




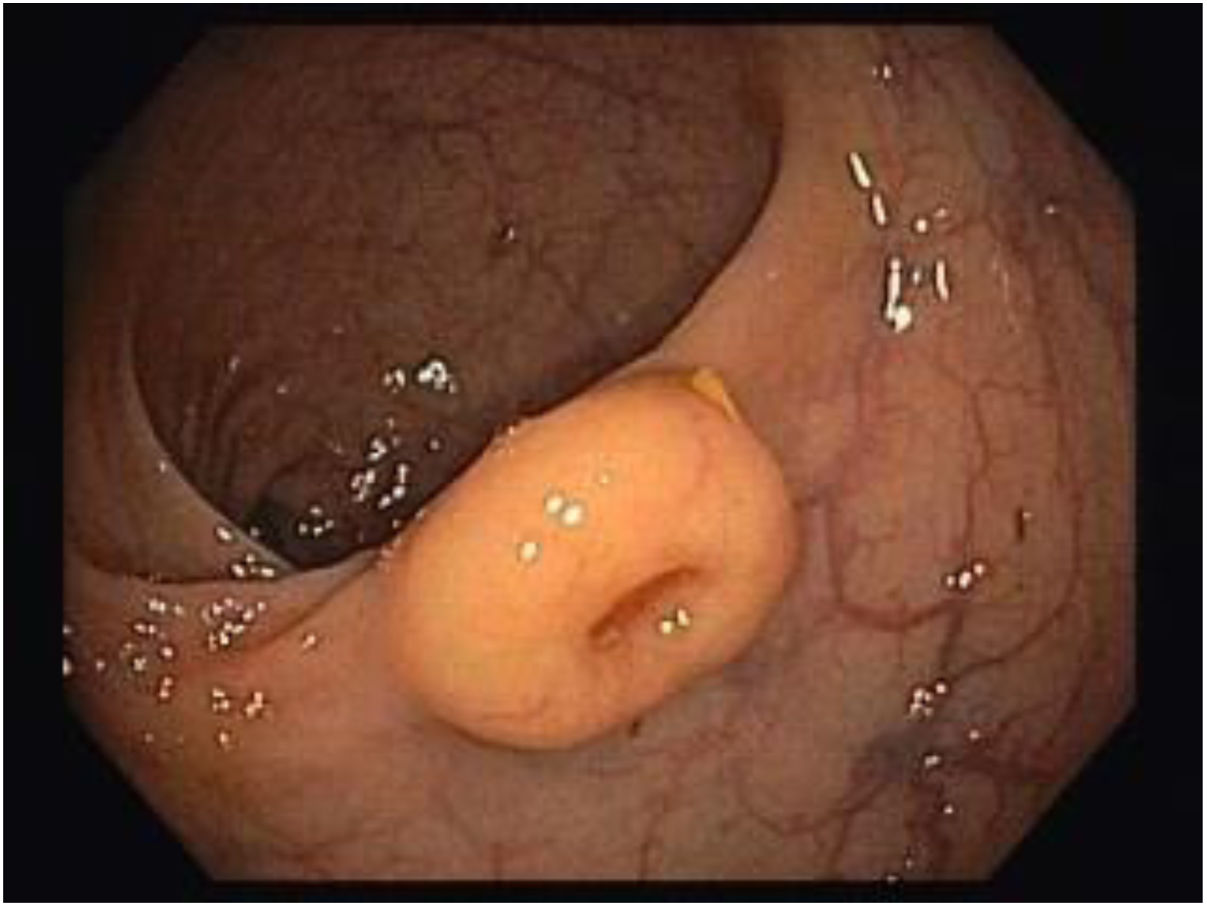
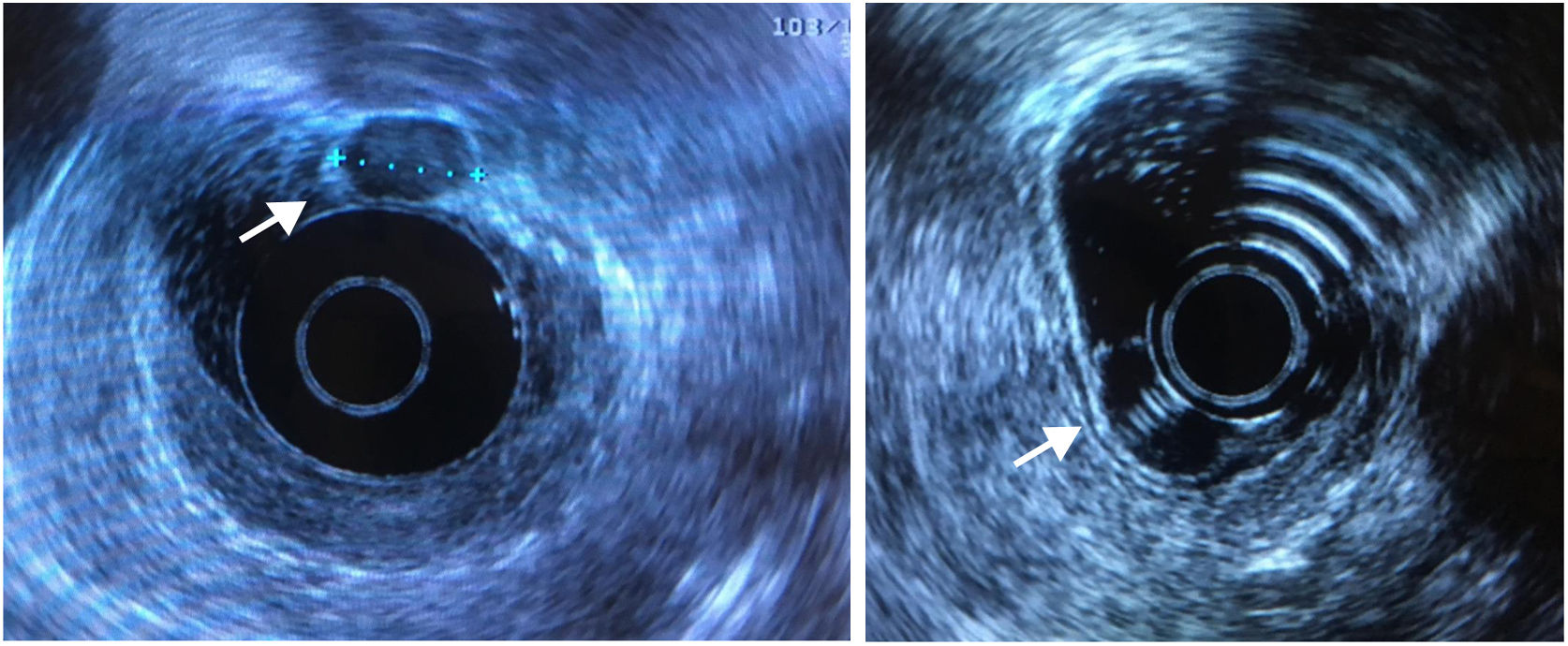
A 60-year-old woman performed a screening colonoscopy, which showed, in the midrectum, a 12mm, sessile, subepithelial lesion covered with yellow discolored mucosa, with a central depression (Fig. 1). Conventional biopsies showed non-specific inflammatory infiltrate. Rectum endoscopic ultrasound showed an hypoechoic lesion with 12mm, homogeneous, well delimited, originating in the muscularis of the mucosa with no lymph nodes or muscularis propria involvement (Fig. 2). Thoraco-abdomino-pelvic computed tomography showed no locoregional/distant metastasis. An endoscopic mucosal resection of the lesion in a single fragment was performed. Histopathology showed a 12×8×9mm, well-differenciated neuroendocrine tumor (NET) G1 (WHO classification, <2mitoses/10 HPF, Ki-67<2%), with no linfovascular invasion and with free margins. One-year later, the patient repeated colonoscopy with biopsies which showed no evidence of recurrence.

, homogeneous, well delimited, originating in the muscularis of the mucosa with no lymph nodes or muscularis propria involvement.")
Rectal NETs (R-NET) represent approximately one-third of all gastroenteropancreatic NETs.1–3 Due to the widespread use of screening colonoscopy, the incidence of R-NET has been increasing. The majority are small, well-differentiated, limited to the submucosal layer, with a good prognosis. Endoscopic ultrasound is essential to assess tumor size, depth of invasion and presence of lymph node invasion, in order to determine the appropriate treatment strategy.1,2,4 This case underscores the importance of early identification and optimal management of these tumors.
Author contributionsCarolina Simões and Sofia Carvalhana were responsible for elaborating the manuscript. Leonor Xavier de Brito, Luís Carrilho Ribeiro and Rui Tato Marinho were responsible for the critical review of the manuscript.
The manuscript, including related data, figures and tables have not been previously published and are not under consideration for publication elsewhere.
Informed patient consentObtained.
FundingThe authors have received no funding.
Conflicts of interestThe authors have no conflicts of interest to report.
