


Positive mental health (PMH) has been shown to confer resilience against suicide ideation. However, the mechanisms underlying the positive effect of PMH on suicide ideation/behavior are largely unknown. The current study aimed to determine whether positive affect mediates the association between PMH and suicide ideation.
MethodA total of 150 adult outpatients (65.3%; female; age: M(SD)=37.79(13.50), range:18–77) completed measures on PMH, positive and negative affect, as well as suicide ideation. Data were collected using self-report questionnaires. Linear hierarchical regression analysis was used to analyze the data. Positive affect was considered to mediate the association between positive mental health and suicide ideation.
ResultsWhile positive affect fully mediated the significant negative association between PMH and suicide ideation, negative affect did not reveal to be a significant mediator of this relationship.
ConclusionsThe protective influence of PMH against suicide ideation is due to heightened positive affect: If positive mental health translates into positive affect, then suicide ideation becomes less likely.
Se ha demostrado que la salud mental positiva (SMP) confiere resistencia contra la ideación de suicidio. Sin embargo, los mecanismos subyacentes al efecto positivo de la SPM en la ideación/comportamiento suicida son en gran medida desconocidos. El objetivo del presente estudio fue determinar si el efecto positivo media la asociación entre el SPM y la ideación suicida. Método: Un total de 150 pacientes externos adultos (65,3%; mujeres; edad: M(DT)=37,79(13,50), rango:18-77) completó las medidas sobre SPM, afectos positivos y negativos, así como la ideación de suicidio. Los datos se recopilaron mediante cuestionarios de autoinforme. Se utilizó el análisis de regresión jerárquica lineal para analizar los datos. Se consideró que el afecto positivo mediaba en la asociación entre la salud mental positiva y la ideación suicida.
ResultadosMientras que el afecto positivo mediaba completamente la asociación negativa significativa entre SPM e ideación suicida, el afecto negativo no reveló ser un mediador significativo de esta relación.
ConclusionesLa influencia protectora de la SMP contra la ideación de suicidio se debe a un mayor afecto positivo. Si la salud mental positiva se traduce en afecto positivo, entonces la ideación de suicidio se vuelve menos probable.
Positive mental health (PMH), that is, high levels of subjective and psychological well-being (Keyes, 2005) has been shown to confer resilience against suicide ideation/behavior. In this sense, PMH was found to moderate both the relationship between different risk factors (depression, cyberbullying) and suicide ideation( Brailosvskaia, Teismann, & Margraf, 2018;Siegmann et al., 2018), as well as the relationship between suicide ideation and suicide attempts (Brailovskaia et al., 2019). Corresponding effects were shown in cross-sectional studies (Siegmann et al., 2018) and in a longitudinal study (Teismann, Forkmann et al., 2018) using various samples (German students, Chinese students, psychiatric inpatients). Finally, a study of inpatients and outpatients showed that PMH and suicide ideation are not mutually exclusive, but exist simultaneously (Teismann, Brailovskaia et al., 2018Brailovskaia et al., 2018). Thus, PMH and suicide ideation/behavior are not opposite poles of a single dimension, but form two independent factors of mental health/mental illness (cf., Keyes, 2005).
Taken together, the relevance of PMH as a resilience factor has been demonstrated in a growing number of studies. However, at present, the mechanisms underlying the positive effect of PMH on suicide ideation/behavior are largely unknown. On the background of the broaden-and-build-theory (Fredrickson, 2013), one may speculate that positive mental health translates into more frequent everyday positive affect, which in turn has been shown to broaden an individual's mindset in ways that, over time, help to accumulate and build one's personal resources, such as resilience and social closeness (Fredrickson, 2013). In line with this reasoning, Joiner et al. (2001) could show that suicidal patients high in positive affectivity experience fewer suicidal symptoms following treatment as a function of gains in problem solving attitudes (indicative of cognitive broadening in the sense of Fredrickson, 2013). Furthermore, everyday positive affectivity has been shown to predict decreased probability of suicide ideation (Husky et al., 2017). However, no study so far has investigated whether positive affect mediates the association between habitual positive mental health and suicide ideation.
On this background, we hypothesized that positive affect mediates the association between positive mental health and suicide ideation in a sample of adult outpatients. To assure specificity, we also tested whether similar relations are linked to negative affect and predicted relations are specific to positive affect.
MethodParticipantsThe study sample comprises 150 outpatients (65.3%; female; age: M(SD)=37.79(13.50), range:18–77) who started treatment at a university outpatient clinic in Germany between April and October 2018 (see also Von Brachel, Teismann, Feider, & Margraf, 2019). The most common diagnoses according to the International Classification of Diseases (ICD-10; World Health Organization, 1992) were affective disorders (F3: n=66, 44%), neurotic, stress-related and somatoform disorders (F4: n=64, 42.7%) and personality disorders (F6: n=9, 6%).
Prior to assessments, participants were informed about the purpose of the study, the voluntary nature of their participation, data storage and security. They gave written informed consent before participating. The study was approved by the responsible Ethics Committee.
MeasuresPositive Mental Health Scale (PMH; Lukat, Margraf, Lutz, van der Veld, & Becker, 2016). The PMH-scale assesses subjective and psychological aspects of well-being across nine items (e.g., “I feel that I am actually well equipped to deal with life and its difficulties”), rated on a scale ranging from 0 (do not agree) to 3 (agree), with higher scores indicating greater PMH. Unidimensional structure, good convergent, and discriminant validity were demonstrated in various populations (Lukat et al., 2016). Cronbach's alpha was good in the current study: α=.91.
Suicide Ideation and Behavior Scale–Suicide Ideation Subscale (SSEV-SI; Teismann, Glaesmer, & Forkmann, 2017). The SSEV-SI assesses with four items the frequency of suicide ideation in the past four weeks (e.g., “During the past four weeks, … I thought it would be better if I wasn’t alive, … I wished I was dead, … I’ve been thinking about killing myself, … I have seriously considered killing myself”). All items are answered on a 6-point Likert scale ranging from “0=never” to “6=many times every day”, with higher scores indicating greater severity of suicidal ideation. Internal consistency was good in the current sample (α=.86).
Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). The PANAS includes two 10-item scales, one for positive affect and one for negative affect. Respondents are asked to indicate to which extent they felt each feeling or emotion during the past two weeks. Each item is rated on a 5-point scale of 1 (not at all) to 5 (very much). Internal consistency was good in the current sample: α=.85 (negative affect), α=.91 (positive affect).
Statistical analysesStatistical analyses were conducted with the Statistical Package for the Social Sciences (SPSS) 24 and the macro Process version 2.16.1 (www.processmacro.org/index.html). To assess associations between the investigated variables, correlation analyses and linear regression analyses were calculated, including suicide ideation as dependent variable, and age and gender as control variables. In the first model, positive mental health served as independent variable. In the second and third model, positive affect or negative affect was included as independent variable.
A mediation model was analyzed including positive affect or negative affect as hypothetical mediator. The basic relationship between positive mental health (predictor, X) and suicide ideation (outcome, Y) was denoted by c (total effect). The path of positive mental health to positive/negative affect (mediator, M) was denoted by a; the path of positive/negative affect to suicide ideation was denoted by b. The indirect effect was represented by the combined effect of path a and path b. Path c’ denoted the direct effect of positive mental health to suicide ideation after the inclusion of positive/negative affect. The mediation effect was assessed by the bootstrapping procedure (10.000 samples) that provides accelerated confidence intervals (95%), controlling for age and gender. Earlier studies (Wen & Fang, 2015) emphasized the shortcomings of the effect size kappa-squared (κ2) commonly used in mediation analyses. Therefore, PM (the ration of the indirect effect to the total effect) was used as mediation effect measure.
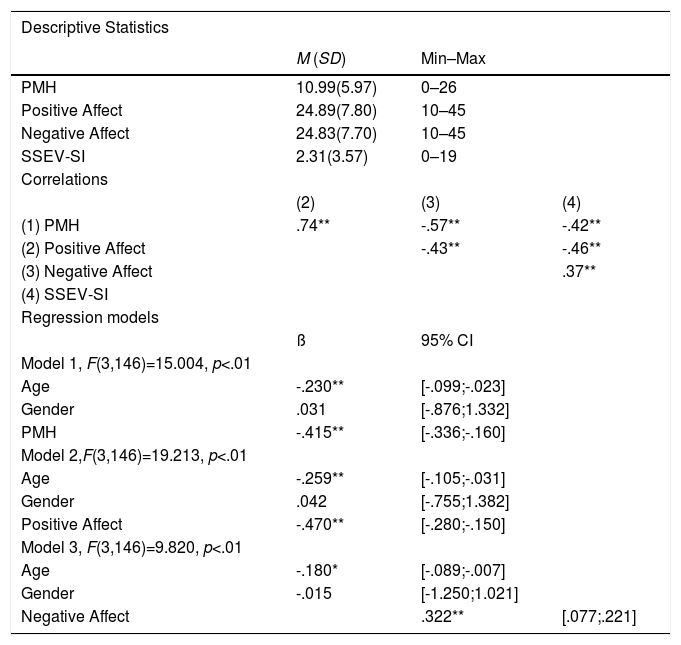
ResultsDescriptive and correlational data of all study variables are presented in Table 1. Concurrent suicide ideation (SSEV>0) was found in 50% (n=75) of the sample.
Descriptive statistics, correlations of investigated variables and linear regression analyses including suicide ideation as dependent variable.
| Descriptive Statistics | |||
|---|---|---|---|
| M (SD) | Min–Max | ||
| PMH | 10.99(5.97) | 0–26 | |
| Positive Affect | 24.89(7.80) | 10–45 | |
| Negative Affect | 24.83(7.70) | 10–45 | |
| SSEV-SI | 2.31(3.57) | 0–19 | |
| Correlations | |||
| (2) | (3) | (4) | |
| (1) PMH | .74** | -.57** | -.42** |
| (2) Positive Affect | -.43** | -.46** | |
| (3) Negative Affect | .37** | ||
| (4) SSEV-SI | |||
| Regression models | |||
| ß | 95% CI | ||
| Model 1, F(3,146)=15.004, p<.01 | |||
| Age | -.230** | [-.099;-.023] | |
| Gender | .031 | [-.876;1.332] | |
| PMH | -.415** | [-.336;-.160] | |
| Model 2,F(3,146)=19.213, p<.01 | |||
| Age | -.259** | [-.105;-.031] | |
| Gender | .042 | [-.755;1.382] | |
| Positive Affect | -.470** | [-.280;-.150] | |
| Model 3, F(3,146)=9.820, p<.01 | |||
| Age | -.180* | [-.089;-.007] | |
| Gender | -.015 | [-1.250;1.021] | |
| Negative Affect | .322** | [.077;.221] |
Notes. N=150; M=Mean; SD=Standard Deviation; Min=Minimum; Max=Maximum; PMH=Positive Mental Health; SSEV-SI=Suicide Ideation and Behavior Scale – Suicide Ideation Subscale; ß=standardized beta, CI=confidence interval. *p<.05, **p< .01.
In the first regression model that explained 23.6% of the variance, PMH was negatively linked to suicide ideation. Positive affect showed a negative association with suicide ideation in the second regression model (28.3% explained variance). In the third model, 16.8% of the variance was explained. Negative affect was positively related to suicide ideation (see Table 1).
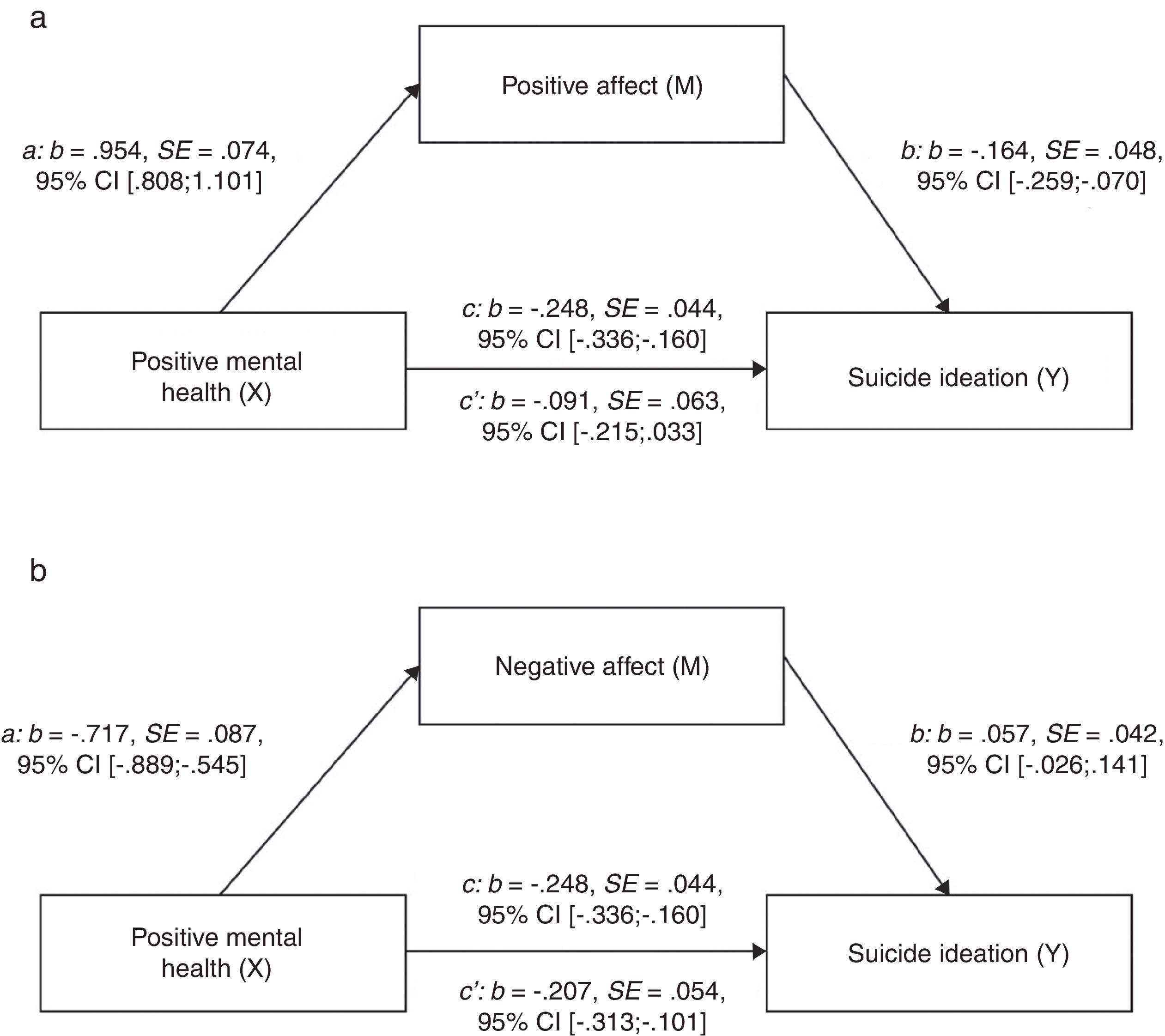
Figure 1a shows that positive affect fully mediated the relationship between PMH and suicide ideation in the first bootstrapped mediation analysis (c: p=.0000; c’: p=.1474). The indirect effect (ab) became significant, b=-.157, SE=.052, 95%CI[-.263;-.060]; PM: b=.632, SE=.309, 95%CI[.227;1.448]. In contrast, as presented in Figure 1b, negative affect did not serve as a significant mediator between PMH and suicide ideation (c: p=.0000; c’: p=.0002; indirect effect (ab): b=-.041, SE=.028, 95%CI[-.097;.014]; PM: b=.166, SE=.152, 95%CI[-.052;.513]).
 Mediation model including positive mental health (X), positive affect (M), and suicide ideation (Y). b) Mediation model including positive mental health (X), negative affect (M), and suicide ideation (Y). Note. c=total effect, c’=direct effect; b=standardized regression coefficient, SE=standard error, CI=confidence interval.")
a) Mediation model including positive mental health (X), positive affect (M), and suicide ideation (Y). b) Mediation model including positive mental health (X), negative affect (M), and suicide ideation (Y). Note. c=total effect, c’=direct effect; b=standardized regression coefficient, SE=standard error, CI=confidence interval.
The aim of the present study was to examine potential mechanisms underlying the association between positive mental health and suicide ideation. There were two main findings: (1) Positive affect mediates the association between positive mental health and suicide ideation. (2) Negative affect is not a mediator of this association. Results show that the protective influence of PMH against suicide ideation is due to heightened positive affect: If positive self-appraisals translate into positive affect, then suicide ideation becomes less likely. Of note, this effect is specific to the experience of positive affect. As such, decreased negative affect did not mediate the association between positive mental health and suicide ideation. This pattern of findings is in line with Frederickson's (2013) assumption that positive emotions are specific in broadening people's thought-action repertoires and help them to bounce back from adversities.
In terms of clinical implications, the results of the current study suggest that it may be important to account both for the presence of positive mental health and positive affect in addition to risk factors, when assessing individuals at risk for suicide. In fact, the experience and activation of positive affect during treatment sessions could possibly be used as an indicator of habitual positive mental health. Drawing from the broaden-and-built theory, Wingate et al. (2006) point out that clinicians might be expected to bring about the greatest treatment effects by deliberately inducing positive emotions in therapy (e.g., by asking patients to think about the best times in their lives) - even when working with suicidal patients. In line with this assumption, positive psychology interventions have been shown to be feasible in dealing with suicidal inpatients (Huffman et al., 2014).
There are several limitations to the present study. First, given the cross-sectional nature of the data, conclusions about causation are bound to involve some degree of speculation. Future studies should therefore make use of longitudinal study designs. In addition, EMA-approaches would allow a fine-grained analysis of the association between positive mental health, daily positive affect and suicide ideation. Second, as an outpatient sample was studied, levels of suicide ideation were rather modest. As such, it is unclear to what extent the results would generalize to high risk samples. Furthermore, it remains unclear in as much results would generalize to different patient groups (e.g., patients suffering from psychosis, personality disorders). In general, there is little knowledge on disorder-specific differences with regard to potential resilience or protective factors. Third, all constructs were assessed with self-report measures. It may well be that face-to-face interviews would have yielded different results. Especially since using the same method to assess all constructs could have resulted in biased estimates of the effects.
Taken together, the current study underscores the importance of positive mental health and positive affect as protective or resilience factors against suicide ideation.
We acknowledge support by the DFG Open Access Publication Fund of the Ruhr-Universität Bochum.
