast-enhanced abdominal CT in portal (A–C) and delayed (D) phases. Sagittal (A) and coronal (B) reformatting. Hypogastric mass corresponding to enlarged spleen. Inflammatory changes and peri-splenic fluid (green arrows) can be seen. In the coronal view, torsion of the splenic vessels with abnormal surrounding fat is shown (blue arrow). No significant differences in the enhancement pattern between the portal and delayed phases are observed (asterisk in C and D).
. The spleen showed an ischaemic appearance and torsion of the pedicle was found. (B–D) Surgical specimen consisting of a congestive and enlarged spleen (B, C) with torsion of its pedicle (D).")
Wandering spleen consists of the ectopic location of the spleen.1 Although patients are usually asymptomatic, its torsion may lead to an acute abdomen. Contrast-enhanced CT scan is a cornerstone diagnostic exam in the emergency setting and typical findings include absence or abnormal rotation of the spleen in the left upper quadrant and a “comma” shaped mass in the abdomen.2 Treatment requires emergent splenopexy or splenectomy based on the presence of infarction, either through laparotomy or laparoscopy.3

