




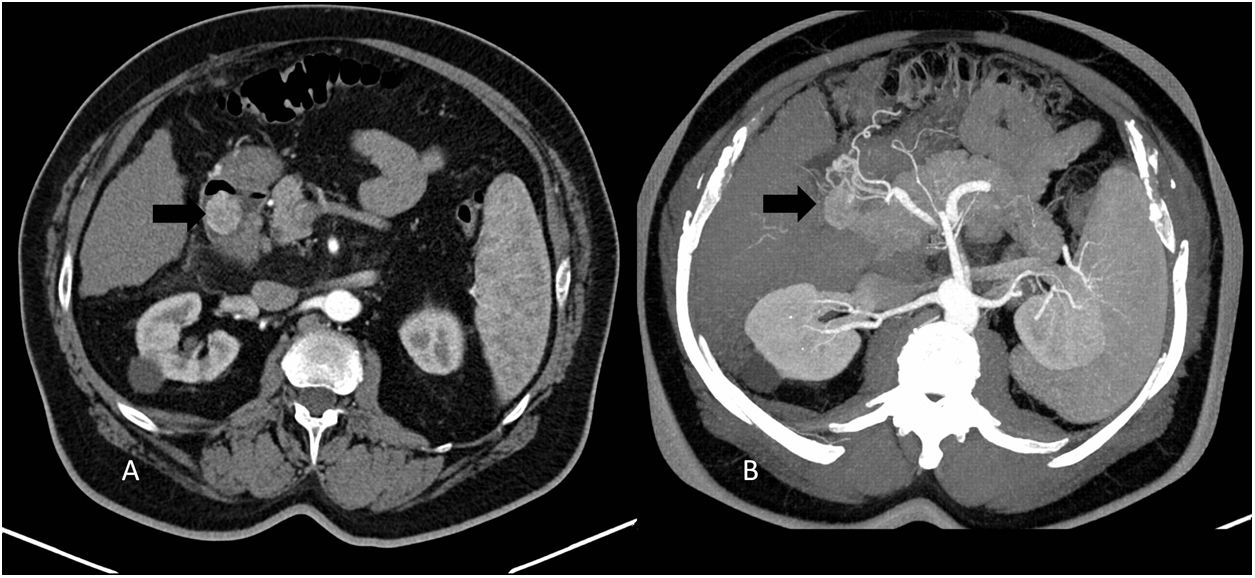
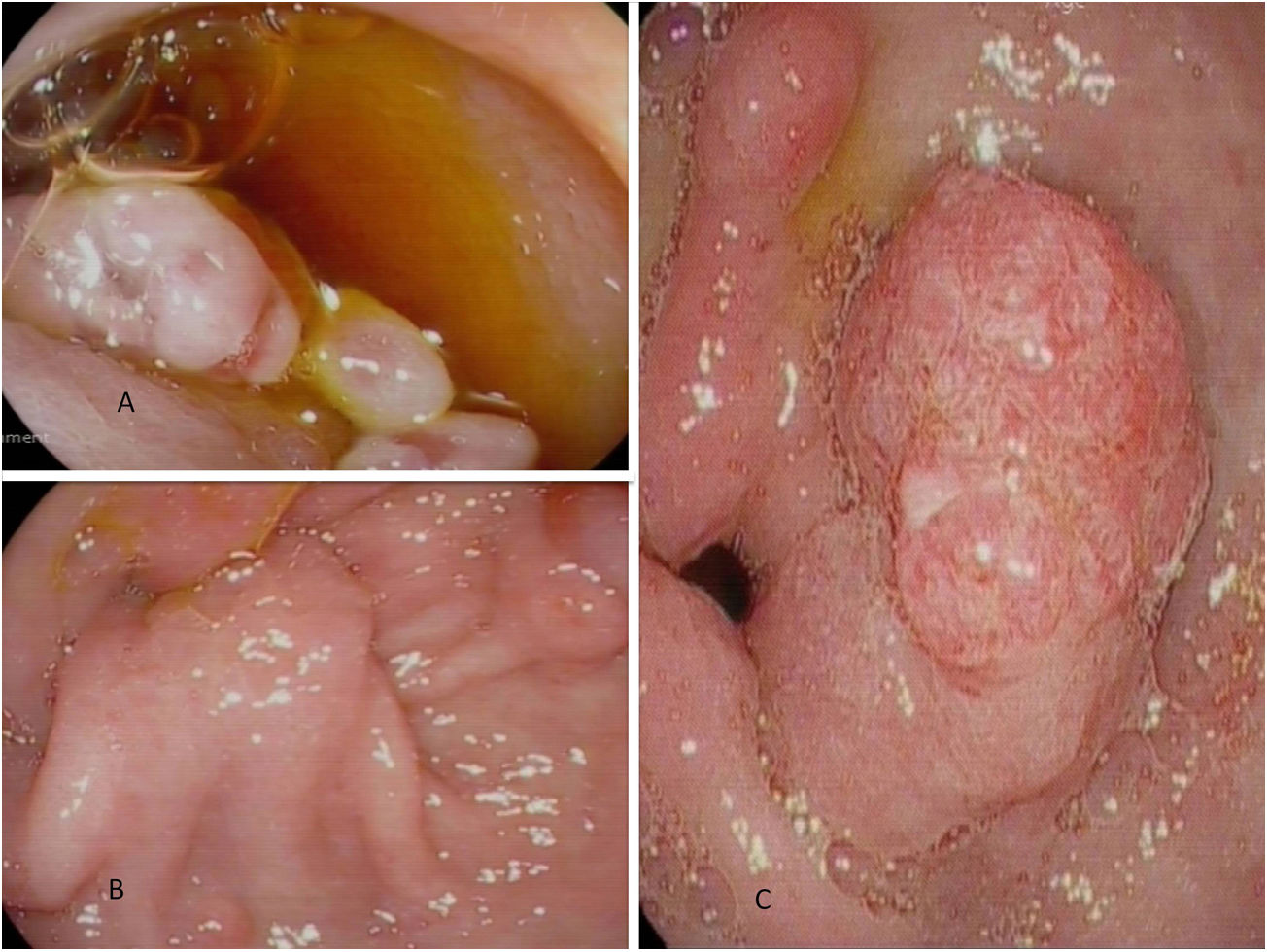
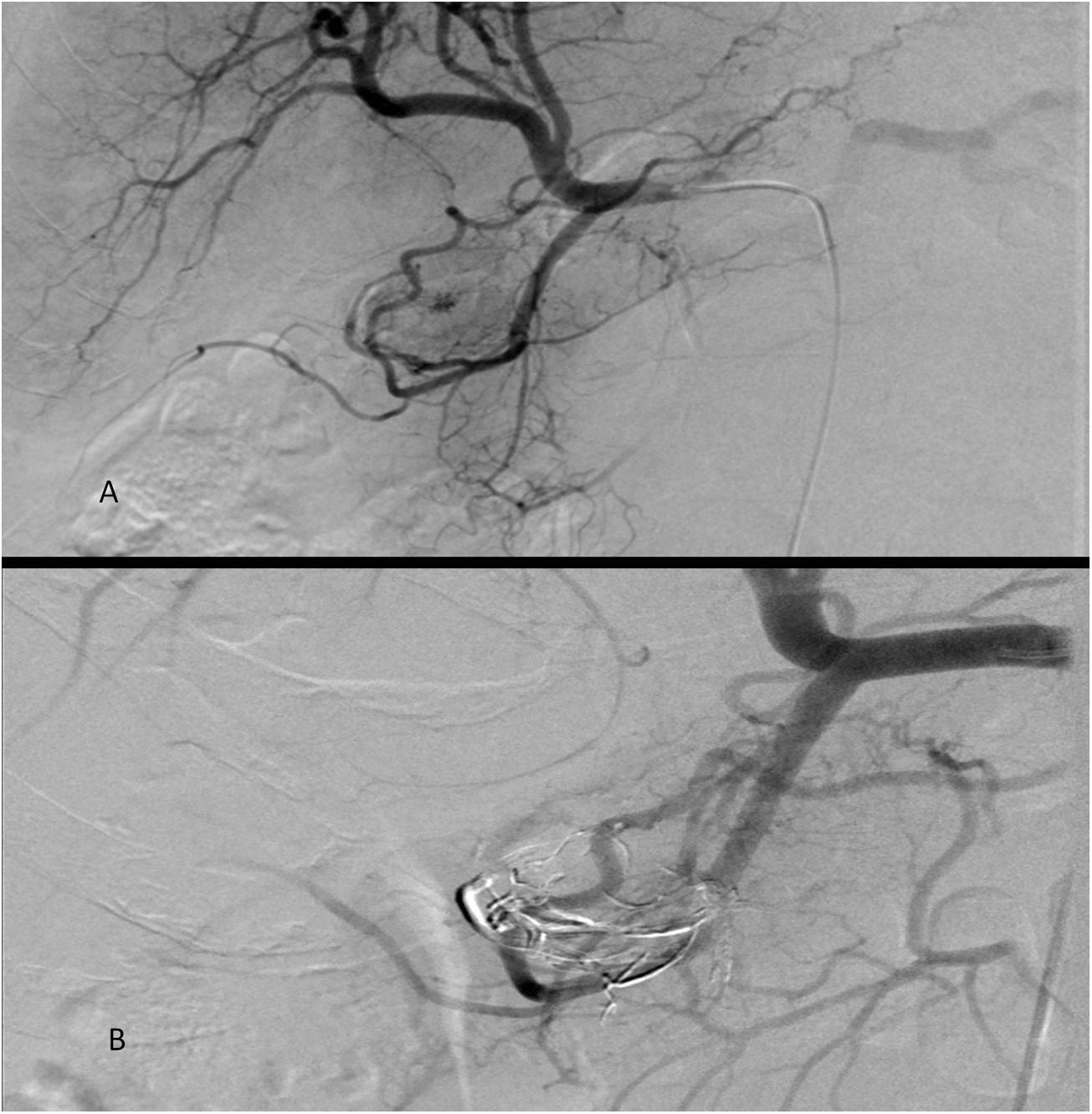
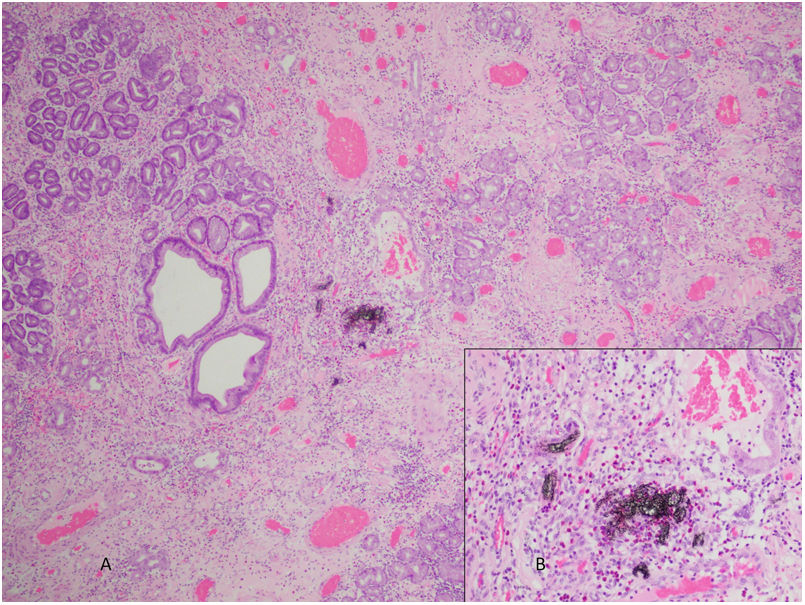
A 69-year-old male with a history of compensated liver cirrhosis. The abdominal computed tomography (CT) revealed a 27-mm polyp in the proximal duodenum with marked enhancement in the arterial phase, including a branch of the gastroduodenal artery in the pedicle (Fig. 1A and B). The gastroscopy showed a gastric polyp with a pedicle in the antrum entering through the pylorus with its head in the duodenal bulb (Fig. 2A and B). Due to its size, a polypectomy was indicated. To minimise the risk of complications, the decision was taken to perform a selective embolisation of the arteries located on the duodenal arch that fed the lesion with ethylene vinyl alcohol first (Fig. 3A and B). In a follow-up abdominal CT scan, the polyp presented reduced enhancement in the arterial phase and a reduction in size, also confirmed by the endoscopy (Fig. 2C). Finally, an endoscopic polypectomy was performed without complications. The pathological diagnosis was hyperplastic polyp (Fig. 4A and B)
. B: Maximum-intensity projection abdominal CT scan showing the arterial branches that go towards the polyp (arrow).")

A: Head of the pedunculated polyp in the duodenal bulb; It is difficult to visualise because it occupies a large part of the bulb. B: Pedicle of the polyp in the antrum, entering through the pylorus. C: Image of the polyp following embolisation; a significant reduction in size is observed.


A: Histological section with 10X magnification showing hyperplastic polyp with embolisation material in its sinus. B: 40X magnification of the area where the embolisation material is located, showing acute inflammatory infiltrates in the adjacent areas, with predominantly eosinophilic polymorphonuclear cells and some multinucleated giant cells.
Post-polypectomy haemorrhage in gastric lesions is a rare complication that occurs in up to 7.2%1 of patients and in some cases requires arterial embolisation2. Performing this procedure prophylactically to avoid bleeding has not been described. In our case, it served to prevent haemorrhagic complications and managed to reduce lesion size, facilitating endoscopic resection.
