



Endoscopic retrograde cholangiopancreatography (ERCP) in patients with surgically altered upper gastrointestinal anatomy such as a Roux-en-Y anastomosis is challenging. The use of balloon-assisted enteroscopy allows evaluation of the surgically excluded segment, access to the biliopancreatic tract and performance of endoscopic therapy.
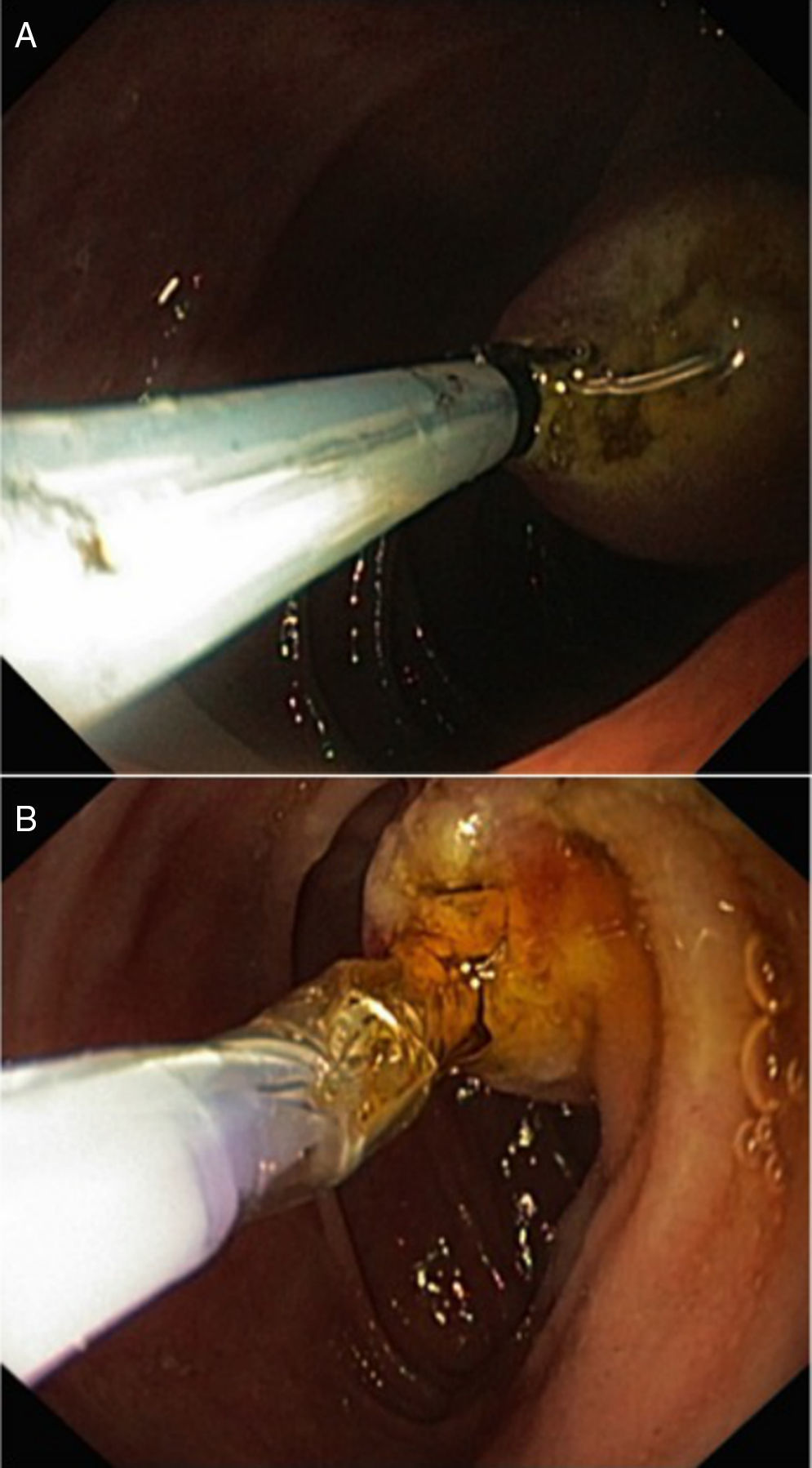
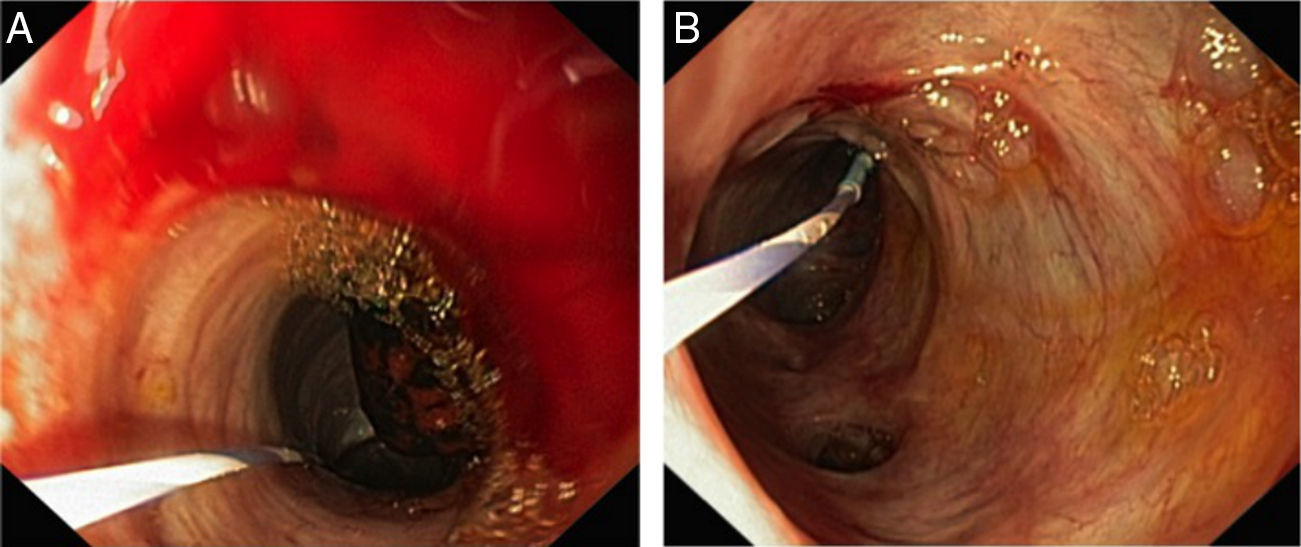
A 79-year-old female patient, with history of cholecistectomy (2005) and total gastrectomy with Roux-en-Y anastomosis for gastric cancer (pT2N0M0, 2007), suffered from recurrent episodes of cholangitis (2012). Abdominal ultrasonography revealed pronounced bile duct dilation (20mm) caused by a large gallstone (17mm) in the distal third of the common bile duct. After a failed standard ERCP, a percutaneous transhepatic biliary drainage (PTBD) was initially performed to relieve the obstruction. However, stone extraction was not accomplished. Therefore, she was referred to us for SBE-assisted ERCP, which was performed using a rendezvous technique, since there was a previously placed PTDB. The SBE (SIF-Q180 Olympus Medical Systems, Tokyo, Japan) was advanced to the afferent limb up to the papilla, where externalization of the percutaneously inserted guidewire was observed. A 4Fr catheter (0.038″ 65cm, Cordis) was placed over the wire and the percutaneous guidewire removed. A 500cm 0.0035′ guidewire (Endoflex 21535500, Germany) was placed percutaneously through the catheter and grasped with a standard polypectomy snare. Then, biliary cannulation over the guidewire using the rendezvous technique was performed. Only limited sphincterotomy was achievable, due to the use of a longer (280cm) conventional sphincterotome (Endoflex OE1042230DL-280, Germany) (Fig. 1). To safely perform a large sphincterotomy, a long Bilroth II-type sphincterome should be used, due to the retrograde approach. Subsequently, endoscopic papillary dilation was performed using a standard 12–15mm balloon (CRE Boston Scientific, Tokyo, Japan), under direct visualization and radiologic control (Fig. 2). Peroral direct cholangioscopy (PDCS) was possible with the enteroscope, owing to pronounced biliary dilation. The large bile duct stone was removed under direct visualization using a retrieval balloon (Fig. 3). Finally, residual gallstones were excluded by PDCS and PTDB cholangiogram. There were no procedure-related complications. The patient had an uneventful recovery, and remains stable after 2-year follow-up.
 and endoscopic papillary balloon dilation (B), performed via a retrograde approach.")

, which was subsequently removed under direct visualization using a retrieval balloon (B).")
Balloon-assisted enteroscopy–ERCP is now an accepted interventional modality in patients with complex postsurgical anatomy, such as Roux-en-Y anatomy.1 The enteroscope allows deep insertion into the small bowel and access to the papilla and the biliary tract. However, cannulation and sphincterotomy are technically difficult with a forward-viewing instrument, via retrograde approach. Additionally, the use of devices, such as dilating balloons, through a narrow and long working channel is limited. Also, the device maneuverability is difficult, particularly from looping and twisting scope position.2,3 A systematic review by Skinner et al. reported an overall ERCP success of approximately 74%, due to these limitations.4
Traditionally used in conventional ERCP, the rendezvous technique has improved the success rate of biliary cannulation in enteroscope-assisted ERCP. The SBE–ERCP rendezvous technique presented herein allowed successful therapeutic techniques such as sphincterotomy, papillary balloon dilation and biliary stone extraction, under direct endoscopic view. Our case, as other recent reports, illustrates the gradual disappearance of barriers for endoscopic biliary interventions in patients with altered upper gastrointestinal tract anatomy.5
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
