


Groove pancreatitis is an uncommon cause of chronic pancreatitis that affects the groove anatomical area between the head of the pancreas, duodenum, and common bile duct.
Clinical caseA 67-year-old man with frequent biliary colic and an alcohol consumption of 30–40g/day was admitted to the hospital complaining of jaundice and pruritus. Laboratory analysis revealed cholestasis and the ultrasound scan showed intra-hepatic biliary ducts dilatation, middle third cystic dilatation of common bile duct, enlarged Wirsung and pancreatic atrophy. The magnetic resonance cholangiopancreatography showed imaging findings compatible with groove pancreatitis. An esophagogastroduodenoscopy later excluded duodenal neoplasia. He was submitted to a Roux-en-Y cholangiojejunostomy because of common bile duct stricture. Five months later a gastrojejunostomy was performed due to a duodenal stricture. The patient remains asymptomatic during follow-up.
DiscussionGroove pancreatitis is a benign cause of obstructive jaundice, whose main differential diagnosis is duodenal or pancreatic neoplasia. When this condition causes duodenal or biliary stricture, surgical treatment can be necessary.
A pancreatite da goteira duodeno-pancreática é uma forma rara de pancreatite crónica, que afeta a área anatómica entre a cabeça do pâncreas, duodeno e ducto biliar comum.
Caso ClínicoDoente do sexo masculino, 67 anos, com antecedentes de cólicas biliares de repetição e consumo etílico de 30-40 g/dia, internado por icterícia e prurido. Analiticamente, apresentava colestase e, ecograficamente, dilatação moderada das vias biliares intra-hepáticas (VBIH), dilatação quística do 1/3 médio do colédoco, ectasia do Wirsung e atrofia pancreática. A colangiopancreatografia por ressonância demonstrou aspetos imagiológicos compatíveis com pancreatite paraduodenal. A endoscopia alta excluiu neoplasia duodenal. Foi submetido a colangiojejunostomia em Y Roux por estenose do colédoco e após 5 meses a gastrojejunostomia por estenose duodenal. O doente mantem seguimento, permanecendo assintomático.
DiscussãoA pancreatite paraduodenal é uma forma benigna de icterícia obstrutiva, cujo principal diagnóstico diferencial é a neoplasia duodenal/pancreática. Quando esta condição causa estenose duodenal ou biliar, a terapêutica cirúrgica poderá ser necessária.
Groove pancreatitis is a rare and under-recognized subtype of chronic pancreatitis that affects the anatomical region composed by the duodenum, pancreatic cephalic portion and common biliary duct (CBD).1–3 The prevalence of this condition in pancreaticoduodenectomy specimens of patients with chronic pancreatitis has been reported to be as high as 24.5%.4 Pathogenesis is still unclear, but it involves a fibrotic inflammation,5 that could cause biliary stricture, with obstructive jaundice or duodenal stricture along with vomiting. The main differential diagnosis is the pancreatic head, CBD or duodenal neoplasia, which imply different management and prognosis. Commonly, this condition can be resolved with conservative treatment. In rare cases of clinical relevant biliary or duodenal stenosis, surgical treatment is necessary.2,6
2Clinical caseThe authors present a case of a 67-year-old man, with a history of repeated biliary colic. He had an alcohol consumption of 30–40g/day and refused cholecystectomy. He presented to the emergency department with a two days evolution of painless jaundice, dark colouration of the urine and generalized pruritus. He denied having had any blood transfusion, new drugs prescription or over-the-counter drugs, fava bean consumption, previous surgeries, recent travels or unprotected sexual intercourse. He had no previous jaundice episodes or recent infections. The physical examination revealed jaundice of mucosa and skin. The remaining physical exam was unremarkable.
Laboratory analysis showed predominant cholestatic hepatitis with aspartate aminotransferase 908 (<35U/L), alanine aminotransferase 1236 (<45U/L), alkaline phosphatase 1581 (40–150UL), gamaglutamyl-transpeptidase 2753 (<55U/L), total bilirubin 17.2 (0.3–1.2mg/dL) and direct bilirubin 9.9 (0.1–0.5mg/dL) with normal amylase and lipase. Subsequent complementary studies showed no abnormalities, including tumour markers carcinoembryonic antigen and carbohydrate antigen 19-9, viral infections (coxsackie, hepatitis B, cytomegalovirus, varicella-zoster virus, herpes simplex virus, epstein–barr virus, human immunodeficiency virus), bacterial infections (mycoplasma, legionella, leptospira, coxiella burnetii, rickettsia conorii, treponema pallidum, borrelia burgdorferi), autoimmunity and serum IgG4.
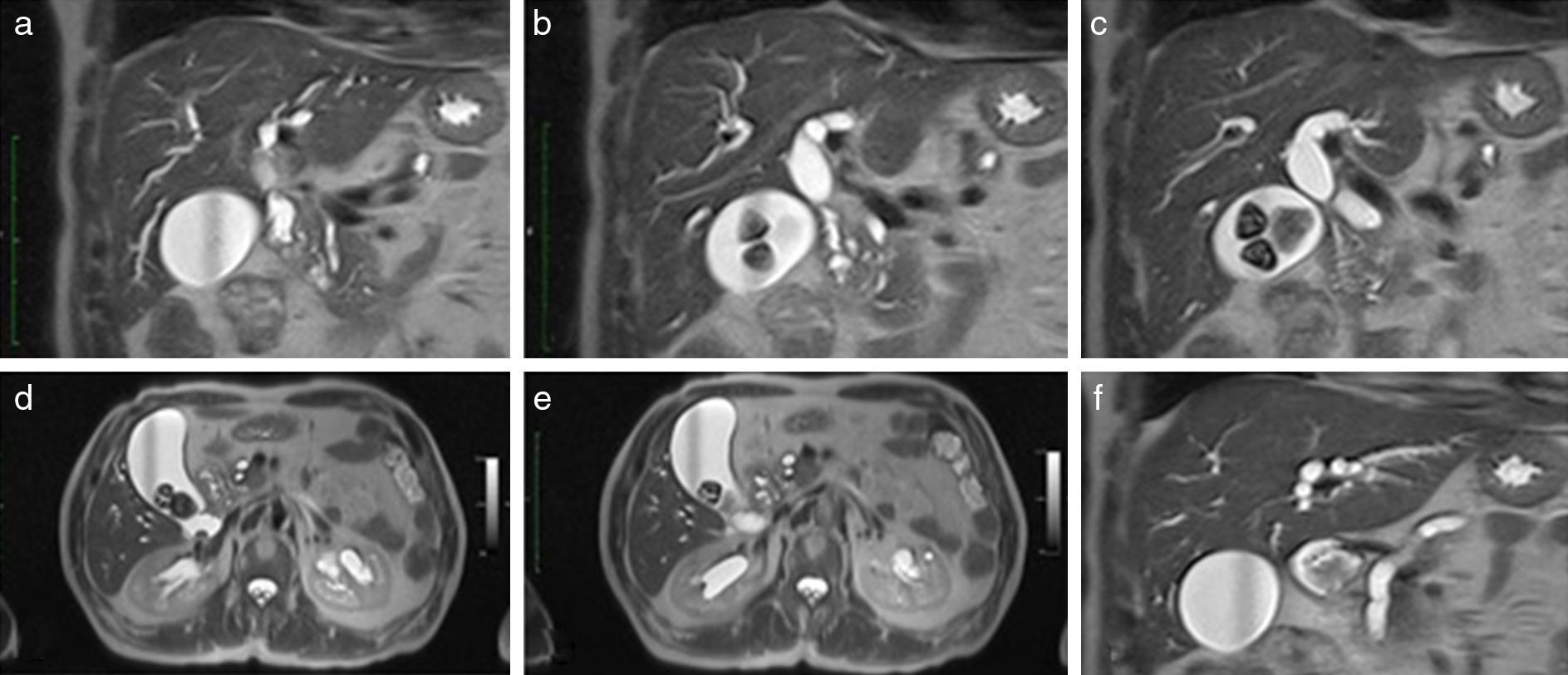
The abdominal ultrasound showed a dilatation of the intra-hepatic biliary ducts (IHBD), middle third of CBD (16mm) and Wirsung (7mm), with normal distal CBD diameter. Biliary lithiasis and pancreatic atrophy were also detected, but it was not possible to identify the obstructive cause. The abdominal computerized tomography and the magnetic-resonance cholangiopancreatography showed IHBD dilatation, dilatation of proximal third of CBD measuring 17mm with progressive distal narrowing, pancreas divisum, ectasia of the duct of Wirsung with maximum diameter of 8mm, atrophy of pancreatic body and tail and cystic structures in pancreaticoduodenal groove. These imagiological findings appeared to have been caused by a thick duodenal parietal wall at minor papilla level with consequent Wirsung obstruction and significant extrinsic compression of CBD which associated to the small cystic images in paraduodenal groove are strongly suggestive of groove pancreatitis (Fig. 1).
, pancreas divisum (a–c) and enlarged Wirsung (f).")
Subsequently, an esophagogastroduodenoscopy was performed, revealing an asymptomatic duodenal stricture with congestive and infiltrative mucosa, making a transpapillary approach by endoscopic retrograde cholangiopancreatography impossible. The biopsies showed moderate duodenitis without dysplasia or neoplasia.
Despite conservative treatment with bowel rest, fluid therapy, analgesics, proton pump inhibitors and pancreatic enzyme supplement, a persistent important cholestasis (total bilirubin ∼16mg/dL) and consequent obstructive jaundice occurred. After multidisciplinary consultation the patient was submitted to a Y-en-Roux cholangiojejunostomy and cholecystectomy. Surgical specimen showed chronic lithiasic cholecystitis, cholestatic hepatitis and CBD with no abnormalities.
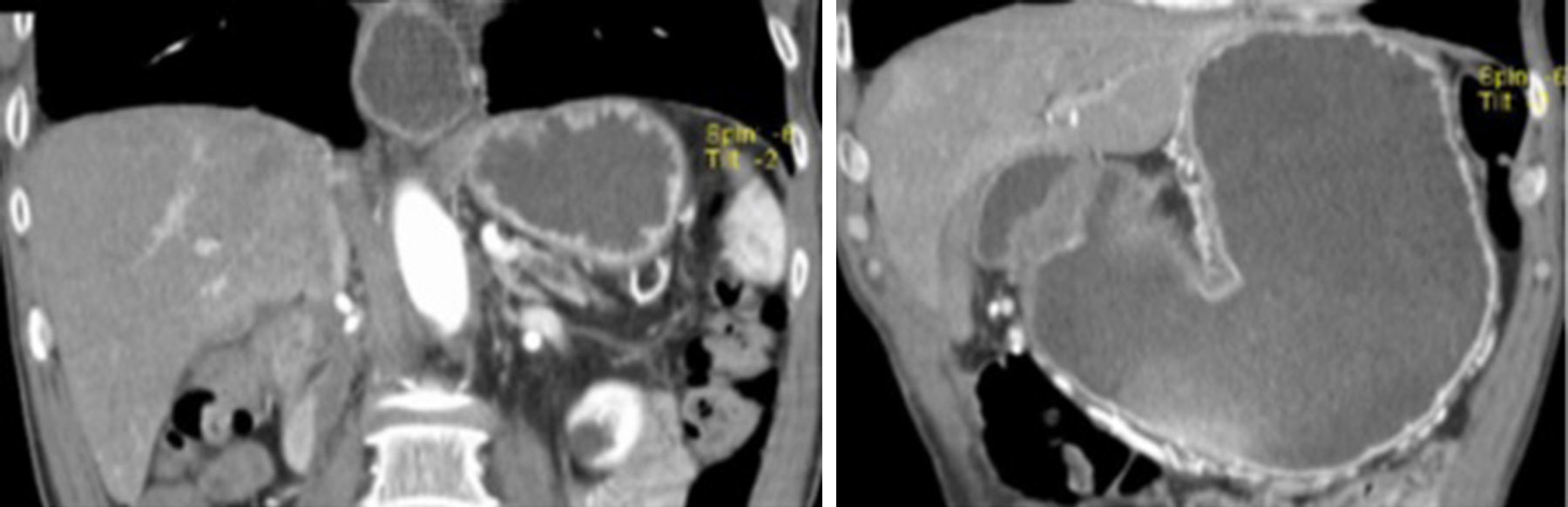
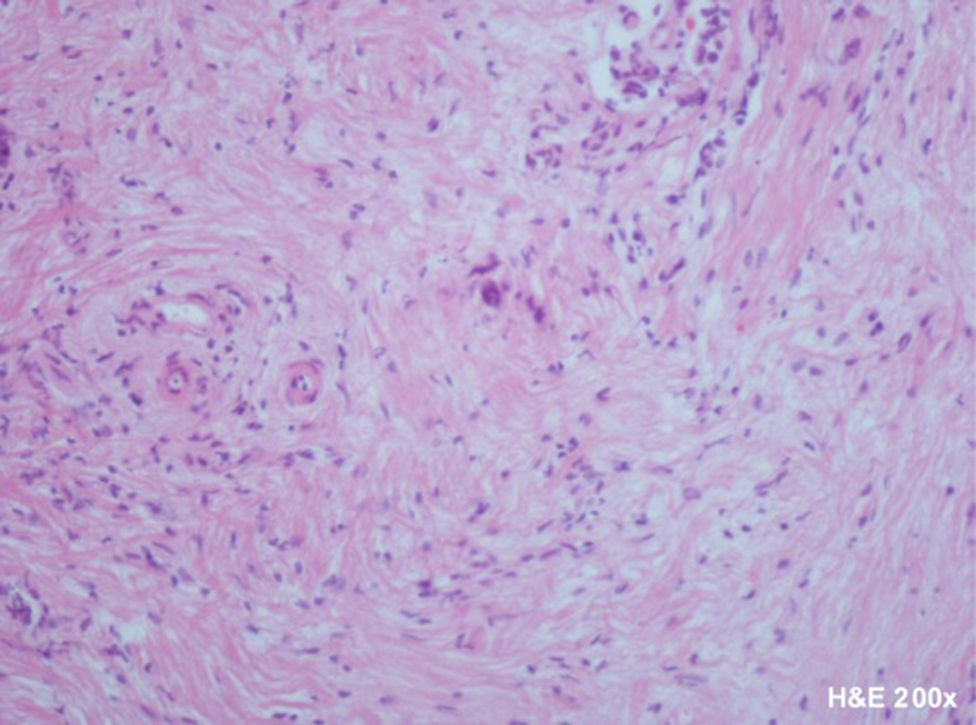
Five months after the surgical intervention, the patient returned to the emergency department due to recurrent vomiting and food intolerance. The ultrasound scan was normal in regards to IHDB and CBD. The plain abdominal X-ray and computerized tomography revealed marked oesophageal and gastric dilatation with stasis (Fig. 2). An esophagogastroduodenoscopy confirmed the presence of severe esophagitis in relation to the gastroesophageal reflux of gastric stasis content due to impassable duodenal stricture. Biopsies continued to show moderate duodenitis without dysplasia or neoplasia. The patient was treated with proton-pump inhibitors, antacids and prokinetics with no clinical improvement. It was then decided to submit the patient to a gastrojejunostomy. At the time of this surgical procedure an incisional biopsy of anterior and lower border of pancreas was also performed. Histopathology revealed chronic pancreatitis without dysplasia or neoplasia (Fig. 3). Presently, the patient is asymptomatic and is being followed up in an outpatient surgical clinic. The patient gave informed consent for all diagnostic and therapeutic procedures.


Groove pancreatitis is an uncommon subtype of focal chronic pancreatitis and a rare cause of obstructive jaundice. Only a very small number of cases have been published.1–3
The prevalence is underestimated, but in surgical case series groove pancreatitis was diagnosed in 2–24.5% of pancreaticoduodenectomy specimens of patients with chronic pancreatitis.4,7,8 This condition is often present in middle-aged males (40–50 years old) with alcohol consumption.1,7–9 The clinical presentation is similar to more prevalent forms of chronic pancreatitis, but recurrent vomiting due to duodenal stricture and impaired motility tends to be more frequent in groove pancreatitis.2 However, the majority of cases had a mild CBD dilatation, insufficient to cause obstructive jaundice.9
Laboratory analysis often reveals a normal or slight elevation of serum pancreatic enzymes and occasionally of serum liver enzymes.1,10 Tumour markers of carcinoembryonic antigen and carbohydrate antigen 19.9 are usually negative.1,8
The diagnosis is difficult to establish and involves clinical, radiological and histopathological features.1 The crucial differential diagnosis is a head pancreas adenocarcinoma, since the management and prognosis are different.1,2,9,11 Magnetic resonance is more sensible and specific to detect findings, the most common being a sheet-like mass between the pancreas head and duodenum with duodenal wall cystic changes and thickening.6,10
In the histopathology analysis, the macroscopic aspects are either an absent or narrow Santorini duct, or the presence of pancreas divisum and groove lesions similar to those of chronic pancreatitis.12,13 The duodenal wall contains enlarged ducts, in the majority of cases with thickened secretions, pseudocystic changes, adjacent stromal reactions and Brunner gland hyperplasia. Fibrosis into the adjacent pancreas and the surrounding fat occurs, especially in the groove area which involves the CBD.14
The pathogenesis is still unclear, but the most accepted mechanism is a disturbance of the pancreatic outflow in the Santorini duct through the minor papilla. One of the main factors is probably chronic alcohol consumption which increases the viscosity of the pancreatic juice and leads to Brunner gland hyperplasia, causing occlusion or dysfunction of the minor papilla.1,9,15,16
The treatment for acute phase of groove pancreatitis is conservative, including bowel rest, analgesia and fluids therapy.10 In the chronic stages of the process, fibrosis dominates over inflammation, and at this point surgical management could be necessary because of persistent biliary or duodenal stricture.17 The surgical treatment of choice is a Whipple procedure or a pylorus-preserving pancreaticoduodenectomy.4
In our case, a combination of clinical, radiological and pathology features was used to make a diagnosis of groove pancreatitis in a middle-aged male with history of alcohol consumption. Although rare, this condition should be part of differential diagnosis of obstructive jaundice and an extensive evaluation should be carried out to exclude pancreatic, duodenal or CBD neoplasia. This case was initially complicated by biliary stricture and later by duodenal stricture, with the option for a less-invasive surgical intervention after malignancy being excluded.
Conflicts of interestThe authors have no conflicts of interest to declare.
