



Pese a que la presencia de limitaciones significativas en conducta adaptativa constituye uno de los tres criterios necesarios para establecer un diagnóstico de discapacidad intelectual, su estructura siempre ha sido objeto de un polémico debate entre investigadores. El presente estudio tiene como objetivo respaldar resultados previos de investigación que proporcionan un mayor apoyo a una estructura multidimensional de habilidades conceptuales, sociales y prácticas frente a una estructura unidimensional. Mediante Análisis Factorial Confirmatorio (AFC) se analizaron modelos de un único factor y de 3 factores correlacionados, ambos representados por un conjunto de 15 indicadores observables, así como su posible relación con un factor de orden superior (i.e., conducta adaptativa). Para ello, se evaluó la conducta adaptativa de 388 niños con y sin discapacidad intelectual con la Escala de Diagnóstico de Conducta Adaptativa (DABS). Los resultados del AFC pusieron de manifiesto que el modelo de 3 factores de primer orden es el que presenta un mejor ajuste a los datos. La fiabilidad y validez del modelo multidimensional se analizaron además mediante otros métodos como la fiabilidad compuesta y la varianza media extractada. Finalmente se discuten las implicaciones que pudieran derivarse de estos resultados, así como futuras líneas de investigación.
Although the presence of significant limitations in adaptive behavior constitutes one of the three necessary criteria for diagnosing intellectual disability, adaptive behavior structure has always been the subject of considerable controversy among researchers. The main goal of this study is to extend previous research results that provide further support to a multidimensional structure of conceptual, social, and practical skills compared to the unidimensional structure. One-factor and 3-correlated factors models as measured by 15 observable indicators were analyzed by means of confirmatory factor analysis (CFA), as well as their relationships with one second-order factor (i.e., adaptive behavior). To that end, 388 children with and without intellectual disabilities were assessed with the Diagnostic Adaptive Behavior Scale (DABS). Results of CFA indicated that the 3 first-order factors solution provides the best fit to the data. Reliability and validity of the multidimensional model were also analyzed through different methods such as the composite reliability and the average variance extracted. Finally, implications of these findings and possible directions for future research are discussed.
Pagina nueva 1
Before the arrival of the intelligence tests movement, intellectual disability (ID) was described in terms of what we nowadays call adaptive behavior (Schalock, 1999; Schalock et al., 2010) or the ability to respond to environmental demands. Nonetheless, adaptive behavior skills ceased to play an important role in the conceptualization and diagnosis of ID in the first half of the 20th century due to the emphasis given to IQ scores. Adaptive behavior reemerged as one of the three diagnostic criteria of ID in the 5th edition of the American Association on Mental Deficiency in 1959. However, adaptive behavior structure has traditionally been the subject of considerable controversy, particularly among the scientific audience. In the 70's, 80's, and early 90's, two main approaches to the study of adaptive behavior structure emerged: the first one, argued that adaptive behavior is a unidimensional construct (e.g., Bruininks, McGrew, & Maruyama, 1988), while the second, consistently supported by research (see Widaman, Borthwick-Duffy, & Little, 1991), defended that adaptive behavior is multidimensional in nature.
In 1992 the American Association on Mental Retardation (AAMR) adopted a position in relation to both approaches and conceptualized ID according to a multidimensional framework that was also reflected in the way of understanding adaptive behavior, assuming that people with ID experience difficulties that result from the presence of significant limitations in different adaptive skills: communication, self-care, home living, social skills, community use, self-direction, health and safety, functional academics, leisure, and work. However, due to the lack of confirmatory factor analysis to validate the structure of these ten adaptive behavior areas, some authors criticized their artificial and arbitrary nature (Verdugo, 2003; Widaman & McGrew, 1996) while others pointed out the mistake of including adaptive behavior as a diagnostic criterion before there was an adequate theoretical understanding of it (Greenspan, 2012).
In response to adaptive behavior structure criticism, the construct was substantially modified, and the current conceptualization of ID (Luckasson et al., 2002; Schalock et al., 2010) defines it as a disability originated before age 18 and characterized by significant limitations both in intellectual functioning and in adaptive behavior.
Adaptive behavior is therefore considered on equal footing as intelligence and can be understood as the "collection of conceptual, social, and practical skills that have been learned and are performed by people in their everyday lives" (Luckasson et al., 2002, p. 17; Schalock et al., 2010, p. 15). This conceptualization of ID reflects the influence of Greenspan's ideas about tripartite intelligence (i.e., conceptual, social, and practical intelligence) (Greenspan, 2006), but it is necessary to point out some aspects regarding this model. On the one hand, although author's original intend was replace the dual criteria model of IQ and adaptive behavior by a broader concept of adaptive functioning or personal competence, the relationship between adaptive behavior and intelligence is not clear today as we can deduce from the large amount of empirical studies that are focused on it (e.g., Ditterline & Oakland, 2009; Kenworthy, Case, Harms, Martin, & Wallace, 2010; Matson, Rivett, Fodstad, Dempsey, & Boisjoli, 2009). On the other hand, although this model has become one of the most relevant approaches to understand the relationship between adaptive behavior and intelligence, it continues to be theoretical and needs more empirical work (Schalock et al., 2010; Tassé et al., 2012).
This tripartite conceptualization of adaptive behavior (i.e., conceptual, social, and practical skills) is based on different empirical studies that attempted to shed light on the structure of this construct (Harrison & Oackland, 2003; Harrison & Rainieri, 2008; Widaman et al., 1991; Widaman & McGrew, 1996). Most of these studies found support for the presence of four domains of adaptive behavior: conceptual, social, practical, and motor skills, but unlike previous definitions, physical or motor competence is not currently included within the adaptive behavior domain, considering that it should be measured within a separate domain of health due to its relation to developmental aspects (Luckasson et al., 2002; Schalock et al., 2010). Similarly, problem behaviors are not considered as part of the diagnosis of significant limitations in adaptive behavior. Firstly, there is a general agreement among scientists and clinicians that the presence of significant levels of behavior problems does not mean significant limitations in adaptive functioning (Luckasson et al., 2002; Schalock et al., 2010; Tassé, 2009). Secondly, although adaptive and maladaptive behaviors are moderate or strongly related in people who present a co-morbid condition (i.e., Autism Spectrum Disorder, ASD) (e.g., Kearny & Healy, 2011), these constructs are weakly related in people with ID and no other conditions (Tassé, 2009). Finally, problem behaviors are not critical issues for diagnosing ID whereas such behaviors may be the answer to inappropriate environments where people lack of alternative communication skills (Schalock, 1999). This conceptualization yields important clinical applications due to motor skills and behavior problems are no longer included in the diagnosis of ID, making possible a differential diagnosis between ID and, for example, developmental delays or mental health related problems. Likewise, the tripartite model of adaptive behavior (i.e., conceptual, social, and practical skills) allow clinicians to provide an accurate diagnosis of significant limitations in one of these skills or an overall score of all of them, once their correlation has been empirically verified.
Up to this time, approximately 200 adaptive behavior scales exist (Schalock, 1999). However, only four of them according to Schalock et al. (2010) and Tassé et al. (2012) are based on a 3-factor structure of adaptive behavior (i.e. conceptual, social, and practical skills) and have adequate evidences of reliability and validity, and have been standardized on people with and without ID: a) the Vineland Adaptive Behavior Scales-2nd edition (Sparrow, Cicchetti, & Balla, 2005); b) the Adaptive Behavior Assessment System-II (Harrison & Oakland, 2003); c) the Scales of Independent Behavior-Revised (Bruininks, Woodcock, Weatherman, & Hill, 1996); and d) the Adaptive Behavior Scale-School Version (Lambert, Nihira, & Leland, 1993). It is important to note that none of these measures are available in Spanish and, therefore, none of the instruments currently used in our context relies on the aforementioned structure of adaptive behavior.
Due to these measures are not exclusively focused on diagnosing, the American Association on Intellectual and Developmental Disabilities (AAIDD), formerly known as AAMR, has developed the forthcoming Diagnostic Adaptive Behavior Scale, DABS (Tassé et al., in press), which has been designed to be consistent with the tripartite model of adaptive behavior. Item Response Theory (IRT) has been used in its development to reliably measure individual levels of performance across the continuum of adaptive skills and ages (4-8 years old; 9-15 years old; and 16-21 years old). This measure will also been published in Spanish (Verdugo, Arias, & Navas, in press) and it has been developed following the development process by the AAIDD (Navas, Verdugo, Arias, & Gómez, 2010, 2012). The Partial Credit Model (Masters, 1982) was chosen to analyze items' and persons' functioning with the goal of selecting those items that will contribute to develop a short and precise instrument measuring a single latent trait (i.e., significant limitations in adaptive behavior), which should be enough to explain people's performance. Principal Component Analysis (PCA) on residual scores, and parallel analysis with 1,000 replications by performing a Monte Carlo simulation were carried out, offering support for the unidimensionality of the DABS (Navas et al., 2012).
This paper describes an instrumental or empirical study (Gómez, Verdugo, Arias, & Crespo, 2010) focused on examining the factor structure of adaptive behavior as measured by the Spanish version of the DABS Form 4-8 years old by means of Confirmatory Factor Analysis (CFA). Three factor solutions are defined and tested against each other in this paper: a) adaptive behavior is a unidimensional construct; b) adaptive behavior consists of 3-correlated factors (i.e., conceptual, social, and practical skills); and c) adaptive behavior consists of 3 first-order factors (i.e., conceptual, social, and practical skills) and one second-order factor (i.e., adaptive behavior).
Method
Participants
The development of the Diagnostic Adaptive Behavior Scale (DABS) in Spain has involved the participation of 173 interviewers and 773 respondents filling in the Spanish version of the DABS for 1,047 people with and without ID between 4 and 21 years old. Having people without ID in the sample will be essential to compute the within-age means and standard deviations of the subscales (i.e., conceptual, social, and practical skills), while having people with ID can help the researcher to reliably select those items measuring lower levels of adaptive behavior to make an accurate diagnosis of ID.
Specifically, the sample aged 4 to 8 years old (M = 5.88; SD = 1.37) was comprised of 388 people with (n = 164) and without (n = 224) ID. Related to their main socio-demographic characteristics, 61.5% were male. All of them had already been diagnosed as having profound (n = 11), severe (n = 40), moderate (n = 46), or mild (n = 67) intellectual disability. The school psychologist of each center provided data regarding the diagnosis of ID. Most of the assessments were based on intelligence measures such as the Wechsler Intelligence Scale for Children (Wechsler, 2005). However, only 32 people had an assessment of their adaptive behavior, and in these cases the Inventory for Client and Agency Planning (ICAP) was used (Montero, 1993) and its aim is not diagnosis, but rather services planning and program evaluation. This fact emphasizes the need of an assessment instrument like the DABS.
Instrument
The DABS Form 4-8 years old is administered via a face-to-face interview for the purpose of ruling-in or ruling-out a diagnosis of ID, and is divided into three subscales which are focused on the measurement of conceptual (i.e., language, reading and writing, money use, self-direction, time, numbers/measures, and problem-solving), practical (i.e., activities of daily living, safety, healthcare, schedules/ routines), and social skills (i.e, interpersonal relationships, responsibility, self-esteem, wariness, naïveté, follows rules/obeys laws, manners, and social problem solving). The DABS assesses individual's typical performance during daily routines and changing circumstances. Adaptive behavior skills are measured according to a four-point Likert scale from 0 (rarely or never does it) to 3 (does it always or almost always independently).
With the aim of developing the shortest possible and most precise measure (i.e., 75 items, Appendix 1), item selection was carried out by means of Item Response Theory (IRT) within subscales so that the final instrument were as balanced as possible (i.e., 25 items per each subscale). Items' and persons' functioning were analyzed with the goal of selecting those items that provide the most accurate information around the cut-off point for determining significant limitations in adaptive behavior (see Navas et al., 2012).
Procedure
Most of the children (73.78%) were recruited from ordinary schools across 11 Spanish provinces. The DABS administration procedure consisted of a face-to-face interview (carried out by qualified and trained professionals) with one or more people who knew the person assessed very well (i.e., at least during the last 6 months), and who have had the opportunity to observe his or her behavior in a variety of settings. Due to sample characteristics (i.e., people under the age of 18), it was necessary to request for authorization to conduct the research to the University of Salamanca Ethics Committee. Once it was submitted and approved, we requested also for authorization to parents or legal guardians to conduct the adaptive behavior assessment.
CFAs were conducted using LISREL version 8.8 (Jöreskog & Sorbom, 2006). The first steps in this process were model specification and model identification by means of stating the hypotheses to be tested and statistically identifying the model. Based on the recommendations of Hu and Bentler (1999), model fit was evaluated using a combination of absolute and incremental goodness of fit indices.
Results
Model specification and identification
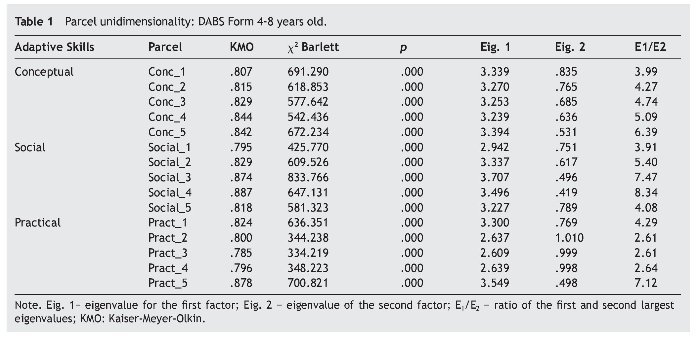
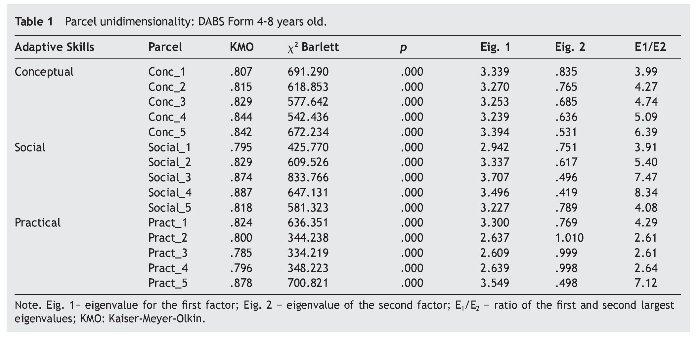
Model specification involves using all the available relevant theory with regard to adaptive behavior to specify and explain the variation and covariation in a set of observed variables (i.e., items) in terms of a set of underlying traits (i.e., conceptual, social, and practical skills). To reduce model complexity (i.e., the DABS is composed of 75 items), parcels were used as indicators of the latent constructs by combining individual items and using them as the observed variables. Although the use of parcels remains a controversial practice (see Little, Cunningham, Shahar, & Widaman, 2002), parcel scores have many advantages. On the one hand, parcels are closer to multivariate normality than the original set of item scores, making easier Maximum Likelihood (ML) estimation procedures (Bandalos, 2002; Jackson, Gillapsy, & Purc-Stephenson, 2009). However, item parceling should only be carried out if a clearly defined unidimensional structure has been indentified for a measure (Bandalos & Finney, 2001; Little et al., 2002). Parcels are considered approximately unidimensional if the eigenvalue for the first factor is large relative to the eigenvalue of the second factor (Reise, Moore, & Haviland, 2010) and if the ratio of the first and second largest eigenvalues is greater than 2.5 (Hall, Snell, & Singer Foust, 1999). Weighing the pros and cons of parceling, 5 parcels were constructed within each subscale (i.e., conceptual, practical, and social skills). Each parcel was composed of 5 items. The method of item parceling was to create parcels of items with opposite skew (Temperaal, Schim, & Gijselaers, 2007), a recommended practice with continuous or ordered categorical items (Holt, 2004).
Three models were tested against each other: a) adaptive behavior is a unidimensional construct (Model 1); b) adaptive behavior consists of 3-correlated and underlying traits (i.e., conceptual, social, and practical skills), each one measured by 5 observed variables or parcels (Model 2); and c) adaptive behavior consists of 3 first-order factors (i.e., conceptual, social, and practical skills) each one measured by 5 indicators, and one second-order factor (i.e., adaptive behavior) (Model 3).
Each parcel complied with the condition of unidimensionality (see Table 1). Kaiser-Meyer-Olkin (KMO) index and Bartlett's test of sphericity were also examined. KMO results greater than .80 and levels of significance lower than .001 indicated the appropriateness of conducting CFA. In three cases (parcels Social_1, Pract_3, and Pract_4), KMO indices were less than .80, however they were pretty close to an acceptable value (.795, .785, and .796, respectively). The ratio of the first and second largest eigenvalues was greater than 2.5 in all cases.
Given that a required condition for a model to be estimated is that there are more observations than parameters to be estimated (Mueller & Hancock, 2008), measured variables were identified. This yields to three over identified models (Models 1, 2, and 3) with 90, 87, and 88 degrees of freedom (df), respectively.
Parameter estimation and model fit
Due to ML estimation method assumes a multivariate normality of the data, normality indicators were examined by means of a joint test of skewness and kurtosis. Skewness values higher than |2.00| are described as "extremely" skewed, and values lower than |2.00| indicate that the distribution is peaked relative to the normal (Bandalos & Finney, 2010), while kurtosis values between |8.00| and |20.00| indicate extreme kurtosis (Arias, 2008; Kline, 2010). Skewness values ranged from -.950 to -.136, while kurtosis values ranged from -1.398 to .40, suggesting no severe deviations from normality.
The variance-covariance matrix was obtained in order to analyze the standardized estimates. The t-value associated with each of the standardized solutions exceeded the critical value (2.58) at p < .01 significance level. Is thereby deduced that the observed variables are reliable indicators of the latent traits.
Model fit (i.e., difference between the sample variance-covariance matrix and the estimated variance-covariance matrix) was assessed by means of both, absolute and incremental goodness-of-fit indices (Arias, 2008; Hu & Bentler, 1999; Gorostiaga, Balluerka, Aritzeta, Haranburu, & Alonso-Arbiol, 2011; Kline, 2010; Verdugo, Arias, Gómez, & Schalock, 2010): a) the chi-square test, χ2; b) the Root Mean Square Error of Approximation (RMSEA); c) the Tucker-Lewis Index (TLI); d) the Comparative Fit Index (CFI); and e) the Standardized Root Mean Square Residual (SRMR). Model fit is indicated by smaller values of χ2 (being no significant levels desirable); TLI and CFI values above .95; SRMR values less than .08; and RMSEA values less than .05 representing reasonable fit (Browne & Cudeck, 1993).
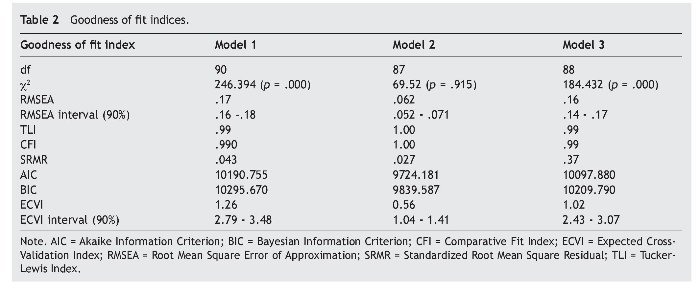
Regarding chi-square analysis, several authors recommend to examine the magnitude of c2 rather than its level of significance (Barrett, 2007; Flora & Curran, 2004; Hu & Bentler, 1999; Iacobucci, 2010; Kline, 2010), In this sense, different corrections have been made for structural equation models so data more closely approximate the chi-square distribution such as the Satorra-Bentler (SB) scaled chi-square (Satorra & Bentler, 2010), which was used for assessing model fit. Table 2 presents the results of SB chi-square and the aforementioned indices for the three models tested.
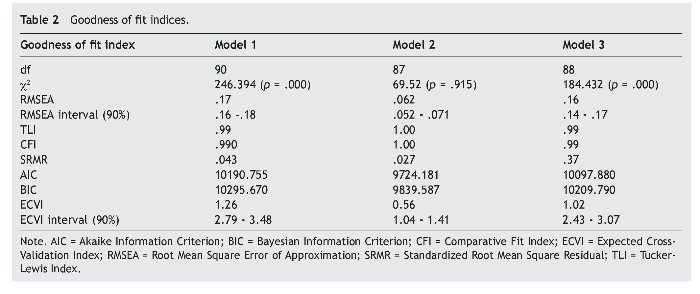
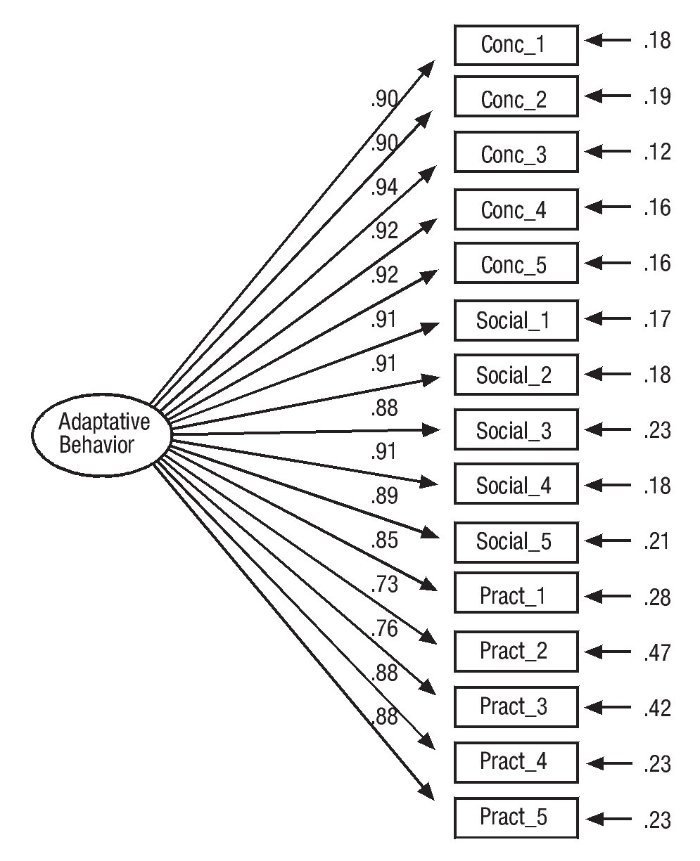
First, the unidimensional or one-factor model (i.e., one latent variable) was tested (see Fig. 1). Measurement errors ranged between .12 (parcel Conc_3) and .47 (parcel Pract_2), so is thereby deduced that the squared multiple correlation coefficients or coefficients of determination (R2) ranged from .88 to .53 (i.e., 1 minus the unexplained variance or measurements errors). All the factor loadings had values greater than .50. While SRMR values and TLI and CFI indices indicate a possible fit (SRMR = .04; CFI = .99; TLI = .99), chi-square analyses, and RMSEA values were far from acceptable: χ2 90 = 246.39, p < .001; and RMSEA = .17.
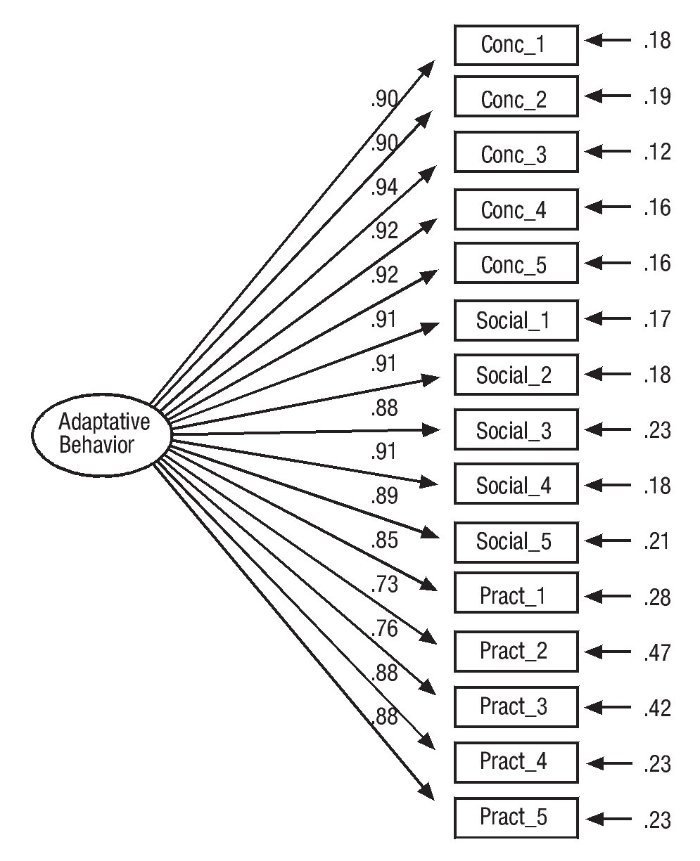
Figure 1 Model 1 (unidimensional). Standardized solution.
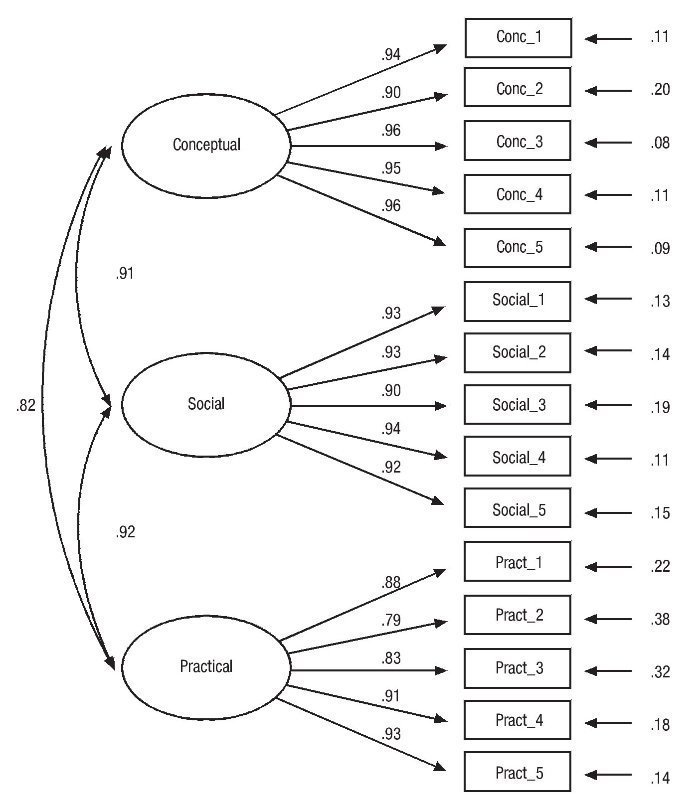
The second model (i.e., adaptive behavior consists of three correlated factors: conceptual, social, and practical skills), hypothesized to provide the best fit to the data, was then evaluated (see Figure 2). Measurement errors ranged between .08 and .38. The amount of variance explained by the latent traits ranged between .92 and .62. All the factor loadings had values greater than .50. Satorra-Bentler chi-square index verified the null hypothesis (χ2 87 = 69.52 p < .915) and all relative fit indices indicated that the three-factor solution provided a good fit to the data: RMSEA = .062, SRMR = .02, CFI = 1.00, and TLI= 1.00.
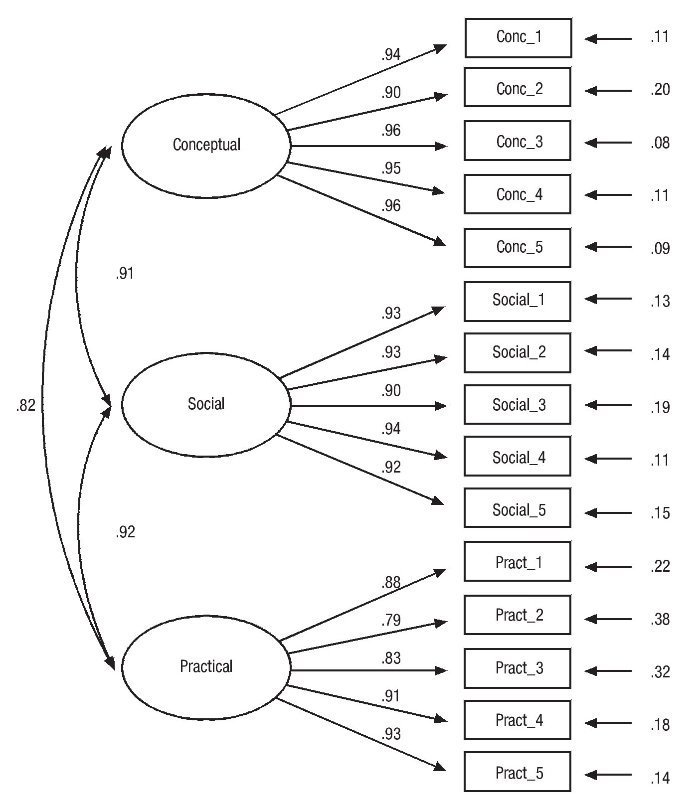
Figure 2 Model 2 (3-correlated factors). Standardized solution.
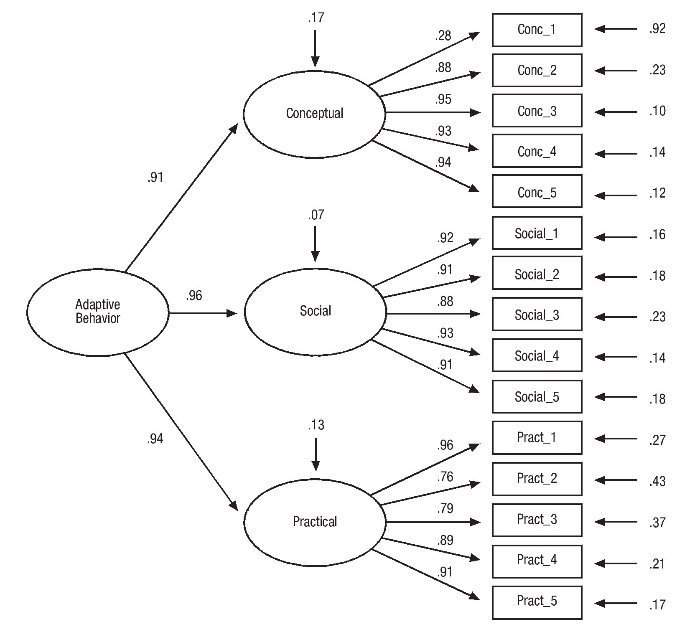
Finally, a hierarchical model was evaluated (see Figure 3) in which conceptual, social, and practical first-order factors were each measured by five indicators, with these first-order factors all loading onto one higher-order factor (i.e., adaptive behavior). Measurement errors ranged between .10 and .92, so R2 values ranged between .90 and .08, with only one factor loading lower than .50 (i.e., Conc_1). Results indicated a poor fit to the data, as the CFI and TLI were the only fit indices indicating good model fit: χ2 88 = 184.43 p < .001; RMSEA = .16; SRMR = .37; CFI = .99; and TLI = .99.
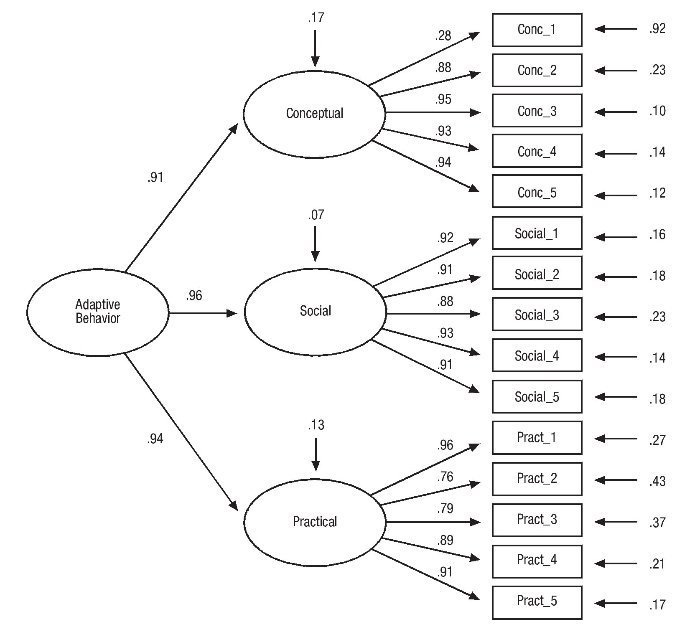
Figure 3 Model 3 (hierarchical). Standardized solution.
Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were also calculated for the three models tested. These comparative measures of fit are meaningful when different models are estimated, indicating lower values a better fit. Lowest AIC and BIC values were obtained for Model 2 (see Table 2). Furthermore, Expected Cross-Validation Index (ECVI) was computed, which has been defined as a measure of the distance between the fitted and expected covariance matrix (Jorëskog & Sörbom, 2006). Lowest ECVI values were obtained for Model 2, indicating a greatest potential for replication (Byrne, 2001).
Reliability and validity of the multidimensional model
With the aim of analyzing the internal consistency of Model 2 (i.e., adaptive behavior consists of three correlated factors: conceptual, social, and practical skills), and in addition to the reliability provided by R2 as a measure of the latent construct (Bollen, 2002), we calculated the composite reliability (rc) and the average variance extracted (rv) for each one of the latent constructs. Composite reliability is also called 'construct reliability' (Arias, 2008) and, similarly to Cronbach's a coefficient, indicates the overall reliability of a collection of heterogeneous but similar items within underlying traits. Values greater than .70 indicate that indicators are a reliable measure of the latent variable. The average variance extracted (rv) for each one of the latent constructs indicates how accurately the construct is measured (i.e., validity). Values should be greater than .50 (Hair, Ringle, & Sarstedt, 2011).
Both indices were in an acceptable range. Composite reliability values ranged from .792 (i.e., practical skills) to .889 (i.e., conceptual skills), while rv values ranged from .768 (i.e., practical skills) to .883 (i.e., conceptual skills), providing further support to the internal consistency of Model 2.
Discussion
The adoption of new approaches to the study of ID has highlighted the need for multidimensional classification systems based on the particular needs and circumstances of each individual. Although achieving a consensus on diagnostic instruments that have to be used in daily practice is not an easy task, it is essential to ensure at least instrument validity and reliability for the assessment process (Schalock et al., 2010).
Previous research indicates that significant limitations in adaptive functioning are a necessary (although not sufficient) diagnostic criterion for ID. This paper has aimed to extend previous studies (Widaman & McGrew, 1996; Widaman et al., 1991) by providing evidence about the appropriateness of a multidimensional structure of adaptive behavior (i.e., conceptual, social, and practical skills) as measured by the forthcoming Diagnostic Adaptive Behavior Scale (Tassé et al., in press). The use of parcels as indicators of latent constructs could be considered as a limitation of this study. However, once unidimensionality was guaranteed, item parceling was considered appropriate due to adaptive behavior was measuring by a multi-item scale. Another limitation that should be pointed out refers to multicollinearity or the high correlations among predictor variables. To determine the degree of multicollinearity, we computed the variance inflation factor (VIF) for each independent variable. Large VIF values are an indicator of multicollinearity. VIF values did not exceed the value of 10, which is often regarded as indicating severe multicollinearity.
Despite these limitations, and following the guidelines proposed by Hartley (2012), the three main conclusions that can be drawn form this study can be summarized as follows: a) the results of CFA studies indicated that the three correlated factors model provided a good fit when indicators (i.e., parcels) were extracted from the DABS, as evidenced by all relative fit indices (i.e., CFI, TLI, RMSEA, SRMR) meeting fit criteria and SB chi-square index; b) the reliability of each parcel (R2), as well as composite reliability and average variance extracted, indicated that conceptual, social, and practical skills are by themselves valid and reliable factors, without needing to turn to hierarchical models; c) these results have important implications if we take into account that current conceptions of significant limitations in adaptive behavior include a performance that is approximately two standard deviations below the mean of either i) one of the following three types of adaptive skills: conceptual, social, or practical, or ii) an overall score on a standardized measure of adaptive behavior (Luckasson et al., 2002; Schalock et al., 2010). Therefore, the presence of significant limitations in conceptual, social, or practical skills could be interpreted as a reliable evidence of the possible existence of significant limitations in adaptive behavior for the diagnosis of ID. We would like to remark possible because adaptive behavior assessment should rely on other aspects like clinical judgment and cultural and contextual considerations (i.e., Has the individual opportunities to perform adaptive skills in typical environments? Did the assessment take into account individual's cultural context? Has the person been rated with assistive technologies in place? Has the individual's adaptive skill been compared with his or her peers of the same chronological age?)
Finally, it is necessary to point out that although the DABS can be a useful measure as indicated by evidences of validity based on its internal structure, research about significant limitations in adaptive behavior should be continued by providing more evidences about different types of reliability. In this regard, although we would have liked to obtain other evidences of construct validity by applying different adaptive behavior measures, people assessed had no other adaptive behavior assessment, and no other measures with similar characteristics have been developed in our country. This fact demonstrates that, at least in our country, psychologists still have an excessive reliance on IQ measures, and also stresses the relevance of having an adaptive behavior diagnostic instrument with adequate psychometric properties like the DABS, which would help clinicians to avoid false negatives and false positives when diagnosing.
It would also be necessary to continue the research about the relationship between significant limitations in adaptive behavior and significant limitations in intellectual functioning to provide support or maybe refute theoretical models based on the concept of Personal Competence (Greenspan, 2006, 2012), which support the idea of setting aside the dual criteria model of IQ and adaptive behavior by a broader and single concept that will include both kind of limitations.
Funding
This project has been founded by the Ministry of Science and Innovation, MICINN (R&D Projects, 2009) (PSI2009-10953). It has been partially supported by a grant (EDU/894/2009) given to the Excellence Group of Research (GR197) by the Junta de Castilla y León (Spain).
*Corresponding author at:
Universidad of Valladolid, Campus Miguel Delibes, FEYTS,
Paseo de Belén 1, 47011 Valladolid, Spain.
E-mail address:barias@psi.uva.es (B. Arias).
Received December 20, 2012;
accepted March 20, 2013
References
Arias, B. (2008). Desarrollo de un ejemplo de análisis factorial confirmatorio con LISREL, AMOS y SAS. In M. A. Verdugo, M. Crespo, M. Badia, & B. Arias (Eds.), Metodología en la investigación sobre discapacidad. Introducción al uso de lasecuaciones estructurales (pp. 75-120). Salamanca: INICO.
Bandalos, D., & Finney, J. S. (2001). Item parceling in structural equation modeling. In G. A. Marcoulides, & R. Schumacker (Eds.), New developments and techniques instructural equation modeling (pp. 269-295). Mahwah, NJ: Earlbaum.
Bandalos, D.L. (2002). The effects of item parceling on goodness-of-fit and parameter estimate bias in structural equation modeling. Structural Equation Modeling, 9, 78-102.
Bandalos, D.L., & Finney, S. J. (2010). Factor analysis: Exploratory and confirmatory. In G. R. Hancock, & R. O. Mueller (Eds.), The reviewer's guide to quantitative methods in the social sciences (pp. 125-155). Florence, KY: Routledge Education.
Barrett, P. (2007). Structural equation modeling: Adjudging model fit. Personality and Individual Differences, 42, 815-824.
Bollen, K. A. (2002). Latent variables in psychology and the social sciences. Annual Review of Psychology, 53, 605-634.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen, & J. S. Long (Eds.), Testing structural equation models (pp. 136-162). Newbury Park, CA: Sage.
Bruininks, R. H., McGrew, K., & Maruyama, G. (1988). Structure of adaptive behavior in samples with and without mental retardation. American Journal on MentalRetardation, 93, 265-272.
Bruininks, R. H., Woodcock, R., Weatherman, R., & Hill, B. K. (1996). Scales of Independent Behaviour-Revised. Park Allen, TX: DLM Teaching Resources.
Byrne, B. M. (2001). Structural Equation Modeling with AMOS: Basic concepts, applications, and programming. Mahwah, NJ: Lawrence Erlbaum Associates.
Ditterline, J., & Oakland, T. (2009). Relationships between adaptive behavior and impairment. In S. Goldstein, & J. Naglieri (Eds.), Assessing impairment: From theory to practice (pp. 31-48). New York, NY: Springer.
Flora, D. B., & Curran, P. J. (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9, 466-491.
Gómez, L. E., Verdugo, M. A., Arias, B., & Crespo, M. (2010). Normas, sugerencias y recomendaciones para la publicación de artículos en ciencias sociales. Siglo Cero, 41, 38-58.
Gorostiaga, A., Balluerka, N., Aritzeta, A., Haranburu, M., & Alonso-Arbiol, I. (2011). Measuring perceived emotional intelligence in adolescent population: Validation of the Short Trait Meta-Mood Scale (TMMS-23). International Journal of Clinical and Health Psychology, 11, 523-537.
Greenspan, S. (2006). Functional concepts in mental retardation: Finding the natural essence of an artificial category. Exceptionality, 14, 205-224.
Greenspan, S. (2012). How do we know when it's raining out? Why existing conceptions of intellectual disability are all (or mostly) wet. Psychology in Intellectual and Developmental Disabilities, 37, 4-8.
Hair, C., Ringle, C. M., & Sarstedt, M. (2011). PLS-SEM: Indeed a silver bullet. Journal of Marketing Theory and Practice, 19, 139-151.
Hall, R. J., Snell, A. F., & Singer Foust, M. (1999). Item parceling strategies in SEM: Investigating the subtle effects of unmodeled secondary constructs. Organizational Research Methods, 2, 233-256.
Harrison, P. L., & Oakland, T. (2003). Adaptive behavior assessment system - Second Edition. San Antonio, TX: Harcourt Assessment.
Harrison, P. L., & Raineri, G. (2008). Best practices in the assessment of adaptive behaviour. In A. Thomas, & J. Grimes (Eds.), Best practices in school psychology (5th ed.) (pp. 605-616). Bethesda, MD: NASP Press.
Hartley, J. (2012). New ways of making academic articles easier to read. International Journal of Clinical and Health Psychology, 12, 143-160.
Holt, J. K. (2004, October). Item parceling in structural equation models for optimum solutions. Paper presented at the 2004 Annual Meeting of the Mid-Western Educational Research Association, Columbus, OH.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-55.
Iacobucci, D. (2010). Structural equations modeling: Fit indices, sample size, and advanced topics. Journal of Consumer Psychology, 20, 90-98.
Jackson, D. L., Gillaspy, A. R., & Purc-Stephenson, R. (2009). Reporting practices in confirmatory factor analysis: An overview and some recommendations. Psychological Methods, 14(1), 6-23.
Jöreskog, K. G., & Sorbom, D. (2006). LISREL: Interactive LISREL: Technical support (Version 8.8) [Computer software]. Lincolnwood, IL: Scientific Software.
Kearny, D. S., & Healy, O. (2011). Investigating the relationship between challenging behavior, co-morbid psychopathology and social skills in adults with moderate to severe intellectual disabilities in Ireland. Research in Developmental Disabilities, 32, 1556-1563.
Kenworthy, L., Case, L., Harms, M. B., Martin, A., & Wallace, G. L. (2010). Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 40, 416-423.
Kline, R. B. (2010). Principles and practices of structural equation modeling (3rd ed.). New York: The Guilford Press.
Lambert, N., Nihira, K., & Leland, H. (1993). AAMR Adaptive Behavior Scales-School (ABS-S:2). Examiner's Manual (2th ed.). Austin, TX: Pro-Ed.
Little, T. D., Cunningham, W. A., Shahar, G., & Widaman K. F. (2002). To parcel or not to parcel: Exploring the question, weighing the merits. Structural EquationModeling, 9, 151-173.
Luckasson, R., Borthwick-Duffy, S., Buntix, W. H. E., Coulter, D. L., Craig, E. M., Reeve, A., Schalock, R. L., Snell, M. E., Spitalnik, D. M., Spreat, S., & Tassé, M. J. (2002). Mental retardation: Definition, classification, and systems of supports (10th ed.).
Washington DC: American Association on Mental Retardation. Masters, G. N. (1982). A Rasch model for partial credit scoring. Psychometrika, 47, 149-174.
Matson, J. L., Rivett, T. T., Fodstad, J. C., Dempsey, T., & Boisjoli, J. A. (2009). Examination of adaptive behavior differences in adults with autism spectrum disorders and intellectual disability. Research in Developmental Disabilities, 30, 1317-1325.
Montero, D. (1993). Evaluación de la conducta adaptativa en personas con discapacidades. Adaptación y validación del ICAP. Bilbao: Mensajero.
Mueller, R. O., & Hancock, J. R. (2008). Best practices in structural equation modeling. In J. W. Osborne (Ed.), Best practices in quantitative methods (pp. 488-508). Thousand Oaks, CA: Sage Publications, Inc.
Navas, P., Verdugo, M. A., Arias, B., & Gómez, L.E. (2010). La conducta adaptativa en personas con discapacidad intelectual. Siglo Cero, 41, 28-48.
Navas, P., Verdugo, M.A., Arias, B., & Gómez, L.E. (2012). Development of an instrument for diagnosing significant limitations in adaptive behavior in early childhood. Research in Developmental Disabilities, 33(5), 1551-1559.
Reise, S. P., Moore, T. M., & Haviland, M. G. (2010). Bifactor models and rotations: Exploring the extent to which multidimensional data yield univocal scale scores. Journal of Personality Assessment, 92, 544-559.
Satorra, A., & Bentler, P. M. (2010) Ensuring positiveness of the scaled difference chi-square test statistic. Psychometrika, 75, 243-248.
Schalock, R. L. (1999). Adaptive behavior and its measurement: Implications for the field of mental retardation. Washington, DC: American Association on Mental Retardation.
Schalock, R. L., Borthwick-Duffy, S. A., Bradley, V., Buntix, W. H. E., Coulter, M. D., Craig, E. M., Gomez, S. C., Lachapelle, Y., Luckasson, R., Reeve, A., Shogren, K. A., Snell, M. E., Spreat, S., Tassé, M. J., Thompson, J. R., Verdugo, M. A., Wehmeyer, M. L., & Yeager, M. H. (2010). Intellectual disability. Definition, classification and systems of supports (11th ed.). Washington, DC: American Association on Intellectual and Developmental Disabilities.
Sparrow, S., Cicchetti, D., & Balla, D. (2005). VinelandAdaptive Behavior Scales, Second Edition (Vineland-II). Circle Pines, MN: American Guidance Service.
Tassé, M. J. (2009). Adaptive behavior assessment and the diagnosis of mental retardation in capital cases. Applied Neuropsychology, 16, 114-123.
Tassé, M. J., Schalock, R. L., Balboni, G., Bersani, H., Duffy, S. A., De Valenzuela, J. S., Spreat, S., Thissen, D. M., Widaman, K. F., & Zhang, D. (2012). The construct of adaptive behavior: Its conceptualization, measurement, and use in the field of intellectual disability. American Journal on Intellectual and Developmental Disabilities, 117, 291-303.
Tassé, M. J., Schalock, R. L., Balboni, G., Bersani, H., Duffy, S. A., De Valenzuela, J. S., Spreat, S., Thissen, D. M., Widaman, K. F., & Zhang, D. (in press). Diagnostic Adaptive Behavior Scale: User's Manual. Washington, DC: American Association on Intellectual and Developmental Disabilities.
Temperaal, D. T., Schim, S., & Gijselaers, W. H. (2007). A structural equation model analyzing the relationship of student's attitudes toward statistics, prior reasoning abilities and course performance. Statistics Education Research Journal, 6, 78-102. Verdugo, M. A. (2003). Análisis de la definición de discapacidad intelectual de la Asociación Americana sobre Retraso Mental de 2002. Siglo Cero, 34, 5-19.
Verdugo, M. A., Arias, B., Gómez, L. E., & Schalock, R. L. (2010). Development of an objective instrument to assess quality of life in social services: Reliability and validity in Spain. InternationalJournal of Clinical and Health Psychology, 10, 105-123.
Verdugo, M.A., Arias, B., & Navas, P. (in press). Escala de Diagnóstico de Conducta Adaptativa. Madrid: TEA.
Wechsler, D. (2005). WISC-IV: Escala de Inteligencia de Wechsler para niños-IV. Madrid: TEA.
Widaman, K. F., Borthwick-Duffy, S. A., & Little, T. D. (1991). The structure and development of adaptive behaviors. International Review of Research in Mental Retardation, 17, 1-54.
Widaman, K. F., & McGrew, K. S. (1996). The structure of adaptive behavior. In J. W. Jacobson & J. S. Mulick (Eds.), Manual of diagnosis and professional practice in mentalretardation (pp. 97-110). Washington, DC: American Psychological Association.
