


El sobrepeso y la obesidad son condiciones médicas que requieren un análisis multidisciplinario de sus causas y tratamiento. En Chile se ha observado un aumento sostenido de la presencia de obesidad y sobrepeso en niños. Sin embargo, se desconoce el nivel de presencia y la dinámica de las conductas alimentarias problemáticas mencionadas en niños chilenos. El objetivo de esta investigación fue estudiar la relación entre la alimentación restringida, externa y emocional y las variaciones en el Índice de Masa Corporal (IMC) en niños chilenos. Consecuentemente, 453 niños entre 7 a 12 años respondieron el Cuestionario Holandés de Conducta Alimentaria para niños. Además, se obtuvieron datos antropométricos. Se encontró una relación positiva entre la alimentación restringida y el IMC y una correlación negativa entre alimentación externa y el IMC. La alimentación emocional demostró una relación inversa modesta con el IMC. Se observó una significativa interacción entre la conducta problemática y estado nutricional (normopeso, sobrepeso, obesidad). La alimentación restringida fue característica de los niños con obesidad mientras que la alimentación externa, de los niños con normopeso. Estos resultados sugieren que la conducta alimentaria problemática y su relación con el peso corporal son similares a los estudios descritos en Europa.
Overweight and obesity are medical conditions that require a multidisciplinary analysis of their causes and treatment. In Chile a sustained increase in the presence of obesity and excess weight has been observed in children. However, the amount and the dynamics of the aforementioned problematic eating behaviours in Chilean children are unknown. The aim of this study was to assess the relationship between restrained, external, and emotional eating, and variations in body mass index (BMI) in Chilean children. Consequently, 453 children from 7 to 12 years of age responded to the Children's Dutch Eating Behaviour Questionnaire, Spanish version. In addition, their anthropometric data were obtained. A positive association was found between restrained eating and BMI, and a negative correlation between external eating and BMI. Emotional eating demonstrated a modest inverse relationship with BMI. A significant interaction between problematic behaviour and nutritional status (normal-weight, overweight, obese) was revealed. Restrained eating was characteristic of obese children whereas external eating of normal-weight children. These results suggest that problematic eating behaviours and their relationship with body weight are similar to those described in studies in Europe.
The personal, family, and social consequences of obesity are so high that the need to develop a better understanding of its causes and treatment has been acknowledged (Eckel, 2008). A significant body of evidence indicate to the context as an important factor in the development of weight gain problems in adults and children (Kaur, Hyder, & Poston, 2003; Poston & Foreyt, 1999). It has effectively emphasised that, independently of the genetic influence in the appearance and development of obesity, the presence of certain environmental c onditions has simultaneously favoured excess food intake and a positive energy balance (Poston & Foreyt, 1999). The scientific community has denominated the group of contextual factors that favour excessive weight gain as the "obesogenic environment" (Booth, Pinkston, & Poston, 2005; Poston & Foreyt, 1999), which includes the combination of an environment that requires scarce physical activity with a significant foment of consumption of high energy density foods (i.e., easy access, marketing, etc.). Naturally, individual differences are seen in the consequences of the exposition to an obesogenic environment, and there are people who respond to this context gaining weight while others maintain their body weight in a normal range. For this reason, individual factors, especially problematic eating behaviours, have been increasingly approached in the study of obesity and similar disorders.
In regard to eating behaviours related to weight gain, at least three types of problematic behaviour have been distinguished: external eating, restrained eating, and emotional eating (Van Strien, Frijters, Bergers, & Defares, 1986). As emphasized (Snoek, Van Strien, Janssens, & Engels, 2007; Van Strien & Oosterveld, 2008), each type was initially approached independently by three psychological theories on overeating. However, in the past few years it has been consolidating the idea that these behaviours are not alterations in eating that arise in an orthogonal and/or exclusive way, but rather, they may interact and/or co-exist. More importantly, this type of problematic behaviour shows different patterns of expression throughout life span (Braet et al., 2008; Lluch, Herbeth, Mejean, & Siest, 2000; Van Strien & Oosterveld, 2008).
External eating refers to eating behaviours that are triggered by the external environment (eating cues). "External eaters" are persons who tend to overeat induced by external cues such as the presence of food, its aroma and/ or flavour, and even by the time of day (Van Strien et al., 1986). On the other hand, restrained eating has been related with the recurrent combination of restraint and overeating (Herman & Polivy, 1980). This pattern paradoxically leads to overweight and even to obesity in the long term and, although it is not a clinical syndrome, it might be the precursor to developing eating disorders such as binge eating (Silva, 2007, 2008a, 2008b). Finally, emotional eating is related to eating behaviour arising in response to emotional variations, especially connected to negative feelings (Van Strien et al., 1986). Emotional eaters are persons who tend to alter their food-intake behavior when they experience negative emotions (Borda Mas et al., 2011; Silva, 2008a, 2011; Silva, Ortiz, Quiñones, Vera, & Slachevsky, 2011), pattern also observed in eating disorders (Medina-Pradas, Blas Navarro, Álvarez-Moya, Grau, & Obiols, 2012; Pascual, Etxebarria, Cruz, & Echeburúa, 2011).
When the set of problematic eating behaviours in the general population is considered, emotional eating and restrained eating in adults has been observed to modulate the relationship between overeating and overweight (Van Strien et al., 2009). External eating, however, does not seem to play a relevant role in this association. van Strien and collaborators (Van Strien, Herman, & Verheijden, 2009) sustain that if previous studies are taken into consideration, emotional eating seems to have increased noticeably in the past years, partially explaining the continual increase in the presence of obesity in the population. In this context, as will be described in the following section, there is a growing interest in discovering the influence of the problematic behaviour in weight gain in infants, children, and adolescent populations.
Thanks to the recent development of the Dutch Eating Behaviour Questionnaire in its version for children from 7 to 12 years of age (Van Strien & Oosterveld, 2008), analysis has been able to progress on the relationship between the set of different forms of problematic eating behaviour and the alterations of body weight in children. In the seminal study by van Strien and Oosterveld (Van Strien & Oosterveld, 2008), unlike that observed in adults, there was a low prevalence of emotional eating in Dutch children. Likewise, in overweight children there was a predominance of restrained eating.
Another study (Braet et al., 2008), using the DEBQ-C in Belgian children and adolescents, also revealed that restrained eating is predominant in those overweight participants. At the same time, the children presented a much-diminished presence of emotional eating while it was more relevant in adolescence. Similar findings have been reported in Italy, employing the parents version of the DEBQ (Caccialanza et al., 2004), in which restrained eating seemed to predominate in overweight and obese preadolescents. Likewise, in the Stanislas Family Study (France) (Lluch et al., 2000) a positive relationship was described between restrained eating and body weight along with a negative correlation of the latter with external eating. Emotional eating, again, did not show an important presence nor did it show a relationship to the body mass index (BMI).
In Chile and in Latin America in general, there is currently no report in regard to the different eating styles and body weight in children. It has been emphasized that the epidemiological transition of Chile has favoured the increase of obesity and excessive weight in all age groups (Albala, Vio, Kain, & Uauy, 2002; Kain, Lera, Rojas, & Uauy, 2007; Vio, Albala, & Kain, 2008). However, it is unknown whether this socio-cultural environment, which has modulated the population's nutritional status, has modified the aforementioned behavioural aspects. This is not a trivial point considering that cultural factors that model eating behaviour seem to be very relevant in both the conformation of excessive weight and obesity as well as in its treatment (Davis, Northington, & Kolar, 2000; Kumanyika, 2008). Bearing in mind the above information, it is important to learn whether the relationship between problematic eating behaviours and body weight, established in studies in Europe, can be applied to subjects from other cultural contexts, particularly Chile.
This study, therefore, intends to determine the presence of problematic eating behaviours (external, restrained and emotional eating) in Chilean children from 7 to 12 years of age and its relationship with body weight. Additionally, unlike prior studies, we intend to analyse these relationships considering the nutritional status of the participants in three levels: normal weight, overweight, and obese. In fact until now, prior studies that mploy the DEBQ-C have made comparisons of groups taking into consideration the normal weight/overweight dichotomy, without differentiating between those who are overweight and those who are obese in the latter group of participants. This differentiation could provide evidence of degrees of difference in the variations of the variables studied. Thus, different age ranges (7-8; 9-10; 11-12), three socioeconomic levels (low, middle, and high) and the nutritional status (normal, overweight, obesity) will be taken into account.
Method
Participants
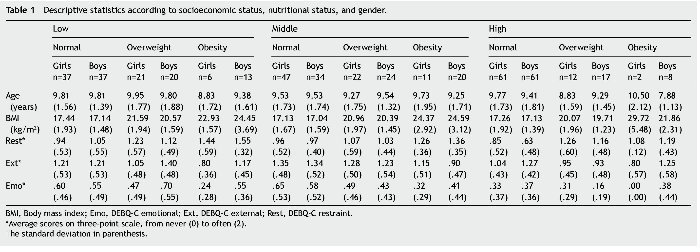
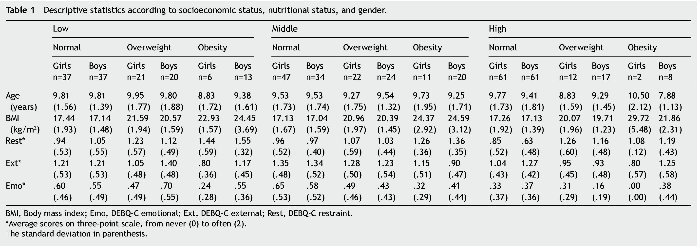
By means of a probabilistic sampling method, 453 children from the ages of 7 to 12 were selected from different socioeconomic levels (high, middle, low)1 in the city of Santiago, Chile, who participated in a cross-sectional descriptive study (Montero & León, 2007) with the informed consent of the parents and children. The sample was made up of 234 girls (51.7%) and 219 boys (48.3%), with an average of 9.54 years of age (SD = 1.68) and average BMI of 18.99 kg/m2 (SD = 3.18). 61.1% of the children (n = 277) presented normal weight, 25.6% (n = 116) were overweight, and 13.2% (n = 60) were obese (see Table 1).
Instruments
Dutch Eating Behaviour Questionnaire for 7 to 12 year old children (DEBQ-C) (Van Strien & Oosterveld, 2008): The DBEQ-C is a questionnaire adapted to age (7 to 12 years old), which assesses the presence of External Eating, Emotional Eating, and Restrained Eating. It is a self-applied questionnaire composed of 20 Likert type questions.
• Anthropometric data: The anthropometric data were obtained individually by a psychologist who measured and weighted each child. To obtain the most precise measurement, each child was measured and weighed barefoot, wearing trousers/skirt and shirt only. This measurement was carried out in a private room, after the application of the DEBQ-C. Using the Chilean Standards (Pizarro, Rodríguez, & Benavides, 2004) the total sample was divided into children with normal weight, overweight, and obesity. The "overweight" group was made up by all those children whose BMI was equal to or above the 85th percentile and lower than the 95th percentile, according to gender and age. Following the same guidelines, obesity was defined based on a BMI equal to or above the 95th percentile (see Table 1).
Procedure
• Translation: The Spanish version of the DEBQ-C was obtained through a translation/back-translation process. First, a direct translation of the instrument was done, where a group of bilingual experts translated the instrument from the source language (English) to the target language (Spanish) (translation). Subsequently, for the purpose of assessing the equivalency between the two versions of the questionnaire and to detect possible translation problems of some items, another group of translators translated this Spanish version back into English (back-translation). The author of the original instrument approved the final version.
• Pilot test: A pilot test of the DEBQ-C was applied to a sample of 18 children from 7 to 12 years of age. This test took three socio-economic levels into consideration, assessing 6 children from each level (high, middle, low). The objective of this pilot test was to determine the level of comprehension of the instrument, especially in younger children (7 and 8-years-old). Based on this experience, as in the original study, it was decided that the most appropriate method was to read the questions and statements of the questionnaire to the 7 and 8-year-old children.
• Application of the DEBQ-C: The application of the definitive version of the questionnaire was carried out collectively in three schools according to socioeconomic status. For the 7 to 8 year old children, a research assistant read the questionnaire together with the children and gave examples when required.
Results
Psychometric properties of the Spanish-language version of the DEBQ-C
The Spanish version of the DEBQ-C obtained Cronbach's alpha of .72, similar to the original report (van Strien and Oosterveld, 2008). Upon analysing the correlation between each item and the total sub-scale, a corrected homogeneity index of .30 (Kline, 1999) was considered acceptable. Using these criteria, the items 4 and 10 were excluded from the rest of the analysis and from the study in general. Likewise, a Principal Components Analysis extracted 3 linear components in the data (eigenvectors), which self-values (eigenvalues) in the R-matrix were equal to or greater than 1. These components explained 42.4% of the total variance. The oblique rotation also results in a structure of three factors, being grouped according to the original Restrained, External, and Emotional Eating factors (Van Strien & Oosterveld, 2008).
1. The central aim of this study was not to analyse the influence of SES. This analysis is part of an additional project and therefore this variable is not described in greater detail.
Correlations between pertinent variables
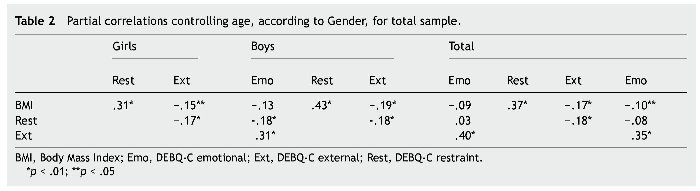
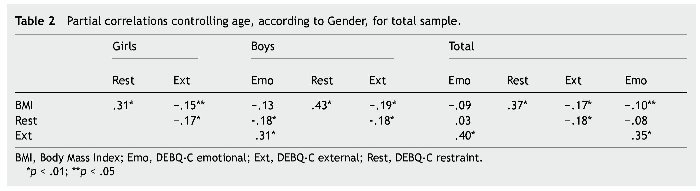
For the purpose of a preliminary assessment of the relationship between some of the relevant variables, a set of partial correlations (controlling for age) was carried out between the different types of eating (emotional, external, and restrained), the total score of the DEBQ-C, and BMI (see Table 2).
The association of the socioeconomic status, age range, and gender, and the different types of eating (Emotional, External, and Restrained)
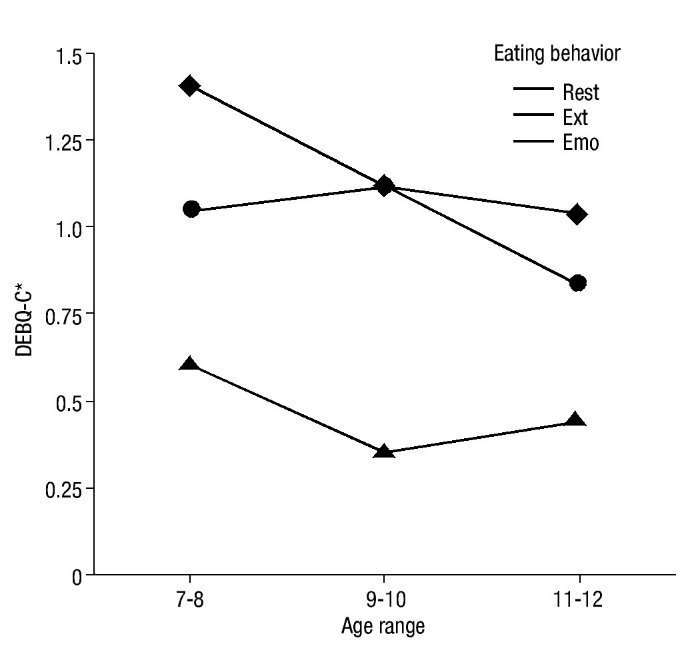
As a first analysis, the different types of eating were compared according to socioeconomic status (SES), age range (AR) and gender. Thus, a 3x2x3x3 mixed ANOVA, with SES (low, middle, high), AR (7-8, 9-10, 11-12) and Gender (female, male) as a between-factor variable and Eating (Emotional, External, Restrained) as a repeated measure, was carried out on the response averages of the DEBQ-C. Given the correlation of the variables from the repeated measure, and therefore not complying with the compound symmetry test, Pillai's trace was used in the multivariate test to evaluate the main effects and interactions. The tests of within-subject effects reveal an Eating x AR interaction (F(4, 435) = 9.50; p < .001; power = 1.0; η2p = .04), and a significant interaction between Eating, SES, and Gender (F(8, 435) = 2.36; p < .53; power = .50; η2p = .01). These interactions will be assessed separately below. To explore the differences by AR, a repeated measure ANOVA was done on the DEBQ-C scores for each age range, with Eating (emotional, external, restrained) as within-subject factor. For the 7-8 year old range, a significant within-subject effect (Greenhouse Geisser as correction) was obtained for Eating (F(1.90, 143) = 106.34; p < .001; η2p = .43). The within-subject contrasts demonstrate that external eating is greater than restrained eating (F = 37.28; p < .001; η2p = .21) and, at the same time, greater than the emotional eating (F = 59.49; p < .001; η2p = .29). On the other hand, for the 9-10 year old range, a significant within-subject effect (Greenhouse Geisser as correction) was also obtained for Eating (F(1.62, 157) = 156.28; p < .001; η2p = .50). However, the within-subject contrasts in this age range do not display differences between external and restrained eating (p > .949), although the difference from emotional eating is maintained (F = 217.89; p < .001; η2p = .58). Finally, for the 11-12 year old range, a significant within-subject effect (Greenhouse Geisser as correction) was again obtained for Eating (F(1.64, 152) = 54.58; p < .001; η2p = .27). In this group, the within-subject contrasts show that external eating differs from restrained eating (F = 8.95; p < .001) but on a small scale (η2p = .056). Likewise, restrained eating is greater than emotional eating (F = 41.895; p < .001; η2p = .22) (see Fig.1). The interaction of Eating, SES, and Gender, was explored in each SES by means of a mixed ANOVA, with Gender (female, male) as between-subject variable and Eating (emotional, external, restrained) as repeated measure. Only in the high SES were differences found in the type of eating depending on the gender. Specifically, a significant Gender x Eating interaction (Pillai's trace) was observed (F(2, 161) = 4.95; p < .05; η2p =.06), where the post-hoc comparisons demonstrate that boys present slightly higher external eating than girls (post hoc t test; DEBQ-C/EXT: p < .01)2.
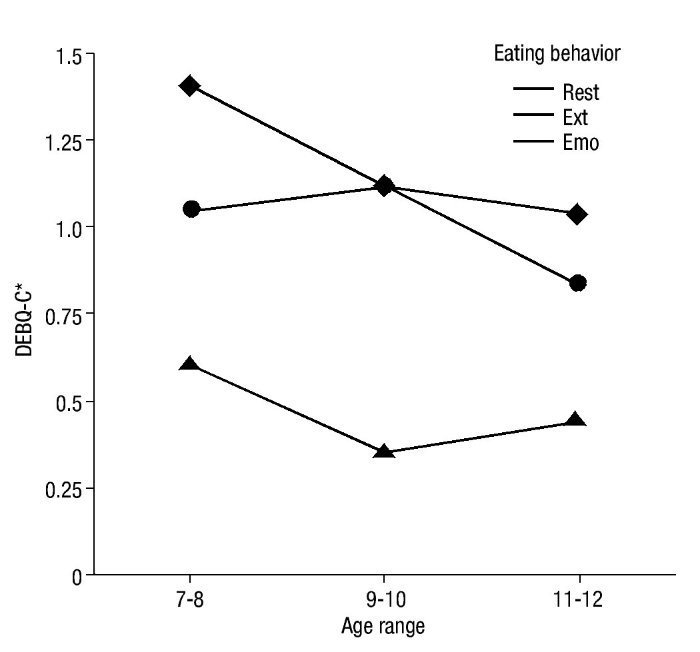
Figure 1 Problematic eating behaviours for the total sample according to age range. DEBQ-C, Children's Dutch Eating Behaviour Questionnaire; Emo, DEBQ-C emotional; Ext, DEBQ-C external; Rest, DEBQ-C restraint. *Average scores on three-point scale, from never (0) to often (2). See text for significant between and within-group differences.
2. Multilevel analytic modelling (e.g., hierarchical linear modelling) would probably provide an account in greater depth of the association of SES and eating behaviours. However, this study does not aim to emphasise this influence in detail, which forms part of an additional project.
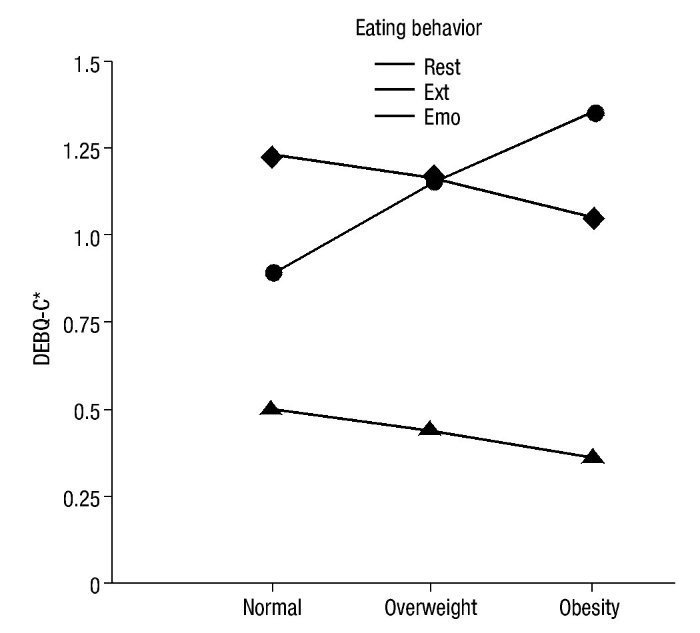
Association between nutritional status and eating behaviour
A mixed ANOVA with Weight (normal weight, overweight, and obesity) as between-factor and Eating (emotional, external, and restrained) as repeated measure was done over the DEBQ-C scores. The within-subject effects test (Pillai's trace) showed a significant Eating x Weight interaction (F(4,453) = 12.02, p < .001; power = 1.00; η2p = .05). As observed in Fig. 2, the type of eating that shows the greatest variation throughout the weight categories is restrained eating. A growing tendency in eating restraint can clearly be observed as the weight increases. To explore these observations, an ANOVA with Weight (normal weight, overweight, and obesity) as between-factor was done on the restrained eating scores. The between-subject effects test was significant (F(2, 453) = 27.86, p < .001; η2p = 0.11), while the post-hoc tests (Dunnet) reveal that restrained eating is greater in the obesity group than in the overweight group (p < .01) and then in the normal weight group (p < .001). In addition, the polynomial contrast test shows that restrained eating adopts a growing linear tendency throughout the weight categories (p < .001).
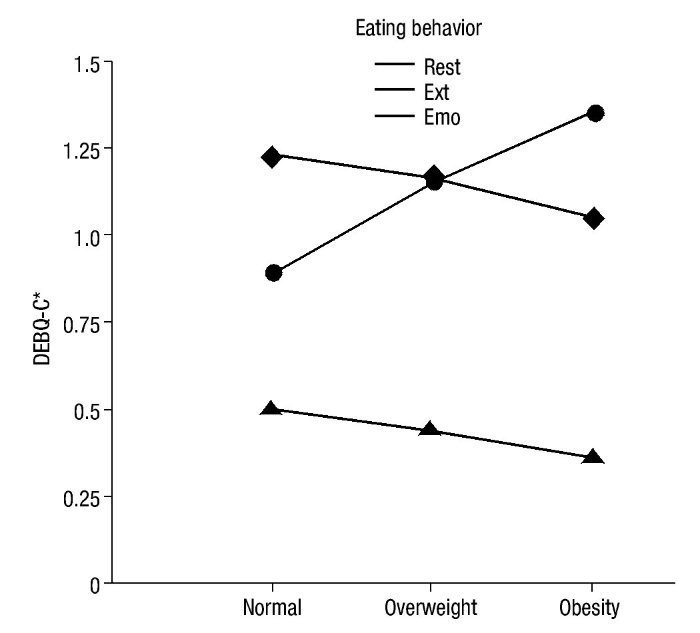
Figure 2 Problematic eating behaviours according to nutritional status of total sample. DEBQ-C, Children's Dutch Eating Behaviour Questionnaire; Emo, DEBQ-C emotional; Ext, DEBQ-C external; Rest, DEBQ-C restraint. *Average scores on three-point scale, from never (0) to often (2). See text for significant between and within-group differences.
Association between nutritional status, overconsumption, gender and eating behaviour
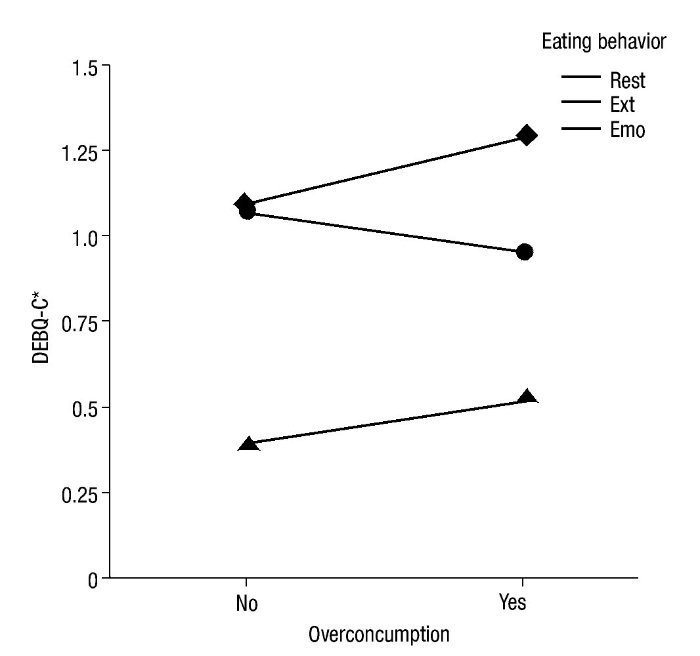
Overconsumption behaviour was assessed following a similar strategy as in prior studies (Van Strien et al., 2009). Specifically, through the responses (Yes vs. No) to the question included in the questionnaire "Have you ever eaten a quantity of food that other people consider unusually large?", two groups were obtained (Overconsumption and non-Overconsumption). In this context, to evaluate the effect of nutritional status, overconsumption and gender on the type of eating, a 3x2x2x3 mixed ANOVA, with Weight (normal weight, overweight, obesity) Overconsumption (absent, present) and Gender (female, male) as between-factor variable, and Eating (Emotional, External, Restrained) as repeated measure, was carried out on the scores of the DEBQ-C scale. Significant results were only obtained (Pillai's trace) for the Eating x Overconsumption interaction (F(2,435) = 7.60, p < .001; power = .945; η2p = .03). The post-hoc t contrasts show that external eating is greater in children who present overconsumption behaviour (p < .001), compared with those who did not (p < .015). Likewise, in this group, external eating was significantly greater than restrained eating (paired t; EX/REST: p < .001) and emotional eating (paired t; EX/EMO: p < .001). Thus, in children that present overconsumption, external eating pattern prevails over restrained eating (see Fig. 3).
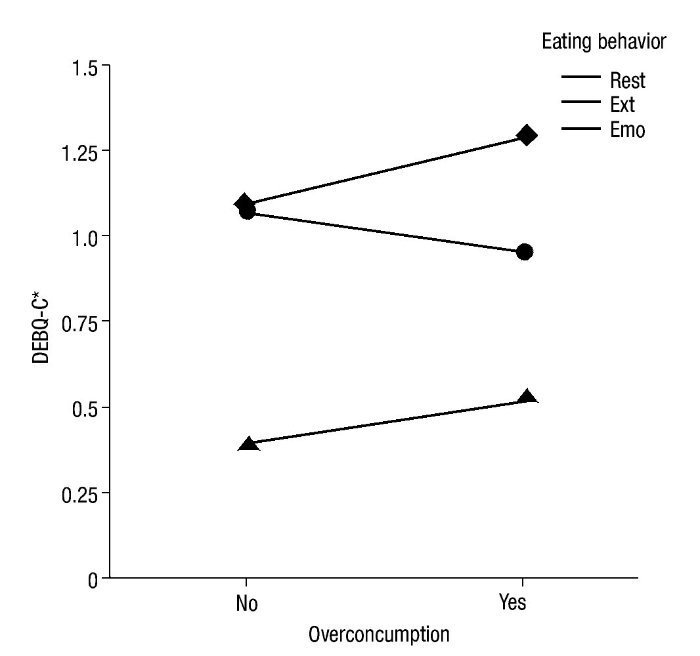
Figure 3 Problematic eating behaviours and over-eating for the total sample. DEBQ-C, Children's Dutch Eating Behaviour Questionnaire. Emo, DEBQ-C emotional; Ext, DEBQ-C external; Rest, DEBQ-C restraint. *Average scores on three-point scale, from never (0) to often (2). See text for significant between and within-group differences.
Discussion
The results of the study in 7 to 12 year old Chilean children suggest that the presence and dynamics of problematic eating behaviours are similar to those described in Europe. As will be described below, a set of observations is concordant with previous evidence.
In the first place, a positive association between restrained eating and the BMI was found, as well as a negative correlation between external eating and the BMI. Both relationships have been consistently reported (Braet et al., 2008; Lluch et al., 2000; Snoek et al., 2007; Van Strien et al., 2009; Van Strien & Oosterveld, 2008), being the source of theoretical discussions. Although the restraint theory predicts that people with restricted eating habits will recurrently overeat and gaining weight over the long term (Silva, 2008a), restraint is associated with overweight but not with overeating (Lluch et al., 2000; Snoek, Van Strien, Janssens, & Engels, 2008). Van Strien has emphasized that DEBQ's restraint factor is a pure restriction measurement, while other instruments (such as the Revised Restraint Scale) tend to assess those persons that are not successful in sustaining a diet (Van Strien, 1999). In any case, in this study the same phenomenon was observed, that is, that restraint was associated with overweight and obesity, while overconsumption was predominant in children with higher levels of external eating. The theory of externality has also been questioned due to the described observations (Snoek et al., 2007). In so far as behaviour is orientated towards contextual cues, an increase in consumption is expected and therefore a relative increase in the BMI. Even when the first is correct, external eating predicts a lower BMI in children. Upon considering the nutritional status categories, a simple explanation can be outlined. The data indicates that the normal weight group shows a predominant pattern of eating behaviour, which is opposite to the obese group.
Specifically, in normal weight children there is a prevalence of external eating above restrained eating while the opposite occurs in obese children (see Fig. 2). Likewise, in the total sample, a significant negative correlation is observed between external and restrained eating. Considering this dynamic variation, it could be suggested that external eating behaviour seems to represent a normal tendency in children that tends to diminish with excessive weight due to the modulation of restrained behaviour. In this manner, in obese children the external eating tendencies would be conditioned by an inhibitory control of the restraint. Van Strien has emphasized this perspective sustaining that external eating could represent an adaptive behaviour from an evolutionary point of view (Van Strien et al., 2009), and correspond to the normal eating pattern in 7 to 12 year old children. In this context, other variables could induce weight gain and, therefore, restraint would only reflect a socially favoured behaviour for the regulation of body weight. In fact some authors have proposed that the problem of restrained eating would be a behaviour belonging to people with sensitivity to weight gain (Lowe & Kral, 2006). Even so, as emphasized by Braet and collaborators (Braet et al., 2008), it is necessary to explain why the relationship between the different types of eating and its impact on the BMI acquire other configurations starting in adolescence and in adulthood.
Secondly, emotional eating appears not to be relevant in the eating behaviour of 7 to 12 year old Chilean children. This finding has also been previously observed and it is one of the findings that have most intrigued researchers (Braet et al., 2008; Van Strien & Oosterveld, 2008). Although in adults there seems to be a significant increase in the presence of emotional eating in the past decades (Van Strien et al., 2009), with body weight also having an impact, this type of behaviour seems not to have an important influence on weight nor on eating habits in children. In fact in this study, in the total sample (and marginally significant in girls, p = .06), a modest inverse relationship was observed between the BMI and this type of eating (see Table 2). This could be due to two phenomena: a) it is possible that eating problems associated with emotional changes arise in stages subsequent to childhood and adolescence (Snoek et al., 2007), or: b) due to lack of superior cognitive capacities (associated with maturing of the brain) which are required for elaboration of a complex emotional experience representation (Lewis & Carmody, 2008), it is very probable that children are incapable of establishing (and reporting) a relationship between the two elements, even when it is substantially present.
Finally, with regard to external eating, various previously described relationships were found (Braet et al., 2008; Van Strien & Oosterveld, 2008). As mentioned, external behaviour was associated with overconsumption. Likewise, it was observed that boys showed more external eating behaviour than girls, although this was only statistically significant for the high SES. Moreover, external eating was positively correlated with emotional eating. This association could imply that external eating and emotional eating operate jointly in facilitating overeating (Van Strien & Oosterveld, 2008). Even so, we should not lose sight of the low presence of emotional eating throughout the different age groups.
One aspect not described in other studies, and pertinent for this discussion, refers to the relationship between external eating and restrained eating in correspondence to the age ranges (see Fig. 1). In this context, it was observed that dynamic relationship exists between external and restrained eating. As stated above, there is a tendency towards a decrease of external eating throughout development, with the 7-8 year old group demonstrating greater external eating than the 11-12 year old group (t(294) = 6.69; p < .001). In this context, it could be suggested, as an explanation to demonstrate in future studies, that external eating decreases with age as the children improve their intentional self-regulation abilities. Thus, the exacerbation of external eating behaviours would be an alteration or a behaviour problem, only starting at adolescence and in adulthood.
The limitations of the study are multiple. Principally, its correlational nature and the obtaining of behavioural data based on self-reporting by children significantly restrict the validity of the asseverations and hypotheses offered. In effect, the direction of the causality cannot be established in a trustworthy manner and it is also unknown whether the intentions of behaviours in children (self-reporting) can be translated into equivalent behaviour. In fact, recent studies have questioned the validity of psychometric measurements of restrained eating (Stice, Cooper, Schoellet, Tappe, & Lowe, 2007; Stice, Fisher, & Lowe, 2004) and external eating (Jansen et al., 2011). In addition, one major concern is that the youngest group received the DEBQ in an interview-like format. This is likely to entirely account for the age effects seen in this study and in the original DEBQ-C report. Younger children within an interview format are perhaps more likely to respond affirmatively because they think this is what the experimenter wants, or perhaps because they understand what they question is better than those children doing the questionnaire version, because they are given verbal examples. Although the information obtained by comparable studies has been of enormous value, it is necessary to implement studies that objectively assess the problematic behaviours discussed herein.
As previously emphasised, there is an urgent need to improve scientific knowledge of the distal and proximal causes of the problem of excess weight in children and adults. In this context, this study suggests that the dynamics of the factors associated with behaviours of restrained, external, and emotional eating occurs in Chile in the same way as in studies carried out in Europe and the United States. In the future it would be interesting to learn, as could be deduced from the described findings, whether the emergence of problematic eating behaviour in obesogenic socio-cultural contexts follows certain universal principles.
Funding
Research financed by Dirección de Investigación de la Universidad de La Frontera (DIUFRO) and FONDECYT 11090162. The authors thank two anonymous reviewers for valuable comments and suggestions.
*Corresponding author at:
Departamento de Salud Mental y Psiquiatría,
Facultad de Medicina, Universidad de La Frontera, Manuel Montt, 112, Temuco,
Región de la Araucanía, Chile.
E-mail address:jaimesilva@ufro.cl (J.R. Silva).
Received May 3, 2012;
accepted September 14, 2012
References
Albala, C., Vio, F., Kain, J., & Uauy, R. (2002). Nutrition transition in Chile: determinants and consequences. Public Health Nutrition, 5, 123-128.
Booth, K. M., Pinkston, M. M., & Poston, W. S. (2005). Obesity and the built environment. Journal of the American Diet Association, 105 (suppl.), S110-117.
Borda Mas, M., Avargues, M. L., López, A. M., Torres, I., Del Río, C., & Pérez, M. A,. (2011). Personality traits and eating disorders: Mediating effects of self-esteem and perfectionism. International Journal of Clinical and Health Psychology, 11, 205-227.
Braet, C., Claus, L., Goossens, L., Moens, E., Van Vlierberghe, L., & Soetens, B. (2008). Differences in eating style between overweight and normal-weight youngsters. Journal of Health Psychology, 13, 733-743.
Caccialanza, R., Nicholls, D., Cena, H., Maccarini, L., Rezzani, C., Antonioli, L., Dieli, S., & Roggi, C. (2004). Validation of the Dutch Eating Behaviour Questionnaire parent version (DEBQ-P) in the Italian population. European Journal of Clinical Nutrition, 58, 1217-1222.
Davis, S. P., Northington, L., & Kolar, K. (2000). Cultural considerations for treatment of childhood obesity. Journal of Cultural Diversity, 7, 128-132.
Eckel, R. H. (2008). Obesity research in the next decade. International Journal Obesity (Lond), 32 (suppl.), S143-151.
Herman, C.P., & Polivy, J. (1980). Restrained Eating. In A. Stunkard (Ed.), Obesity(pp. 208-225). Philadelphia: Saunders.
Jansen, A., Nederkoorn, C., Roefs, A., Bongers, P., Teugels, T., & Havermans, R. (2011). The proof of the pudding is in the eating: Is the DEBQ-external eating scale a valid measure of external eating? International Journal of Eating Disorders, 44, 164-168.
Kain, J., Lera, L., Rojas, J., & Uauy, R. (2007). Obesity among preschool children of Santiago, Chile. Revista Médica de Chile, 135, 63-70.
Kaur, H., Hyder, M. L., & Poston, W. S. (2003). Childhood overweight: An expanding problem. Treatment in Endocrinology, 2, 375-388.
Kline, P. (1999). The handbook of psychological testing. London: Routledge.
Kumanyika, S. K. (2008). Environmental influences on childhood obesity: Ethnic and cultural influences in context. Physiology & Behavior, 94, 61-70.
Lewis, M., & Carmody, D. P. (2008). Self-representation and brain development. Developmental Psychology, 44, 1329-1334.
Lluch, A., Herbeth, B., Mejean, L., & Siest, G. (2000). Dietary intakes, eating style and overweight in the Stanislas Family Study. International Journal of Obesity, 24, 1493-1499.
Lowe, M. R., & Kral, T. V. (2006). Stress-induced eating in restrained eaters may not be caused by stress or restraint. Appetite, 46, 16-21.
Medina-Pradas, C., Blas Navarro, J., Álvarez-Moya, E., Grau, A., & Obiols, J. E. (2012). Emotional theory of mind in eating disorders. International Journal of Clinical and Health Psychology, 12, 189-202.
Montero, I., & León, O. G. (2007). A guide for naming research studies in Psychology. International Journal of Clinical and Health Psychology, 7, 847-86.
Pascual, A., Etxebarria, I., Cruz, M. S., & Echeburúa, E. (2011). Las variables emocionales como factores de riesgo de los trastornos de la conducta alimentaria. International Journal of Clinical and Health Psychology, 11, 229-247.
Pizarro, T., Rodríguez, L., & Benavides, X. (2004). Technical norm for the nutritional evaluation of children aged 6 to 18 years old. Year 2003. Revista Chilena de Nutrición, 31, 11-30.
Poston, W. S., & Foreyt, J.P. (1999). Obesity is an environmental issue. Atherosclerosis, 146, 201-209.
Silva, J. R. (2007). Sobrealimentación inducida por la ansiedad, Parte I: Evidencia conductual, afectiva, metabólica y endocrina. Terapia Psicológica, 25, 112-134.
Silva, J. R. (2008a). Restricción alimenticia y sobrealimentación: Un modelo de la neurociencia afectiva. Revista Médica de Chile, 136, 1336-1342
Silva, J. R. (2008b). Sobrealimentación inducida por la ansiedad, Parte II: Un marco de referencia neurocientífico para el desarrollo de técnicas psicoterapéuticas. Terapia Psicológica, 3, 99-115.
Silva, J. R. (2011). Restraint eating and sensitivity to stress: Preliminary experimental evidence. Rivista di Psichiatria -Roma, 46, 300-304.
Silva, J. R., Ortiz, M., Quiñones, A., Vera, P., & Slachevsky, A. (2011). Affective style and eating disorders: A field study. Eating and Weight Disorders. Studies on Anorexia, Bulimia & Obesity, 16, 73-80.
Snoek, H. M., Van Strien, T., Janssens, J. M., & Engels, R. C. (2007). Emotional, external, restrained eating and overweight in Dutch adolescents. Scandinavian Journal of Psychology, 48, 23-32.
Snoek, H. M., Van Strien, T., Janssens, J. M., & Engels, R. C. (2008). Restrained eating and BMI: A longitudinal study among adolescents. Health Psychology, 27, 753-759.
Stice, E., Cooper, J. A., Schoeller, D. A., Tappe, K., & Lowe, M. R. (2007). Are dietary restraint scales valid measures of moderate-to long-term dietary restriction? Objective biological and behavioral data suggest not. Psychological Assessment, 19, 449-458.
Stice, E., Fisher, M., & Lowe, M. R. (2004). Are dietary restraint scales valid measures of acute dietary restriction? Unobtrusive observational data suggest not. Psychological Assessment, 16, 51-59.
Van Strien, T. (1999). Success and failure in the measurement of restraint: notes and data. International Journal of Eating Disorders, 25, 441-449.
Van Strien, T., Frijters, J. E., Bergers, G. P., & Defares, P. B. (1986). The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. International Journal of Eating Disorders, 5, 747-755.
Van Strien, T., Herman, C. P., & Verheijden, M. W. (2009). Eating style, overeating, and overweight in a representative dutch sample. Does external eating play a role? Appetite, 52, 380-387.
Van Strien, T., & Oosterveld, P. (2008). The children's DEBQ for assessment of restrained, emotional, and external eating in 7-to 12-year-old children. International Journal of Eating Disorders, 41, 72-81.
Vio, F., Albala, C., & Kain, J. (2008). Nutrition transition in Chile revisited: mid-term evaluation of obesity goals for the period 2000-2010. Public Health Nutrition, 11, 405-412.
