


Capsule retention is one of the known complications of capsule endoscopy.1 The risk of retention is high in patients with prolonged nonsteroidal anti-inflammatory drug use, extensive Crohn's Disease and previous major abdominal surgery.2 Most cases of capsule retention are asymptomatic and should be managed conservatively whenever possible. Some can be naturally excreted and other are amenable to medical therapy or endoscopic removal. Surgery is considered if the patient develops acute small bowel obstruction symptoms or the origin is a malignant lesion.3
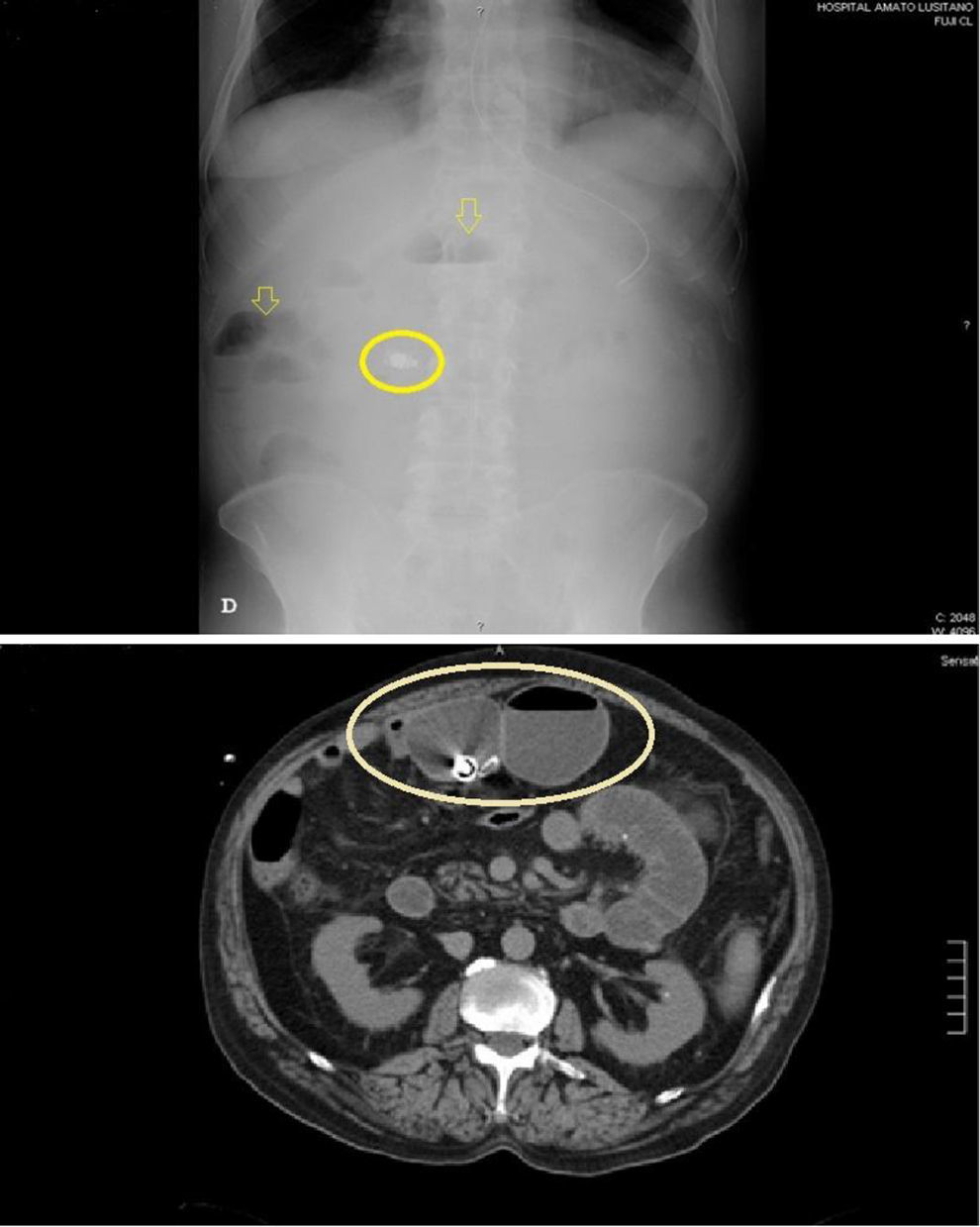
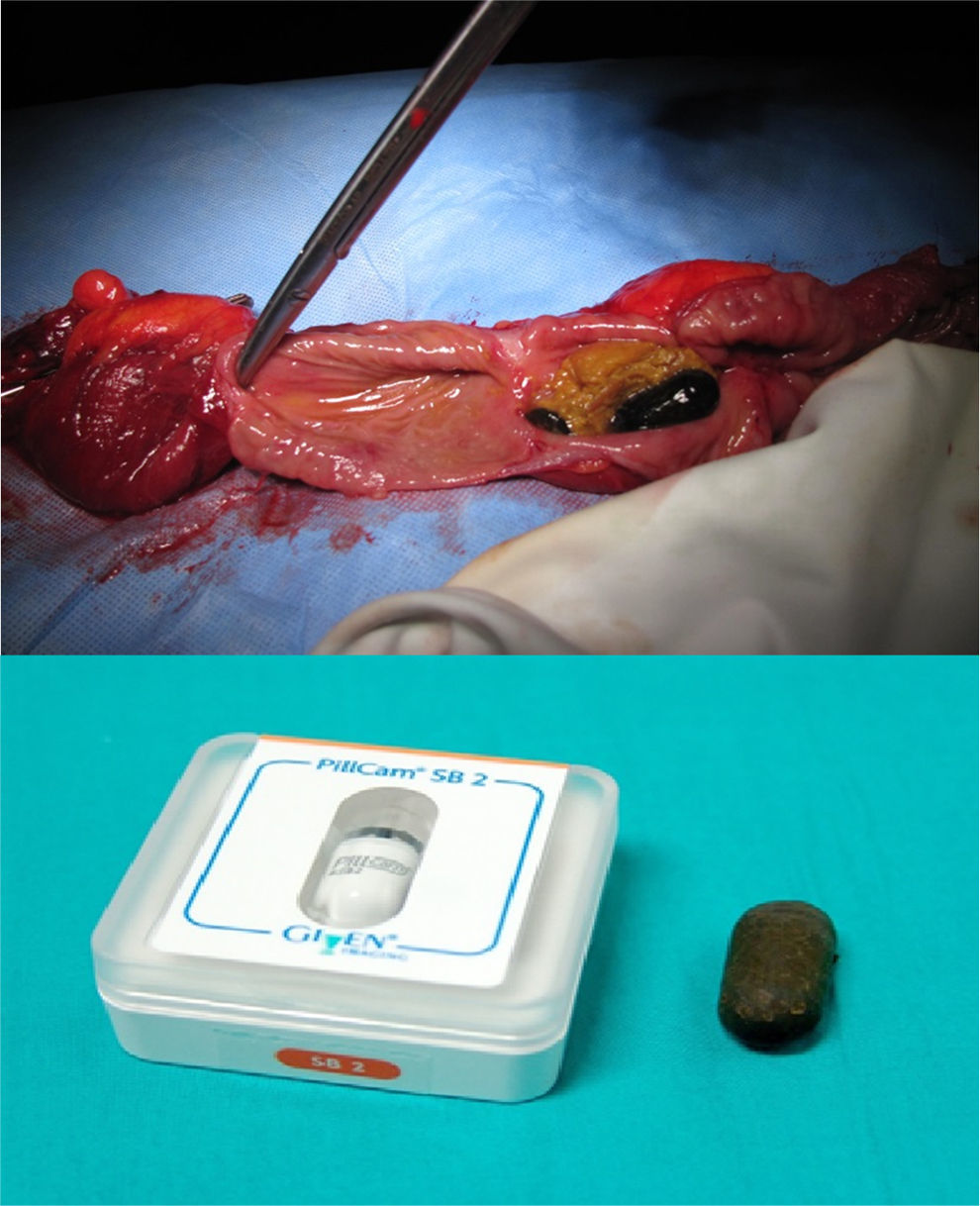
A 69-year-old man, hypertensive, was referred to the Gastroenterology Department to perform an upper endoscopy on November of 2012 because of diffuse abdominal pain and dark colored emesis. Blood workup was unremarkable, except for leukocytosis. The abdominal X-ray and computed tomography scan demonstrated small bowel distension and revealed a metallic foreign body of 20mm localized in the lumen (Fig. 1). Due to acute occlusive syndrome, patient was submitted to an exploratory laparotomy with resection of one segment of jejunum with 35cm and 4 inflammatory stenotic regions, one of them occluded by a cylindrical, black colored foreign body – an endoscopic capsule (Fig. 2)! The histologic result of the surgical specimen confirmed a small bowel diverticula and inflammatory strictures related to diverticulitis. During the review of patient's medical history we confirmed that he did not mention any digestive symptoms and he had a capsule endoscopy 7 years (on July of 2005) before during the workup of microcytic hypochromic anemia. The report of the capsule endoscopy did not mention blood in the lumen or mucosal changes, stressing that the capsule did not reach the cecum during the recorded time. However, there were not any signs/symptoms or past medical history at presentation (pre-capsule endoscopy) associated with a higher risk of capsule retention that could have advised the use of small bowel imaging or patency capsule in this patient. The authors also reviewed the capsule study confirming that no stenosis was identified. Interestingly, the patient did not remember any abdominal symptoms during the 7 years of capsule retention.


As far as we are aware this is the longest reported case of capsule retention,4 an unusual case of retained endoscopic capsule in a patient without any suspicion of stenosis of the intestine and which remained asymptomatic over 7 years.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
