



The aim of the study was to explore the differences between physical activity and/or screen time levels on cognitive (Life satisfaction LS) and affective (Positive affect, PA and Negative affect NA) components of subjective well-being (SWB) in children.
MethodThis cross-sectional study enrolled 1,540 children (1,040 boys, 8–12 years old). LS, PA, NA, physical activity and screen time were assessed with validated questionnaires.
ResultsChildren who reported 3 days per week of physical activity or less had lower LS and PA than counterparts with ≥6 days of physical activity per week (p < .05). Participants who reported 2 hours per day or less of screen time had lower NA than counterparts with 4 hours per day or more of screen time (p < .05). Also, children who meet physical activity guidelines have higher LS and PA compared to inactive peers, even with high screen time. In contrast, excessive screen time was also related with NA independent of the level of physical activity.
ConclusionsOur findings suggest that physical activity is related with positive feelings and LS, but does not eliminate the effect of screen time on negative feelings among Chilean children.
Este estudio explora las diferencias entre la actividad física y/o los niveles de tiempo de pantalla en los componentes cognitivo (Satisfacción de la vida SV) y afectivo (Afecto positivo AP y Afecto negativo AN) del bienestar subjetivo en niños.
MétodoSe incluyó a 1.540 niños (1.040 niños, 8 a 12 años). La SV, AP, AN, actividad física y tiempo de pantalla se evaluaron con cuestionarios validados.
ResultadosLos niños que informaron 3 días/semana de actividad física o menos tenían menos SV y AP que sus homólogos con 6 días/semana de actividad física o más (p < 0,05). Los que informaron menos de 2 horas por día de tiempo de pantalla tuvieron menos AN que sus homólogos con más o igual a 4 horas por día de tiempo de pantalla (p < 0,05). Además, los niños que cumplen con las pautas de actividad física tienen mayor SV y AP en comparación con los inactivos, incluso con un tiempo de pantalla elevado. Por el contrario, el tiempo de pantalla excesivo también se relacionó con el AN independientemente del nivel de actividad física.
ConclusionesLos hallazgos sugieren que la actividad física está relacionada con emociones positivas y SV, pero no elimina el efecto del tiempo de pantalla en las emociones negativas.
Around the world the importance of measuring subjective well-being (SWB) has been recognized as an indicator of positive children development (Casas, 2011). According to the literature, SWB is considered as a key component of good life and reflects the subjective judgment of wellbeing (Diener, Inglehart, & Tay, 2013). Specifically, following the Diener’s tripartite model of SWB (Diener, 1984), this construct is defined as the evaluation of the quality of a person’s life from their own perspective and is composed by cognitive and affective components. These include the experiences of pleasant emotions (positive affect, PA), the experiences of negative emotions such as distress and dissatisfaction (negative affect, NA) and judgment of individuals’ life qualities (overall life satisfaction or satisfaction with a specific domain, LS) (Diener et al., 2013). Childhood represents a period of rapid growth characterized by development of identity and the establishment of behavioral patterns that may enhance or diminish mental health and, consequently, SWB (Hofstra, Van Der Ende, & Verhulst, 2002).
Regular participation in physical activity is imperative for good physical and mental health (Committee PAGA, 2018). Globally, approximately 80% of school youth does not meet the World Health Organization’s (WHO) moderate-to vigorous physical activity guidelines for health (Sallis et al., 2016). In Chile, on average, 27.4% of children (9 to 11 years old) and 18.9% of adolescents meet the PA guidelines based on national data (Aguilar-Farias et al., 2018). Previous studies have shown that levels of physical activity have been linked negatively with self-reported levels of depression, anxiety (Parfitt & Eston, 2005), headaches, feeling low, irritability, and feeling nervous (Marques, Calmeiro, Loureiro, Frasquilho, & de Matos, 2015). Also, is positively associated with self-esteem (Breslin et al., 2012; Parfitt & Eston, 2005), life satisfaction (Breslin et al., 2012; Zullig & White, 2011), comfort, resilience, achievement (i.e., perceived performance both academically and socially with peers) (Breslin et al., 2012) and even with bullying victimization (Garcia-Hermoso, Oriol-Granado, Correa-Bautista, & Ramírez-Vélez, 2019; Hormazábal-Aguayo et al., 2019), all of them closely related with SWB. Recently, a meta-analysis suggests that physical activity has a small positive effect on mental health (i.e., psychological ill-being [depression, anxiety, stress or negative affect] and/or psychological well-being [self-esteem, self-concept, self-efficacy, self-image, positive affect, optimism, happiness and satisfaction with life] outcomes) in adolescents (Rodriguez-Ayllon et al., 2019). However, also notes that studies among children are scarce. Therefore, it is important to examine the overall effect of physical activity on the mental health outcomes of young people in order to guide health policies for this population.
In the past few years, sedentary behaviour has emerged as an important and independent risk factor for children’s physical health, additionally to the level of physical activity (García-Hermoso, Saavedra, Ramírez-Vélez, Ekelund, and Del Pozo-Cruz, 2017). A systematic review suggests a strong negative association between sedentary behaviour (especially screen-based activities) and different indicators of quality of life (Suchert, Hanewinkel, & Isensee, 2015). For example, Yang, Helgason, Sigfusdottir, and Kristjansson (2012) reveal a clear dose-response relationship between screen-based activities use and several negative health and feelings indicators (sad, appetite, lonely, want to cry, sleeping problem, hopeless). Also, the increase of any type of sedentary time was associated with more psychological complaints, such as depression or lower psychological well-being (Rodriguez-Ayllon et al., 2019).
According to the displacement hypothesis (Carlson et al., 2010), prolonged screen time would inevitably reduce physical activity time, or at least a co-occurrence between low physical activity and high sedentary behaviors exists. Several studies indicate opposite findings that screen time and physical activity might alter health dimensions independently (García‐Hermoso et al., 2017), but also interact between them (Rosenberger et al., 2019). Regarding this interaction and their relationship with SWB, results are inconclusive (Brindova et al., 2015; Hrafnkelsdottir et al., 2018; Matin et al., 2017). For example, Brindova et al. (2015), in 8,042 Slovak adolescents from the Health Behaviour of School-aged Children study show that sedentary behaviors are associated with health complaints (i.e., headache, backache, sleep difficulties, feeling low, irritability and feeling nervous) and that these associations are not moderated by physical activity. In contrast, another study in to 14,880 Iranian children and adolescents reported that although the amount of screen time is a factor with negative impact on LS, the impact can be overshadowed by more intense and effective physical activity (Matin et al., 2017).
Despite the scientific evidence above-mentioned, there is confusion in literature about these associations because it is being equated SWB with broader forms of well-being. Subjective well-being implies an overall evaluation of the quality of life from the person’s own perspective (Pavot, Diener, Oishi, & Tay, 2018). For this reason, it is typically assessed using subjective measures (self-reports) that consider cognitive and affective components of SWB according to Diener’s tripartite model (Diener, 1984). Therefore, it can be argued that the absence of NA, the presence of PA and the cognitive evaluation of LS as a whole needs to be assessed to fully reflect SWB (Parfitt & Eston, 2005). Also, due to the high level of physical inactivity and screen time among Chilean children (Aguilar-Farias et al., 2018), and their mental health problems at an early age (Rescorla et al., 2011), it seems appropriate to analyze the relationship between them. To summarize, it is necessary to extend the literature in children population, mapping the links between physical activity, screen time and SWB and their interaction. Also, in Chile, a region which has undergone a well-documented epidemiologic transition fueling an epidemics of non-communicable diseases (Albala & Vio, 1995), relatively little research on physical activity and mental health has been done. This is important to assess, particularly in the context of a low-to-middle income country setting like Chile. We hypothesized that children who achieve higher levels of physical activity and lower screen time (2 h/d or less) have more SWB compared to their more inactive or sedentary counterparts, respectively. Also, active children both with low or high screen time will have higher LS and PA and lower NA compared to counterparts inactive and with high levels of screen time. Thus, the aim of the study was to explore the differences between physical activity and/or screen time levels on LS, PA, and NA in Chilean children.
MethodParticipantsData were collected from 2016 to 2017 and analyzed in 2018. A sample consisting of 1,540 children aged 8–12 years old (from third to sixth grade; 1,040 boys and 500 girls) was included. The children were of low–middle socioeconomic status and were enrolled in eight public schools in the district of Santiago (Chile). These schools were randomly-selected from a total of 21 possible schools. For this purpose, the sample was selected using a nonprobability sampling. However, although we used this type of sampling, all schoolchildren from the selected schools were invited to participate. Sample size calculation indicated that the 1,540 children included in the study were sufficient to detect a coefficient correlation of .20 between physical activity and LS in a two-sided test (alpha < .05, 95% power). Subjects were excluded if they had any type of dysfunction that limited their physical activity (i.e., any disease or problem) or if they had not lived in Santiago (Chile) for at least one school year. None of the children were taking any drug treatments. Exclusion from the study analysis was made effective a posteriori without the students being aware of their exclusion so as to avoid any undesired situations.
The study protocol was approved by the University of Santiago Ethics Committee (Code number: 938) and complied with the principles of the Declaration of Helsinki. A letter was sent to the children’s parents of each school inviting them to a meeting where the objectives were explained, after which they signed the informed consent for their children to participate in the study and the assent of the participants.
InstrumentsA group of trained researchers conducted with the pupils under quiet classroom conditions. The classroom teacher was present at all times. These trained researchers measured the variables and outcomes of the study under standardized conditions. All of the questionnaires were filled by the children with the help of researchers. Data were collected at the same time in the morning, between 8:00 am and 12:00 am.
Anthropometric parameters. Body weight was measured to the nearest 0.1 kg using a portable electronic scale (Seca 769, Hamburg, Germany), and height was measured to the nearest 0.1 cm using a portable stadiometer (Seca 220, Hamburg, Germany). Body mass index (BMI) was subsequently derived, and the BMI z-score was determined using the International Obesity Task Force age-specific and sex-specific thresholds (Cole, Bellizzi, Flegal, & Dietz, 2000). Anthropometric measurements were made when students were barefoot and wearing light clothing.
Subjective Well-Being. Subjective well-being was evaluated according to Diener’s tripartite model (Diener, 1984), evaluating the LS, PA and NA as follow. Life Satisfaction: this scale is a part of CUBE (in Spanish: Cuestionario Único de Bienestar Escolar) developed and validated by the Ministry of Peru and used in a previous study (Miranda, Oriol, Amutio, & Ortúzar, 2018). It is composed by 5 items and assesses different items of LS. All these variables were measured through a 10-point Likert scale ranging from 0 to 10 (0 = totally disagree, 10 = totally agree). This scale presents a high level of reliability (alpha coefficient = .83). Positive affect: this scale consists of 5 items evaluating positive affect (“How Happy, Joyful, Cheerful, Content, Fun”) and 5 for negative affect (“Humiliated, Bothered, Irritated, Embittered and Sad”) and contains a bifactorial structure with 5 items per factor (Damásio, Pacico, Poletto, & Koller, 2013). The items are answered using a five-point scale (1—not even a little, 5—a lot). The alpha coefficient was .75 for NA and .84 for PA.
Physical activity. The measurement of physical activity was based on the following question: “Normally: how many days were you physically active for a total of at least 60 min?”. This measure has shown to have good reliability and validity (Prochaska, Sallis, & Long, 2001). Response options ranged from 0 to 7 days per week, in 1-day increments. Physical activity was defined as less than 60 min of physical activity per day on at least 7 per week. The intraclass correlation coefficient was .77 (Prochaska et al., 2001).
Also, sports participation was assessed by asking participants the following question: “In your free time, do you do any of these organized activities?” with response categories yes/no was followed by the explanatory text: “We mean activities you do in sports or other clubs or organizations”.
Screen time. Screen time was assessed by asking participants to report the number of hours per typical day in the past seven days: “On an average school day, how many hours do you watch TV, play video or computer games or use a computer for something that is not school work?”. Response options were 1 = No time, 2 = about 1 hour, 3 = about 2 hours, 4 = about 3 hours, 5 = about 4 hours, and 6 = 5 hours or more. The alpha coefficient was .72. Screen time use was dichotomized (low screen time: less than 2 h/d and high screen time 2 h/d or more) based on international guidance on limiting pediatric screen time (Bar-On et al., 2001).
Statistical analysisDescriptive data are presented as means and standard deviation for continuous variables and frequencies and percentages for categorical variables. To assess the differences between sexes, the independent Student’s t-test was used for continuous variables and the Chi-squared test was used for categorical variables. All the variables satisfied the tests of homoskedasticity (Levene variance homogeneity test) and normality (Kolmogorov-Smirnov test) of their distributions (p > .05). Preliminary analyses showed no significant interactions between sex and mean differences in physical activity or screen time (all p > .10); therefore, all analyses were performed with boys and girls together to increase statistical power. Analysis of covariance (ANCOVA) and pairwise post-hoc comparisons were examined using Bonferroni test. The following analyses were used: (i) the differences in LS, PA and NA per 1-day increments per week of physical activity or 1-h increments per day of screen time; (ii) the differences between mean values of LS, PA and NA across physical activity (active or inactive) and screen time (low or high) categories, adjusted by age, sex, BMI z-score, sport participation, school, and physical activity or screen time according to the dependent variable included in the model; and (iii) the differences between mean values of LS, PA and NA across combined groups of physical activity (active or inactive) and screen time (low or high). Then, four exclusive groups were created: (1) active/low screen time; (2) active/high screen time; (3) inactive/low screen time; and (4) inactive/high screen time. These last analyses were adjusted by age, sex, BMI z-score, sport participation, and school. Data analyses were performed using the Statistical Package for Social Sciences (Version 21.0) software. P < .05 was considered statistically significant.
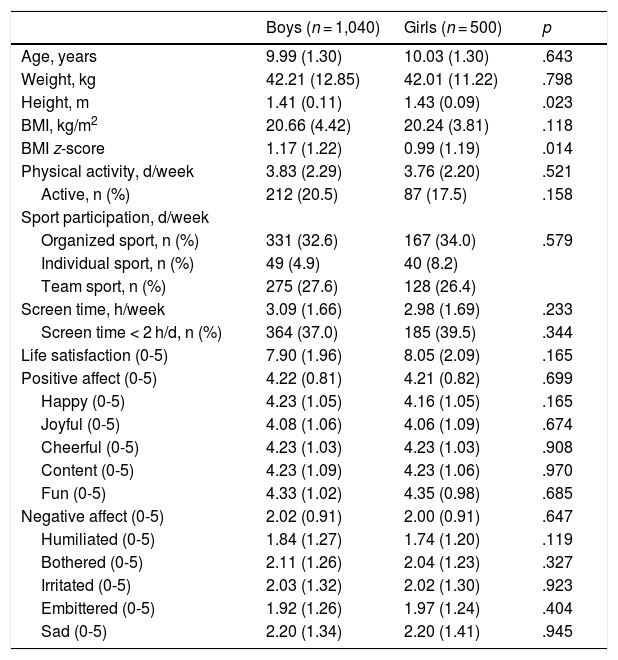
ResultsTable 1 shows the descriptive characteristics of the children. The only significant difference between boys and girls was in BMI z-score (p = .014). A total of 212 boys (20.5%) and 87 girls (17.5%) self-reported that they met the recommended 60 minutes of physical activity each day of the week. Also, the prevalence of high screen time was 37.0% and 39.5%, in boys and girls respectively.
Participants’ characteristics.
| Boys (n = 1,040) | Girls (n = 500) | p | |
|---|---|---|---|
| Age, years | 9.99 (1.30) | 10.03 (1.30) | .643 |
| Weight, kg | 42.21 (12.85) | 42.01 (11.22) | .798 |
| Height, m | 1.41 (0.11) | 1.43 (0.09) | .023 |
| BMI, kg/m2 | 20.66 (4.42) | 20.24 (3.81) | .118 |
| BMI z-score | 1.17 (1.22) | 0.99 (1.19) | .014 |
| Physical activity, d/week | 3.83 (2.29) | 3.76 (2.20) | .521 |
| Active, n (%) | 212 (20.5) | 87 (17.5) | .158 |
| Sport participation, d/week | |||
| Organized sport, n (%) | 331 (32.6) | 167 (34.0) | .579 |
| Individual sport, n (%) | 49 (4.9) | 40 (8.2) | |
| Team sport, n (%) | 275 (27.6) | 128 (26.4) | |
| Screen time, h/week | 3.09 (1.66) | 2.98 (1.69) | .233 |
| Screen time < 2 h/d, n (%) | 364 (37.0) | 185 (39.5) | .344 |
| Life satisfaction (0-5) | 7.90 (1.96) | 8.05 (2.09) | .165 |
| Positive affect (0-5) | 4.22 (0.81) | 4.21 (0.82) | .699 |
| Happy (0-5) | 4.23 (1.05) | 4.16 (1.05) | .165 |
| Joyful (0-5) | 4.08 (1.06) | 4.06 (1.09) | .674 |
| Cheerful (0-5) | 4.23 (1.03) | 4.23 (1.03) | .908 |
| Content (0-5) | 4.23 (1.09) | 4.23 (1.06) | .970 |
| Fun (0-5) | 4.33 (1.02) | 4.35 (0.98) | .685 |
| Negative affect (0-5) | 2.02 (0.91) | 2.00 (0.91) | .647 |
| Humiliated (0-5) | 1.84 (1.27) | 1.74 (1.20) | .119 |
| Bothered (0-5) | 2.11 (1.26) | 2.04 (1.23) | .327 |
| Irritated (0-5) | 2.03 (1.32) | 2.02 (1.30) | .923 |
| Embittered (0-5) | 1.92 (1.26) | 1.97 (1.24) | .404 |
| Sad (0-5) | 2.20 (1.34) | 2.20 (1.41) | .945 |
Note. Data are mean (SD) or number and proportions (%).
Table 2 shows the differences between mean values of life satisfaction, positive and negative affect items across physical activity (active or inactive) and screen time (less than 2 h/d and 2 h/d or more) categories. Physically active children showed higher LS and PA (even analyzing each items separately) compared to inactive peers (all p < .01 except for “joyful” item [p = .024]) independent of the screen time and another potential covariates. Also, children that spent 2 hours or more per day of screen time reported higher NA (p = .019) (specifically for “irritated”, “embittered” and “sad” items) in comparison to those with low screen time (i.e., less than 2 h/d).
Differences in well-being variables according to physical activity and screen time categories.
| Physical activity | Screen time | |||||
|---|---|---|---|---|---|---|
| Active | Inactive | pa | < 2 h/d | ≥ 2 h/d | pa | |
| Life satisfaction (0-10) | 7.79 (2.00) | 8.45 (1.92) | .002 | 8.04 (1.96) | 7.88 (2.02) | .366 |
| Positive affect (0-5) | 4.49 (0.74) | 4.16 (0.82) | <.001 | 4.27 (0.79) | 4.20 (0.83) | .276 |
| Negative affect (0-5) | 1.99 (1.01) | 2.02 (0.88) | .748 | 1.91 (0.88) | 2.08 (0.92) | .019 |
Note. Data are mean (SD). Analyses were fully adjusted by age, sex, body mass index z-score, organized sport participation, school, and physical activity or screen time according to dependent variable. aPairwise comparisons by using Bonferroni's post hoc hypothesis tests for multiple comparisons.
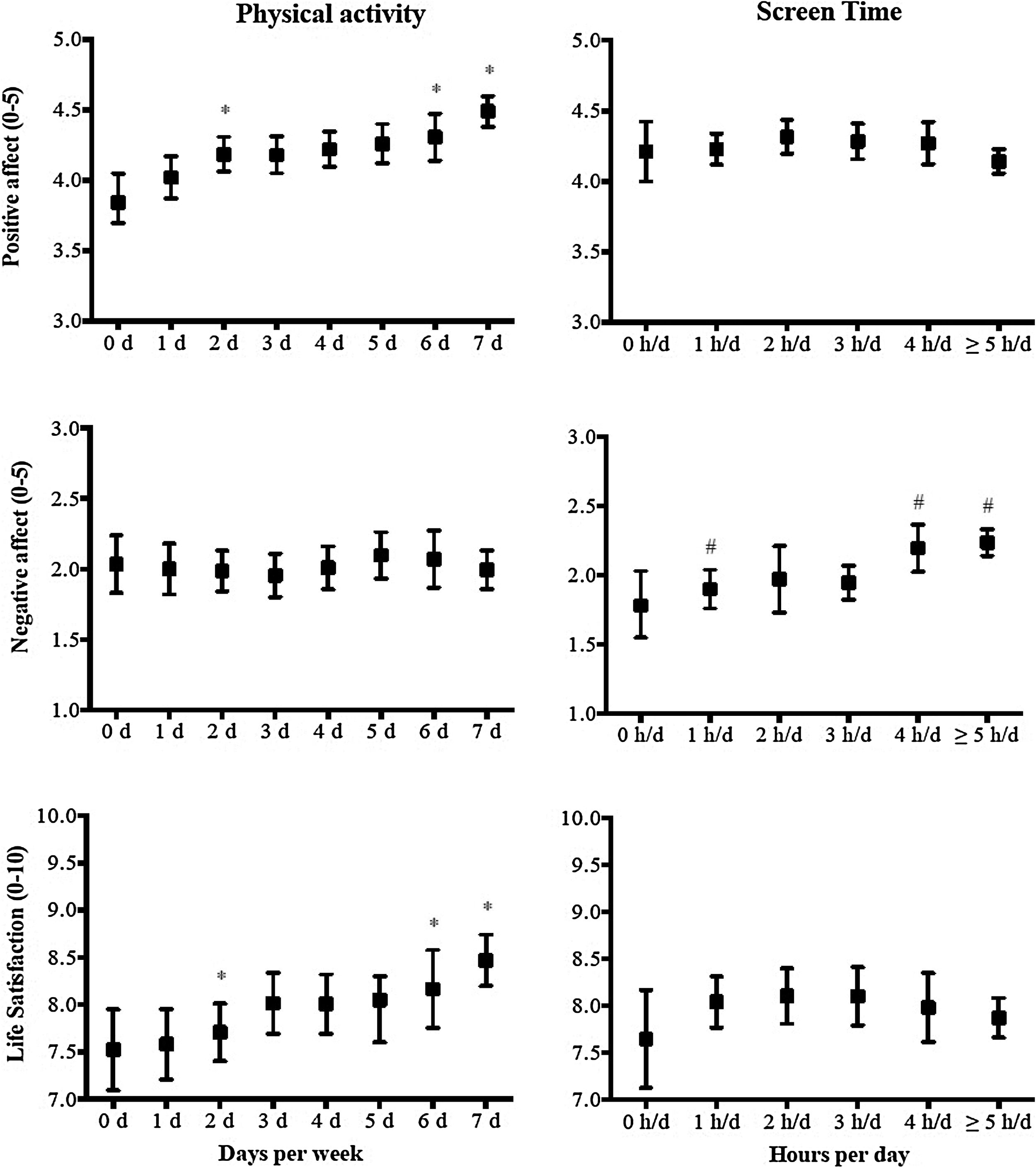
Figure 1 shows the differences in LS, PA and NA items per 1-day increments per week of physical activity or 1 -h increments per day of screen time. Children who reported 3 days per week of physical activity or less had lower LS and PA than counterparts with more than 6 days of physical activity per week (p < .05). Also, children who reported less than 2 hours per day of screen time had lower NA than counterparts with 4 hours per day of screen time or more (p < .05).
 or 1-h increments per day of screen time (B) in Chilean children. Adjusted for age, sex, BMI z-score, sport participation, school, and physical activity or screen time according to the dependent variable included in the model. Pairwise post-hoc comparisons were examined using Bonferroni test. * 3 or less days per week was smaller than 6 days or more per week (p < .05); # Less than 2 hours per day was smaller than 4 hours or more per day (p < .05).")
Differences in life satisfaction, positive and negative affect items per 1-day increments per week of physical activity (A) or 1-h increments per day of screen time (B) in Chilean children. Adjusted for age, sex, BMI z-score, sport participation, school, and physical activity or screen time according to the dependent variable included in the model. Pairwise post-hoc comparisons were examined using Bonferroni test. * 3 or less days per week was smaller than 6 days or more per week (p < .05); # Less than 2 hours per day was smaller than 4 hours or more per day (p < .05).
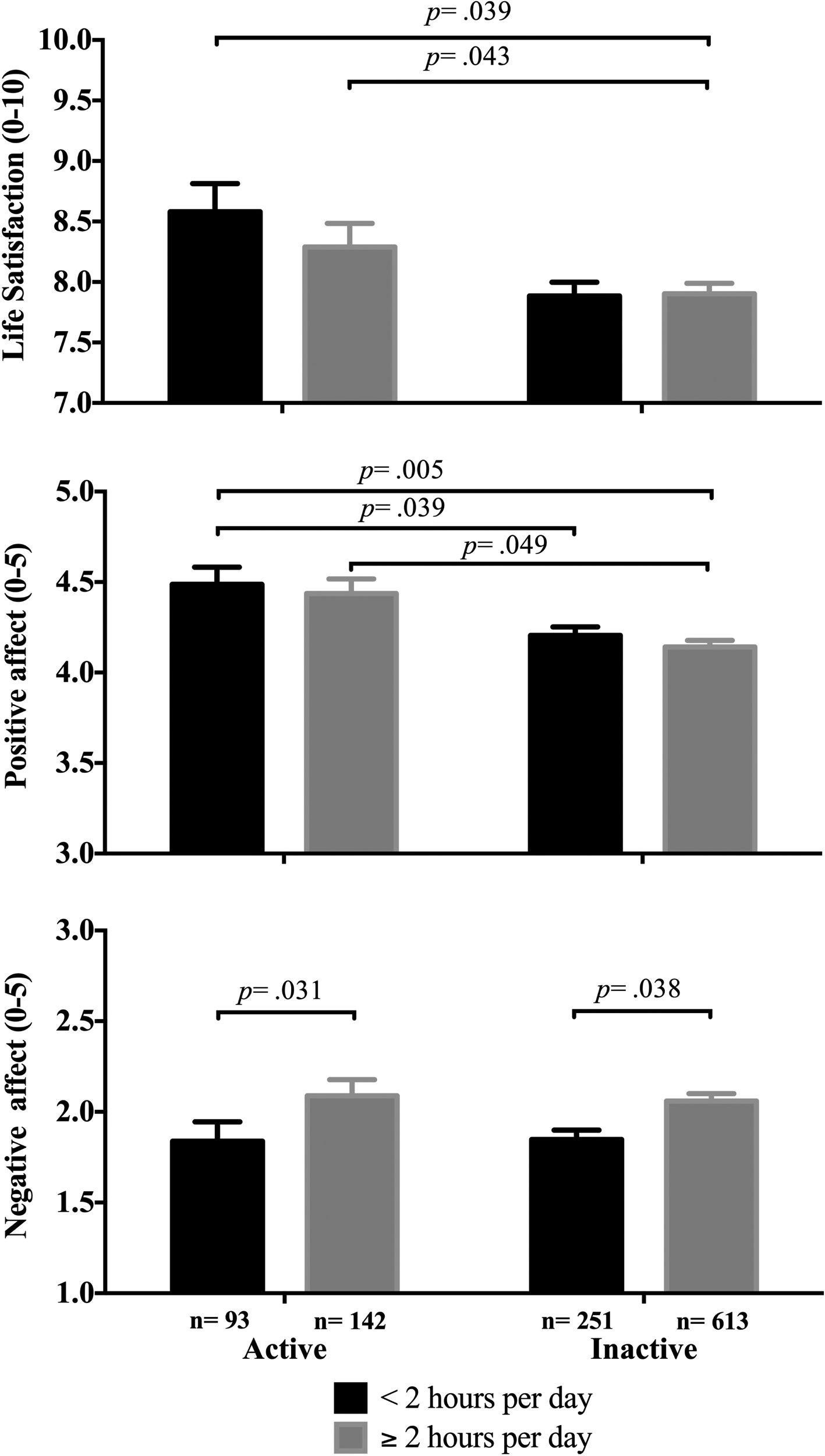
Finally, Figure 2 shows differences between mean values of LS, PA and NA across combined groups of physical activity (active or inactive) and screen time (low or high) adjusted by age, sex, BMI z-score, and sport participation. Active group both with low (p = .039) or high screen time (p = .043) time show higher LS compared to inactive/high screen time group. Regarding PA, active group independent of screen time (low [p = .039] and high [p = .005]) reported higher PA compared to inactive/high screen time group; also, active/high screen time group shows higher PA compared to inactive/high screen time group (p = .049). Finally, active/high screen time group shows higher NA compared to active/low screen time group (p = .031); also, inactive/high screen time group reports higher NA than inactive/low screen time group (p = .038).
Discussion/Conclusions and screen time (low or high). Pairwise post-hoc comparisons were examined using Bonferroni test.")
The current study explored the relationship between physical activity, screen time and SWB, assessed according to the Diener’s tripartite model (Diener, 1984) (i.e., analising LS, PA and NA) in Chilean children. Our study demonstrated that children who meet the physical activity guidelines have higher LS and positive affect compared to inactive peers, even with high screen time (2 hours per day or more). In contrast, excessive screen time was related with NA.
Engaging in 60 minutes or more per day of moderate-to-vigorous physical activity is commonly recommended for better health and quality of life among children and adolescents (Committee PAGA, 2018). Meeting the physical activity recommendations is vital to the physical, psychological/social, and cognitive health of school-aged children and adolescents (Committee PAGA, 2018; Poitras et al., 2016). Our findings suggest that meeting these physical activity guidelines are related with high LS and PA, but not with NA. Several studies have had similar results to ours, although using different questionnaires (Breslin et al., 2012; Parfitt & Eston, 2005). However another study, Marques et al. (2015) in 4,462 Portuguese adolescents aged 11-16 years old, also found a relationship between physical activity and negative feelings such as low, irritability, and nervous among boys. Several potential mechanisms have been suggested for positive relationships between physical activity, LS and PA: (i) regular physical activity has been associated with improving self-esteem, self-efficacy and cognitive and psychological function, reducing distress, and increasing social interaction and support (Biddle, Ciaccioni, Thomas, & Vergeer, 2019); (ii) physical activity may improve levels of mood-regulating neurotransmitters in the brain (Heijnen, Hommel, Kibele, & Colzato, 2016) or the production of endorphins and their pain reduction and euphoric effects (Compton & Hoffman, 2013); and (iii) according to broaden-and-build theory of positive emotions proposed by Fredrickson, Cohn, Coffey, Pek, and Finkel (2008), the experiences of daily living such as physical activity induce PA (but not negative), increasing personal resources (e.g., self-esteem, self-efficacy and optimism) which helps increase LS. That it means, that people who regulary experience PA through physical activity, can increase a positive judment of themselves and in turn, facilitate a better overall perception of their lives.
Regarding screen time, previous findings provide evidence that sedentary behaviour should be considered as an independent risk factor for mental health, including depressive symptomatology and psychological distress, decreased perceptions of self-worth, and lower perceived quality of life and self-esteem (Rodriguez-Ayllon et al., 2019; Suchert et al., 2015). These findings were confirmed by our results, showing that high screen time is related with NA in Chilean children, specifically with “irritated”, “embittered” and “sad” feelings. However, screen time was not related with LS and PA, confirming results on Iranian youth (Matin et al., 2017). Our results about NA, support most of the previous cross-sectional findings in other children and adolescent age groups (Hrafnkelsdottir et al., 2018; Matin et al., 2017; Yang et al., 2012). More specifically, Yang et al. (2012) in 10,829 children aged 10-12-year-old demonstrate a dose-response relationship between screen-based activities use and several psychological well-being parameters such as sad, hopeless and lonely feelings. In adolescents, another studies reveal that high screen time levels are associated with increased chance of being irritable or feeling nervous among others health complaints (Marques et al., 2015; Brindova et al., 2015). One of the main potential mechanisms underlying such associations could be that screen time leads to social withdrawal, social isolation, and hence to internalizing problems and less SWB (Suchert et al., 2015). According to Fairburn, Cooper, and Shafran (2003)), negative emotions likely impact a number of processes that inhibit social connection, which could encourage the children to a higher screen time.
Our study contributes to the limited knowledge base of the interactive effects of physical activity and screen time on SWB among children (Hrafnkelsdottir et al., 2018; Matin et al., 2017), and this is the first study on this topic among Latino children. It is important to note two findings: (i) physically active children regardless of screen time use reported higher LS and PA compared to inactive peers, but not for negative affects; and (ii) high screen time is associated with higher NA in physically active and inactive children compared to those with low screen time counterparts. Despite that physical activity may alter psycho-physiological responses to screen time exposure and, partly reduces the risk of psychological ill effects (Brand et al., 2010), our results among others (Matin et al., 2017) suggest that the effect of screen-based media is not overshadowed by physical activity when they are both in the equation.
Certain weaknesses and strengths should be noted. Firstly, the cross-sectional nature of the data limit causal inference between physical activity, screen time and SWB outcomes, and reverse causation may exist if children with low SWB are less likely or able to participate in physical activity and/or more likely to spend more time in front of screens, and vice versa. However, appropriate analysis of cross-sectional data represents a useful initial step in identifying associations between these behaviors and psychological parameters in Latino children. The findings, therefore, need to be confirmed in longitudinal and intervention studies. Second, the study subjects were sampled within one district of the city of Santiago, Chile. Third, self-report measurements were used to assess physical activity and screen time in this study. Finally, the sample was not balanced according to sex. The most important strength of the present study was the use of standardized and validated measuring tool for our assessment of SWB according to the Diener’s tripartite model (Diener, 1984) in a large sample of Chilean children.
In conclusion, our study demonstrated that children who meet the physical activity guidelines and have high screen time are separately and interactively associated with high life satisfaction and positive or negative affect, respectively. Therefore, it seems important to decrease the amount of time which children spend on screen-based activities and, at the same time to promote regular physical activity in order to reduce negative feelings and improve SWB.
FundingThis study was funded by the Vicerrectoría de Investigación, Desarrollo e Innovación (Proyectos Basales. Grand number: 051641ZR_DAS) of the Universidad de Santiago de Chile (Chile). AGH is a Miguel Servet Fellow (Instituto de Salud Carlos III – CP18/0150). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
