



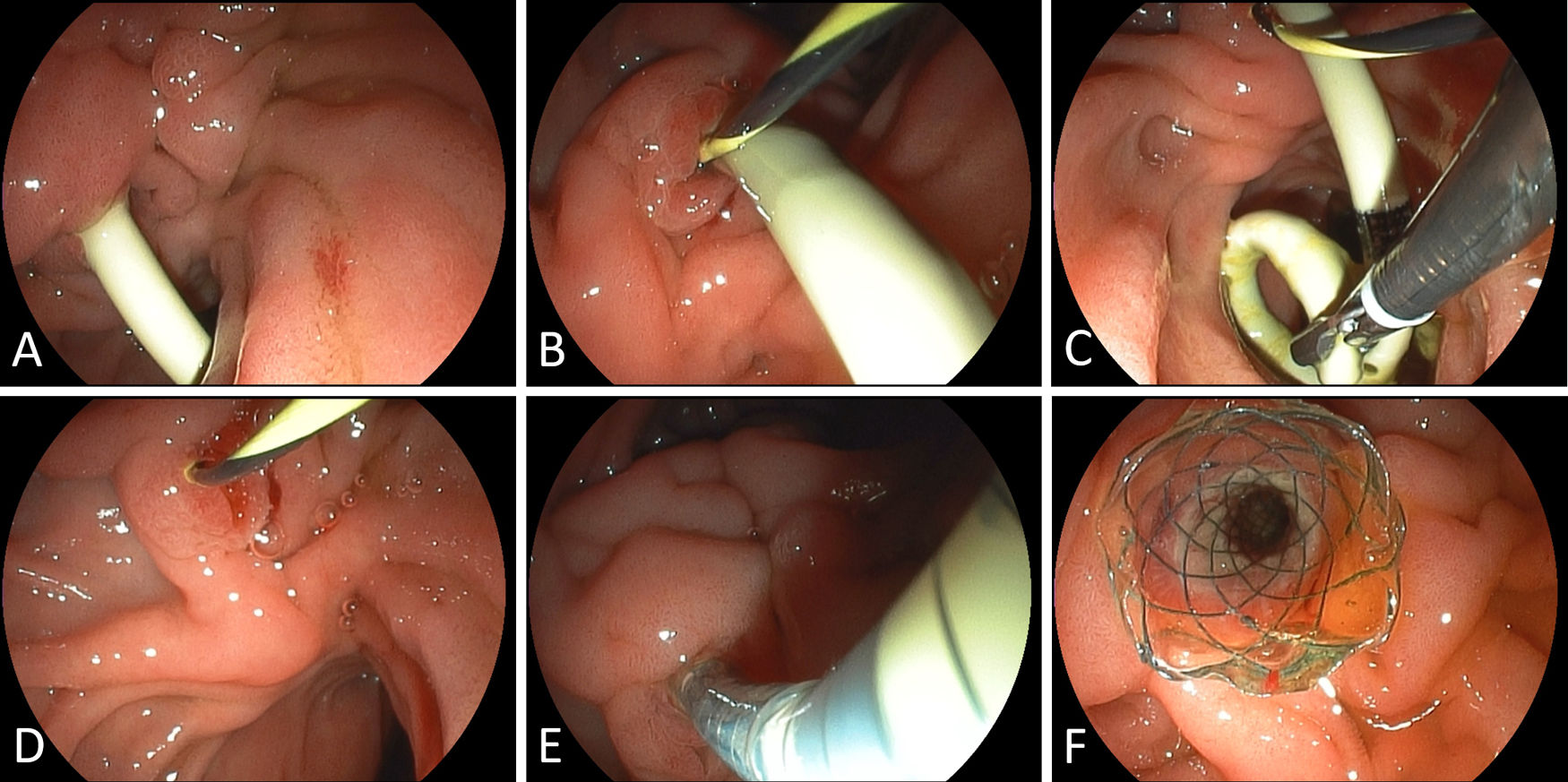
A 78-year-old woman presented with severe cholestasis (bilirubin 11.9mg/dL) and weight loss resulting in profound cachexia (body mass index 15.2kg/m2) of multifactorial etiology (exocrine pancreatic insufficiency, poor nutrition on a quantitative and qualitative level). Medical history was significant for critical alcohol consumption and an episode of acute pancreatitis >20 years ago. Transabdominal ultrasound and computed tomography indicated advanced calcified chronic pancreatitis with marked biliary dilation and minor pancreatic duct dilation. The patient underwent endoscopic-retrograde cholangiopancreatography (ERCP) revealing a complex tight and hard-to-cross biliary stricture, thus a 10-Fr biliary plastic stent was inserted. Pancreatic duct intervention was not entertained in the absence of pancreatic-type pain. Following this cholestasis parameters were significantly improved including normalization of bilirubin levels and the patient's weight stabilized under pancreatic enzyme substitution for fecal elastase-confirmed exocrine insufficiency. Given that an additional endoscopic ultrasound (EUS) did not clearly suggest malignancy over pancreatitis-related benign biliary stricture and the patient was a very poor surgical candidate, temporary metal stenting using a 60×10-mm fully-covered self-expanding metal stent (FCSEMS) was performed. Due to difficulties in transversing the stricture at index ERCP we opted for a “two-devices-in-one-channel”-approach for a guidewire-secured plastic-to-metal stent switch. First, the papilla with the indwelling 10-Fr double-pigtail plastic stent was visualized (Fig. 1A) and a 0.035-in guidewire inserted alongside the stent by an ERCP cannula. (Fig. 1B) Next, a grasper was inserted through the 4.2-mm working channel of the therapeutic duodenoscope next to the guidewire left in place and the most distal part of the plastic stent grasped (Fig. 1C) and extracted through the scope (Fig. 1D). Finally, the FCSEMS was inserted over the guidewire (Fig. 1E) and deployed as per standard procedure. (Fig. 1F) In addition, supplementary oral nutrition and pancreatic enzyme replacement was initiated.
 Duodenoscopic visualization of the indwelling 10-Fr biliary double pigtail plastic stent. (B) Successful 0.035-in guidewire placement alongside the stent after initial alignment with an ERCP cannula. (C) After additional insertion of a grasper through the 4.2mm working channel of the therapeutic duodenoscope, the most distal stent end was grasped. (D) Next, the plastic stent was extracted through the scope with the guidewire left in situ. (E) Insertion of the FCSEMS application system. (F) Documentation of optimal FCSEMS placement.")
(A) Duodenoscopic visualization of the indwelling 10-Fr biliary double pigtail plastic stent. (B) Successful 0.035-in guidewire placement alongside the stent after initial alignment with an ERCP cannula. (C) After additional insertion of a grasper through the 4.2mm working channel of the therapeutic duodenoscope, the most distal stent end was grasped. (D) Next, the plastic stent was extracted through the scope with the guidewire left in situ. (E) Insertion of the FCSEMS application system. (F) Documentation of optimal FCSEMS placement.
Taken together, the “two-devices-in-one-channel” approach represents an easy-to-accomplish trick of the trade out of the interventional endoscopists toolbox to avoid troublesome re-cannulation manoeuvres in difficult strictures.
Financial disclosureThe author discloses no financial relationships relevant to this publication.
Conflict of interestThe author states no conflict of interest.

