




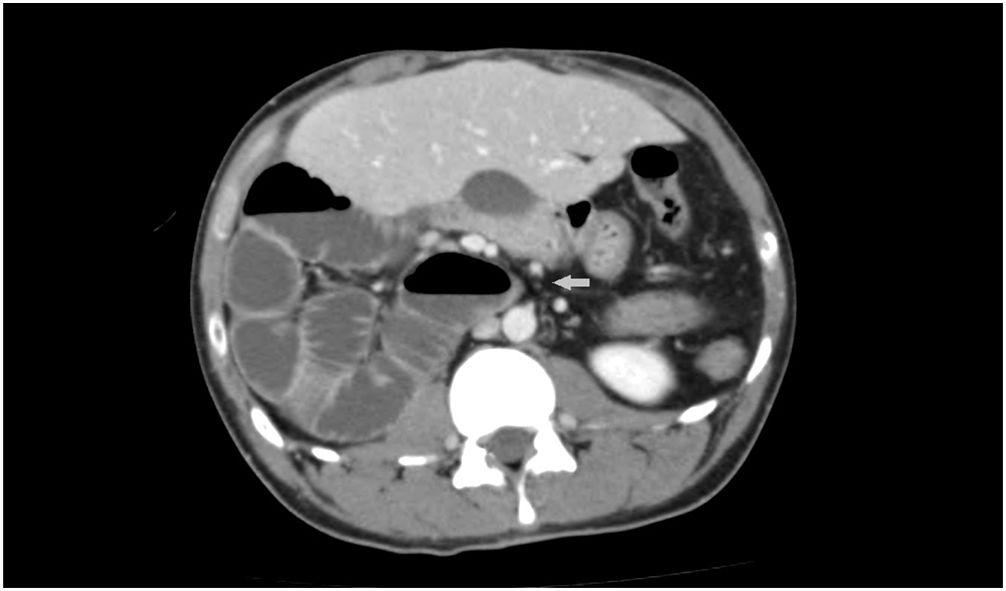


A 34-years-old man consulted for recurrent abdominal pain for the past 14 years. Abdominal ultrasound, upper endoscopy up to the second duodenal portion, celiac disease and Helicobacter pylori exams displayed normal results. He was admitted to our emergency department with a new flare of mesogastric pain which worsened with meals and was easily controlled with conventional analgesia. Physical examination and blood tests were normal. A CT-scan (Figs. 1 and 2) and barium studies (Fig. 3) were performed, revealing location of the large bowel on the left side of the abdomen, a right-sided small intestine and abnormalities in the disposition of vascular structures.
.")


The patient was diagnosed with intestinal malrotation, which results from an abnormal intestinal rotation during embrionary development. Usually diagnosed during the first decade of life, the estimated prevalence in adults is around 0.2%. It may present as an acute complication (volvulation, intestinal ischemia), but can also lead to chronic symptoms such as intermittent abdominal pain. Surgery (Ladd's procedure) is the treatment of choice for patients with complications. Nevertheless, surgical treatment in mild or non-symptomatic patients remains controversial, although many experts stand up for the intervention. In this case, avoidance of copious meals and conventional analgesia improved the symptoms.
