




The obstruction of the common bile duct (CBD) by foreign body, followed by lithogenesis at that level, is uncommon and has been rarely referred in the literature. Sporadic reports have been published due to parasites, fish bones, fragments of T tubes or other rubber objects, shrapnel, metal clips, migrated stents, surgical gauze and non-absorbable suture material, which serve as a nucleus for formation of stones or molds in the bile duct.1–5
The previous reported cases with impacted surgical gauze in CBD had classical presentation of obstructive jaundice with radiological inconclusive investigations mimicking a common bile duct stone or malignant disease of the CBD.2–4
Endoscopic and surgical extraction of these bodies is mandatory, in order to avoid the complications of obstructive jaundice especially cholangitis and biliary sepsis.4,5
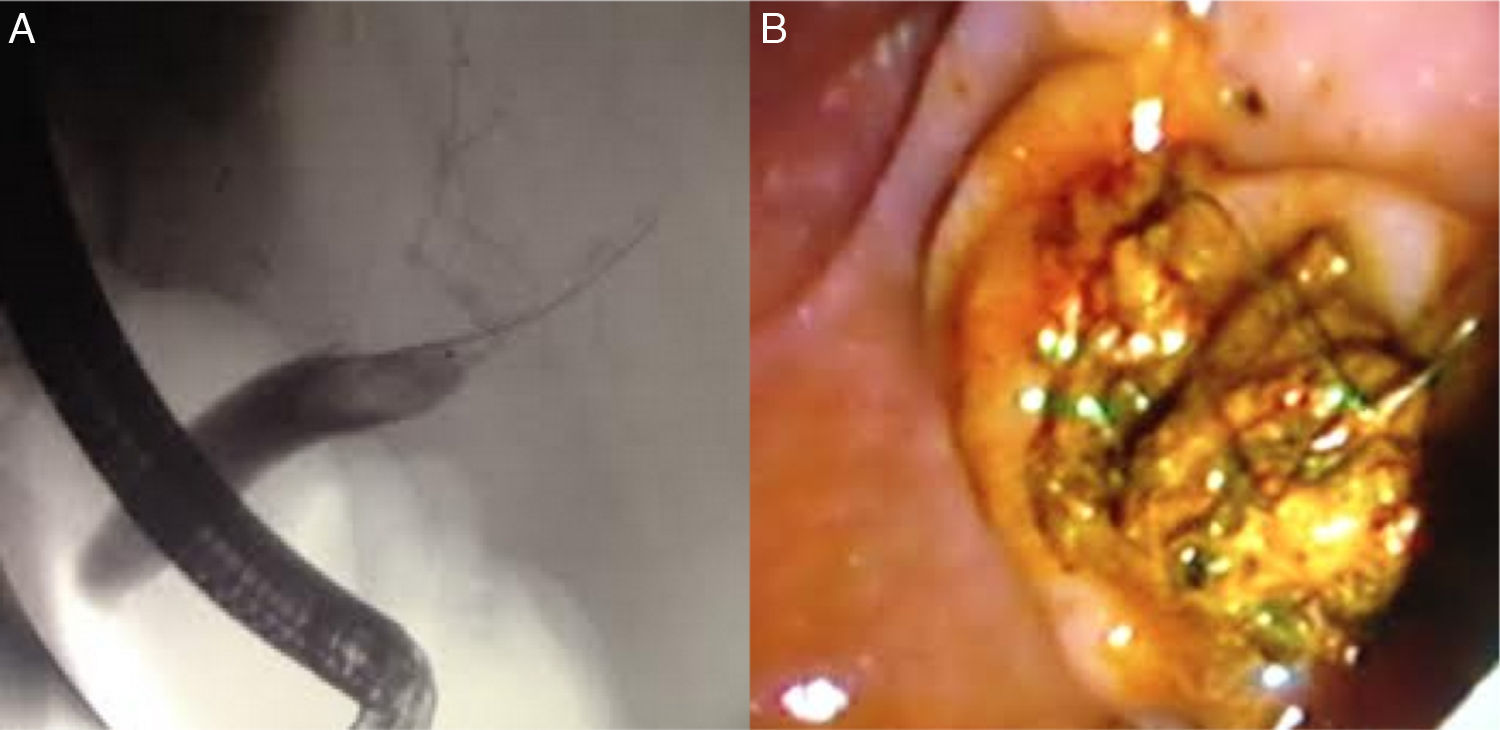
2Case descriptionA 69 year-old man, with a medical history of liver transplant in 2002 from liver cirrhosis due to hepatitis C, underwent liver retransplantation in 2014 by acquired familial amyloid polyneuropathy. Three months after the surgery the patient had progressive deterioration of the analytical hepatic enzymes with cholestasis (gamma glutamyl transpeptidase 1147U/L (<55); alkaline phosphatase 926U/L (40–150); total bilirubin 2.3mg/dL (0.3–1.2); direct bilirubin 1.7mg/dL (0.1–0.5); aspartate aminotransferase 58U/L (<35); alanine aminotransferase 56U/L (<45)), without fever, abdominal pain or increased inflammatory parameters. Ultrasonography of the abdomen showed moderate dilatation of the main bile duct (12mm) and could not define the cause of obstruction. Computed tomography was performed and revealed dilatation of the CBD (13mm) with a dense heterogeneous material inside in probable relationship to choledocholitiasis (Fig. 1). Endoscopic retrograde cholangiopancreatography showed an intracoledocal filling defect of 30mm (Fig. 2A). After sphincterotomy and with help of Dormia basket it was possible to extract an elongate 3cm in length biliary mold (Fig. 2B) whose macroscopic analysis showed the presence of compress fragments (Fig. 3). At discharge and several weeks later the repeated laboratory analysis revealed normalized liver function tests.

. After sphincterotomy and with help of Dormia basket it was possible to extract several small stones and an elongate biliary mold (B).")

The authors emphasize that bile duct obstruction by a foreign body is possible and can cause difficulties in diagnosis. It is therefore important to remember, when facing images suggesting giant stones, that the CBD may be obstructed by foreign body, especially in those patients who have previously undergone surgery.
Ethical disclosuresConfidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Protection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Conflicts of interestThe authors have no conflicts of interest to declare.
