




A 75-year-old man, with only history of Y roux gastrectomy for a peptic ulcer, presented to the emergency room with vomiting and abdominal pain. Physical examination revealed drowsiness, hypotension, tachycardia, hypoxemia, anuria, and tenderness in the right upper quadrant of the abdomen. Laboratory studies revealed a leukocytosis (26,000/μL), and elevated C-reactive protein 35mg/dL, procalcitonin 137ng/mL and lactate 91mg/dL. Liver enzymes were raised (AST 409U/L, ALT 243U/L) and total bilirubin was slightly elevated (1.53mg/dL). The patient was hemodynamically stabilized.
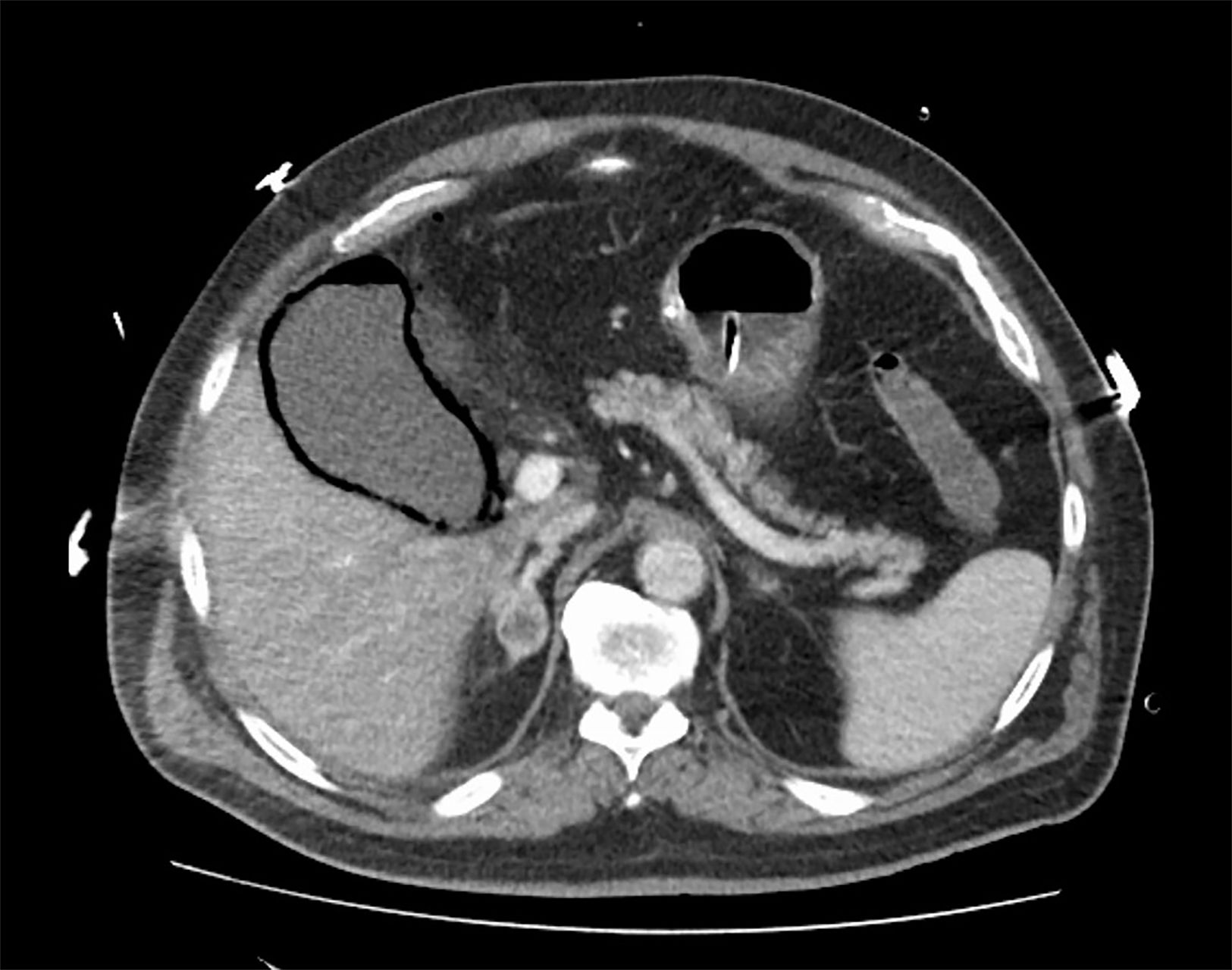
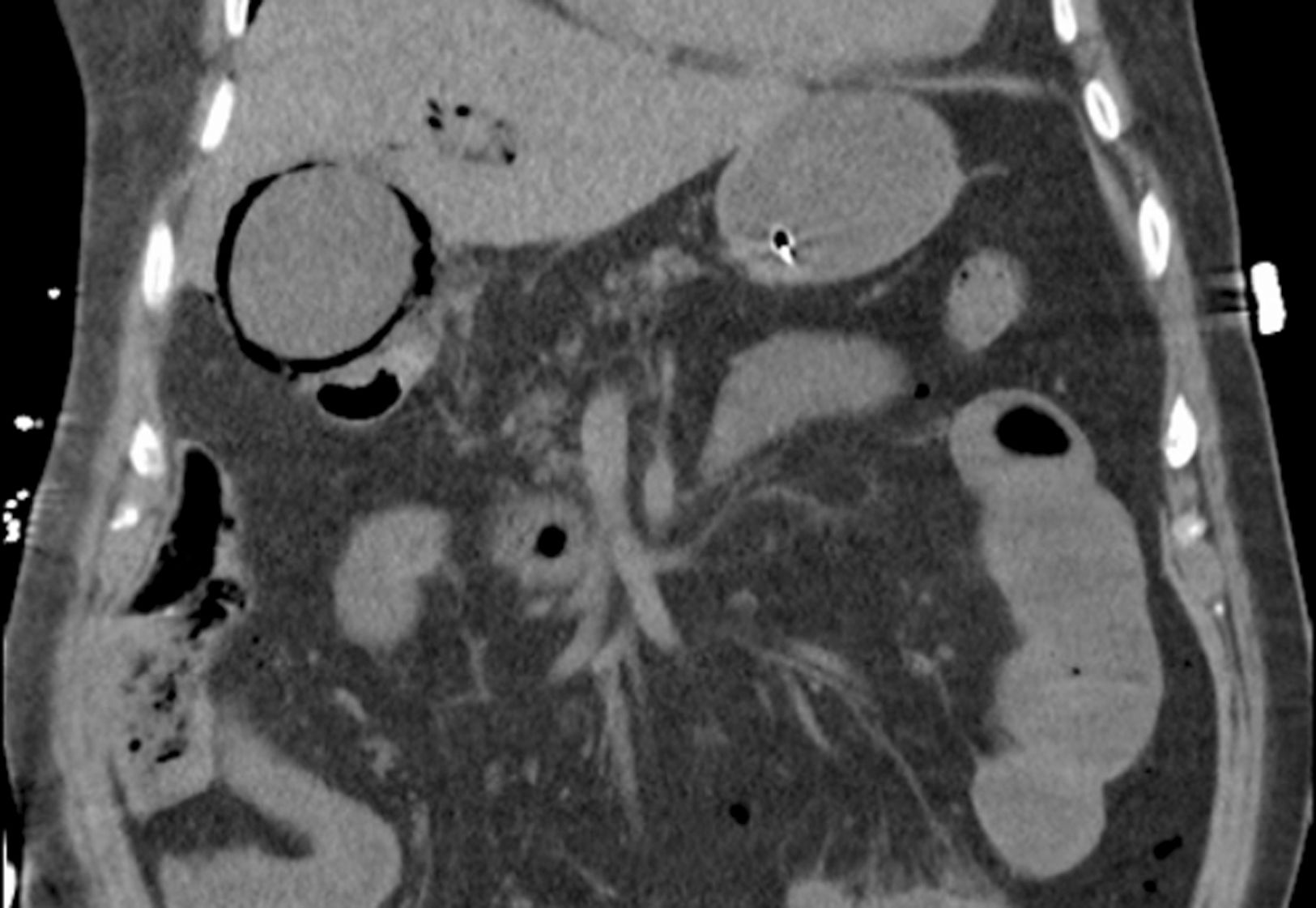
Abdominal computed tomography presented gas in the wall of the gallbladder with air in the lumen (Fig. 1) and air in the intrahepatic biliary tract (Fig. 2).


Septic shock was assumed due to an emphysematous cholecystitis (EC) and initiated organ support and antibiotic (meropenem). Emergent surgery was performed with resection of an inflamed gallbladder with multiple gallstone. Blood cultures grew Klebsiella pneumoniae. Unfortunately, the patient didn’t survive.
EC is an uncommon complication of acute cholecystitis, occurring in 1–4%.1 Despite having a very similar presentation with uncomplicated cholecystitis, EC has a high risk of perforation with peritonitis and consequent septic shock.1,2 Mortality is around 15–25%.1 Image evaluation is essential to early diagnosis and it is pathogmonic.3
Conflict of interestNo conflicts of interest to declare.
