




Foreign bodies (FB) are a common problem and the second leading cause of endoscopic emergencies in our hospitals.
We present the case of an 80-year-old male with Alzheimer's disease who came to Accident and Emergency with a 24-h history of epigastric pain, which began after a large meal. In Accident and Emergency, the patient had haematemesis, but was haemodynamically stable. Gastroscopy showed an FB with a pointed-end embedded in the gastric antrum with a blood clot attached (Fig. 1A). The end of the FB was pulled out with crocodile forceps, finding it to be a toothpick, with 75% of its length having been embedded in the gastric wall (Fig. 1B). After removing the toothpick, three haemostatic clips were placed over the wound (Fig. 1C). Subsequent CT scan showed small extraluminal air bubbles and marked cross-linking of the adjacent fat in the region of the antrum, next to the metal clips (Fig. 1D), in addition to a collection of what appeared to be blood close to the gastric fundus, suggesting perforation. The patient was managed conservatively and made a good recovery.
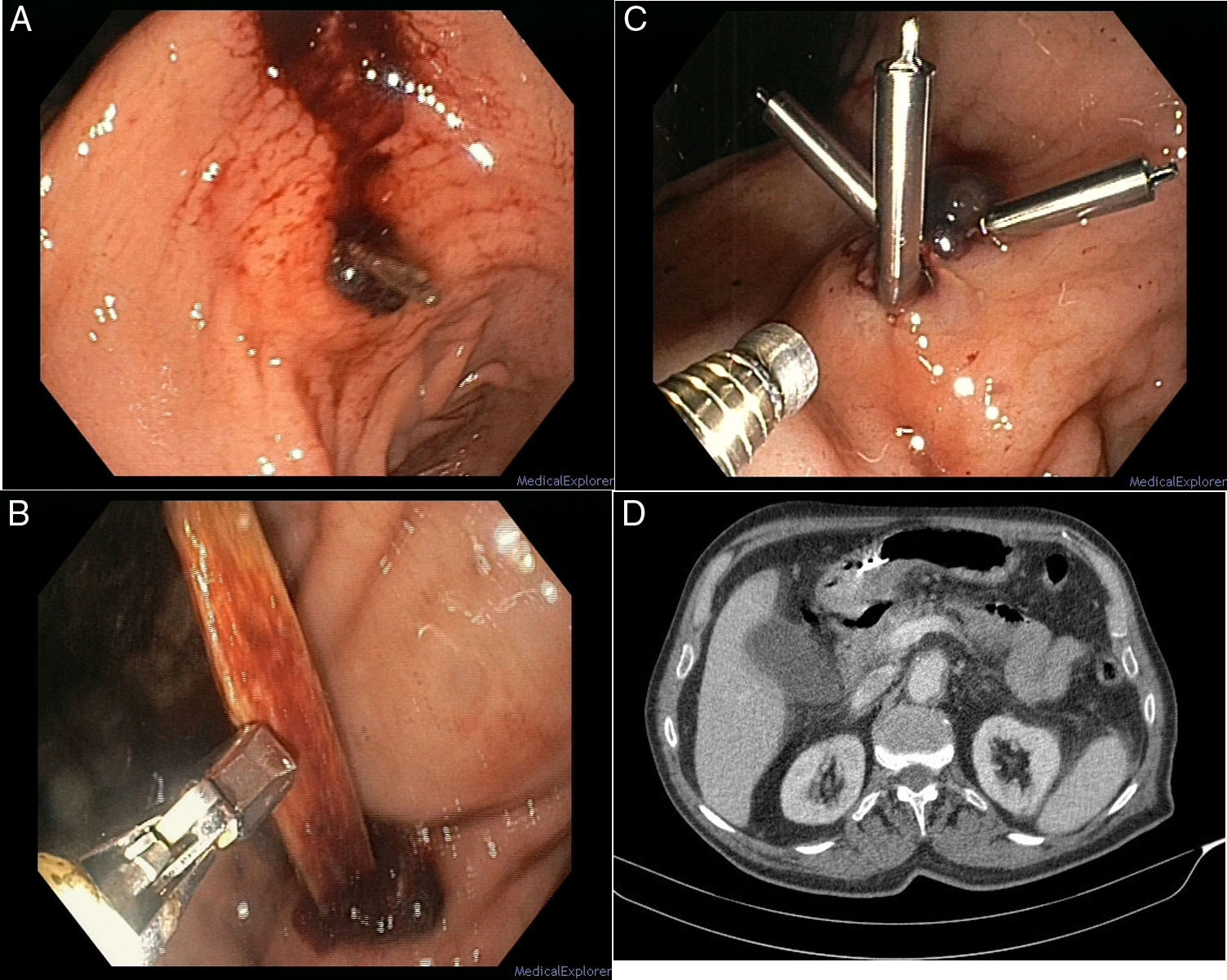
 Endoscopic image of a foreign body (FB) with a pointed end embedded in the gastric wall with a clot attached. (B) Extraction of the FB with crocodile forceps, discovering that it was a toothpick. (C) Placement of 3 haemostatic clips over the wound. (D) CT scan of the abdomen showing extraluminal air bubbles and inflammatory signs in the gastric wall.")
(A) Endoscopic image of a foreign body (FB) with a pointed end embedded in the gastric wall with a clot attached. (B) Extraction of the FB with crocodile forceps, discovering that it was a toothpick. (C) Placement of 3 haemostatic clips over the wound. (D) CT scan of the abdomen showing extraluminal air bubbles and inflammatory signs in the gastric wall.
As FB with sharp or pointed edges can easily pass through the gastrointestinal tract wall, the risk of complications is high. The most common of these are animal or fish bones. In the past, treatment of FB perforating the gastrointestinal wall was always surgical. Nowadays, however, endoscopic management is recommended as the first option, in view of the high likelihood of the condition resolving and the lower rate of secondary complications.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Cebrián García A, Borobio Aguilar EL, Ruiz-Clavijo García D. Perforación gástrica por palillo. Gastroenterol Hepatol. 2019;42:445–446.
