





An increasing number of studies support the beneficial relationship between physical activity and stress coping in people with multiple sclerosis (MS). However, there has been limited understanding of the variables that may influence the nature of this relationship. Therefore, based on the social-cognitive framework and previous research, we aimed to examine the association between the habitual physical activity of people with MS and their coping effectiveness. Furthermore, we sought to determine the extent to which self-efficacy acts as a mediator in this relationship, considering the level of disability as a moderator variable.
MethodsIn this cross-sectional study, a total of 351 people with MS participated. The participants were asked to complete several assessment tools, including the Mini-COPE Inventory for Measurement—Coping with Stress, the Generalized Self-Efficacy Scale, and the Godin Leisure-Time Exercise Questionnaire. Additionally, a neurologist assessed the severity of the disease using the Expanded Disability Status Scale. Information on the demographic and clinical characteristics of the participants was collected via a self-report survey. Two moderated mediation analyses were conducted as part of the study.
ResultsThe study findings indicated a positive correlation between engagement in physical activity and self-efficacy among participants with high and medium disability levels. This, in turn, demonstrated a positive association with effective stress-coping strategies and a negative association with ineffective coping methods. In particular, a significant relationship was observed between involvement in physical activity and self-efficacy in participants with high disability, while it was not statistically significant in participants with low disability.
ConclusionPhysical activity was associated with improved psychosocial functioning in people with high levels of disability caused by MS. This association may be attributed to factors such as increased self-efficacy and improved stress coping. However, the relationship between physical activity and psychosocial functioning was less evident in people with low disability caused by MS.
Multiple sclerosis (MS) is a progressive neurodegenerative disease characterized by unpredictability, limited control options, a wide range of symptoms, and uncertain treatment possibilities. These factors contribute to an increased risk of mental health problems. Research has shown that the mental health of people with MS is significantly worse compared to that of the general population (Feinstein, 2011; Marrie et al., 2015). Recent meta-analyses have indicated that the prevalence of depression and anxiety in people with MS is 30.5 and 22.1 %, respectively (Boeschoten et al., 2017). In order to cope with the challenges of daily life and maintain mental health, people with MS need to tap into personal resources that improve their stress-coping abilities.
Coping is defined as a set of behavioral and psychological strategies employed to master, tolerate, reduce, or minimize stress in certain situations (Lazarus & Folkman, 1984). Various stress-coping strategies exist, and the literature mainly distinguishes between adaptive strategies (primarily problem-solving) and maladaptive strategies (emotional and avoidance) (Pakenham, 1999). Research indicates that people with MS more frequently employ less favorable strategies, relying on emotions and avoidance rather than actively addressing problems and approaching challenges constructively (Goretti et al., 2009; Grech et al., 2018). Since emotional and avoidance strategies are considered less effective, they often contribute to disruptions in mental functioning (Bassi et al., 2019; Wilski et al., 2019).
Studies aimed at improving the mental functioning of people with MS should mainly focus on searching for factors that improve the effectiveness of coping with stress. Physical activity is one such factor that may be beneficial. Numerous scientific studies have established a relationship between physical activity and the utilization of more effective coping strategies, both in people without health conditions (Biddle & Asare, 2011; Kim & McKenzie, 2014; Perchtold‐Stefan et al., 2020; Xu & Zhang, 2020) and those with disabilities (Kim et al., 2021; Stephens et al., 2012). In a study involving people with MS, it was noted that those who were less active faced considerable difficulties in coping with the stress associated with exercise. The authors propose that this difficulty could be attributed to a higher tendency to employ avoidance or emotional coping strategies (Mezini & Soundy, 2019).
Although intervention studies conducted with both patients and nonclinical populations have highlighted the beneficial effects of physical activity on mental health and coping, the specific mechanisms underlying this relationship remain unclear. One hypothesis proposes that physical activity improves coping by enhancing self-efficacy, which refers to an individual's belief in their ability to accomplish a specific task and reflects their confidence in coping with challenging, demanding, or limiting situations (Bandura, 2012). Existing literature connects self-efficacy levels with physical activity in the general MS population (Baird et al., 2022; Casey et al., 2017; Streber et al., 2016). According to Bandura's Social Cognitive Theory (Bandura, 1995), the associations between personal factors such as self-efficacy and behaviors such as physical activity are bidirectional. Nevertheless, studies suggest that engaging in physical activity contributes to the development of self-efficacy (McAuley & Blissmer, 2000). Regular participation in physical activity is likely to enhance an individual's self-efficacy in managing daily activities and disease symptoms (Rejeski & Mihalko, 2001).
Building on this path, improved self-efficacy enables a person to cope better with stressful events. A study by Wilski et al. (2021b) involving a sample of 382 MS patients revealed the highest level of self-efficacy among “Problem Copers” and the lowest level among “Emotion Copers,” aligning with theoretical assumptions and earlier findings from studies conducted on different groups of patients (Benyon et al., 2010; Fuochi & Foà, 2017). This suggests that individuals’ confidence in their abilities is associated with greater utilization of active, problem-solving strategies and a lesser reliance on emotional coping strategies.
The abovementioned relationships may be conditioned by many factors associated with individual differences and the impact of the disease. Among these factors, the level of disability is often highlighted as a variable that can modify the level of physical activity, self-efficacy, and coping strategies for managing stress. For example, Koring et al. (2012) suggest that greater functional limitations caused by MS may strengthen the association between physical activity level and self-efficacy, as confidence is most strongly linked to behavior in challenging situations. When individuals successfully exhibit a behavior under difficult physiological circumstances, their mastery and self-efficacy are enhanced (Bandura, 2012). These results are supported by Vanner et al. (2008), who examined a sample of 43 persons with moderate-to-severe MS, with an Expanded Disability Status Scale (EDSS) score of 6.0–8.0, and reported that high levels of general self-efficacy are associated with high levels of physical activity.
However, conflicting data exist regarding the relationship between disability level and coping strategies. Some studies indicate that higher disability is associated with depression in patients with MS, as they tend to apply less adaptive emotion-centered coping strategies (Kroencke & Denney, 1999; Mohr et al., 1997). Such coping strategies have been negatively associated with adjustment (Pakenham, 1999), quality of life (McCabe, 2006), and the level of self-management (Wilski et al., 2021a). On the other hand, a recent study examining coping profiles of MS patients found no differences in coping styles based on disease severity, as measured by the EDSS, and duration (Wilski et al., 2021b). The authors of the study concluded that coping is independent of the disease state, challenging the assumption that disease severity influences coping styles (Montel & Bungener, 2007).
Overall, a growing number of studies support the beneficial relationship between physical activity and stress coping in people with MS. However, there is still a limited understanding of the variables that may influence this relationship, such as self-efficacy and disability level. Therefore, based on the social-cognitive framework and previous research, our study aims to examine whether individuals’ habitual physical activity is associated with their coping efficiency and the extent to which self-efficacy acts as a mediator in this relationship, considering the level of disability as a moderator variable. According to this, we propose two research questions: First, is the mediating effect of self-efficacy on the relationship between physical activity and effective stress-coping strategies dependent on the level of disability? Second, is the mediating effect of self-efficacy on the relationship between physical activity and ineffective stress-coping strategies dependent on the level of disability? It can be assumed that engaging in physical activity may be particularly important for patients with high levels of disability, where their motor abilities play a significant role. Therefore, we hypothesize that the mediating relationships being analyzed, which involve the significance of physical activity, may be stronger among people with more severe disabilities.
Materials and methodsParticipants and proceduresThe study sample comprised 351 people with MS who were recruited in collaboration with three rehabilitation centers in Poland between January 2021 and January 2022. The inclusion criteria were as follows: (1) a confirmed diagnosis of definite MS by a neurologist based on the revised McDonald criteria (Polman et al., 2011); (2) absence of relapse within 30 days before enrollment; (3) absence of other medical conditions, including psychotic disorders, as identified by the Diagnostic and Statistical Manual of Mental Disorders, version V (DSM-V); and (4) absence of MS-related cognitive problems. A member of the research team recruited the participants during their clinic visit, providing verbal instructions and explaining the study's purpose. Individuals who expressed interest in participating were asked to provide written informed consent. The study was conducted by ethical standards outlined in the Declaration of Helsinki, and participants were assured that their data would be treated confidentially. The questionnaires were completed by the participants in a designated quiet room dedicated to the study. A total of 375 patients responded to the questionnaire, but 24 of them were excluded due to incomplete data. The accuracy of the questionnaire responses was verified upon receipt of the completed forms. Individuals who provided incomplete data were contacted and asked to fill in any potentially significant gaps in their responses. This measure was taken to ensure the completeness and accuracy of the data used for analysis. The study received ethical approval from the Bioethical Commission of Poznan University of Medical Science. Furthermore, the study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist, ensuring comprehensive reporting of the observational study.
MeasuresAll research tools utilized in the study had undergone standardization and validation in many previous studies involving various patient groups, including people with MS. The coping strategies of the participants, which served as the dependent variable in this study, were assessed using the Polish version of the Mini-COPE Inventory for Measurement—Coping with Stress. This questionnaire was initially developed and validated by Carver, Scheier, and Weintraub (Carver et al., 1989), and subsequently adapted by Juczyński and Ogińska-Bulik (2012). The Mini-COPE Inventory assesses dispositional coping strategies employed in highly stressful situations, providing 28 statements corresponding to 14 strategies (with two statements for each strategy). Respondents indicate the frequency of utilizing each strategy when faced with extremely challenging situations, selecting one of four possible answers: “I almost never do that” (0 points), “I rarely do that” (1 point), “I often do that” (2 points), and “I almost always do that” (3 points). A higher score indicates a greater frequency of utilizing that particular coping strategy. In this study, Cronbach's α values for the various coping strategies were as follows: active coping (α = 0.70), planning (α = 0.67), positive reframing (α = 0.70), acceptance (α = 0.59), sense of humor (α = 0.64), turning to religion (α = 0.87), seeking emotional support (α = 0.81), seeking instrumental support (α = 0.68), self-distraction (α = 0.62), denial (α = 0.69), venting (α = 0.50), substance use (α = 0.90), behavioral disengagement (α = 0.61), and self-blame (α = 0.72).
The participants’ self-efficacy was measured using the Polish version of the Generalized Self-Efficacy Scale (GSES). Developed by Schwarzer and Jerusalem (1995) and adapted by Juczyński (2000), the GSES measures individuals’ belief in their abilities to handle challenging or unfamiliar situations. It consists of 10 items rated on a four-point scale, ranging from 1 (“not at all true”) to 4 (“exactly true”). Higher scores indicate greater self-efficacy. In this study, the internal consistency of the GSES was found to be 0.96.
To assess the participants’ physical activity levels, the Godin Leisure-Time Exercise Questionnaire (GLTEQ) was used. The GLTEQ, developed by Godin and Shephard (1985), is a self-administered tool comprising two items that measure habitual physical activity without a specified time component. In this study, only the first part of the questionnaire was included, following the approach of previous research (Gosney et al., 2007; Motl et al., 2006). The first part consists of three open-ended questions that assess the frequency of strenuous (e.g., jogging), moderate (e.g., fast walking), and mild (e.g., easy walking) exercises lasting more than 15 min during one's free time in a typical week. The weekly frequencies of strenuous, moderate, and mild activities are multiplied by metabolic equivalents, specifically 9, 5, and 3, respectively. The products obtained are then summed to determine the total leisure activity. The final score categorization is as follows: scores of 24 units or more are considered active (substantial benefits), scores of 14–23 units are considered moderately active (some benefits), and scores of 13 units or less are considered inactive (few benefits). Previous studies have demonstrated the validity of the GLTEQ as a measure of physical activity in individuals with MS (Guicciardi et al., 2019; Kalron et al., 2019; Motl et al., 2006).
Additionally, participants were asked to complete a demographic data questionnaire that gathered information about their sex, age, educational level, and marital status, as well as details regarding the course of their MS diagnosis and the duration of the disease. In addition, a neurologist assessed the severity of MS using the EDSS, which assigns scores ranging from 0 (indicating a normal examination) to 10 (representing death resulting from MS) (Kurtzke, 1983). The neurologist also confirmed whether the participants exhibited any cognitive and/or psychiatric issues.
Data analysisA principal component analysis (PCA) with varimax rotation was performed to analyze the factor structure of stress coping among the participants. This analysis aimed to reduce the initial 14 dimensions (coping strategies) into smaller number of factors. The determination of the number of factors extracted was based on the parallel method proposed by Horn (1965).
Firstly, a factor analysis of coping strategies was conducted on the study sample. The results revealed two distinct factors. The first factor comprised effective stress-coping strategies, including positive reframing, planning, active coping, seeking emotional support, self-distraction, acceptance, seeking instrumental support, and a sense of humor. The second factor encompassed ineffective stress-coping strategies, such as venting, self-blame, denial, behavioral disengagement, and substance use. Due to the low and similar loadings of the coping strategy “turning to religion” on both extracted factors, it was excluded. Subsequently, PCA 2 was conducted, which yielded nearly identical outcomes to the initial analysis. These two factors (effective and ineffective coping strategies) were employed as dependent variables in the moderated mediation analyses. Refer to Table in the supplementary materials for further details.
Furthermore, two moderated mediation analyses were conducted to examine the relationships among the variables. The independent variable was the level of physical activity, while self-efficacy served as the mediator. The factors extracted from the PCA (effective coping strategies in the first analysis and ineffective coping strategies in the second analysis) were treated as the dependent variables. The analysis also took into account the potential moderating effect of the EDSS score (level of disability). The mediational relationship (physical activity—self-efficacy—stress-coping strategies) was analyzed at three moderator levels (EDSS) as follows: low level (1 SD below the mean EDSS score), average level (mean EDSS score), and high level (+1 SD above the mean EDSS score). According to current recommendations, mediation was deemed to occur when a significant indirect effect was observed. The significance of moderating and mediating paths and effects was assessed using the percentile bootstrap method with 5000 samples, and a 95 % confidence interval was estimated (Hayes, 2017). A statistically significant effect was obtained if the confidence interval did not include zero. The analysis was performed using Jamovi software (version 2.2.5).
It should be noted that the PCA employed in this study was exploratory in nature. Therefore, the factors and the size of factor loadings were not predicted before the study. It is emphasized that when we do not have detailed information about the predicted results of the analysis, however, assuming “moderate” conditions based on the number of strong factor loadings and communalities, a minimum sample size of 200 subjects is recommended for obtaining reliable results (Fabrigar & Wegener, 2012; Pituch & Stevens, 2016).
Similarly, the moderated mediation analysis was partly exploratory since there were limited previous studies on the specific topic under investigation, making it difficult to determine the specific paths to be moderated. Therefore, moderation was carried out on all possible paths within the mediation model. The effect sizes, including the expected mediation effect sizes at each moderator level, were challenging to predict. In social science regression analysis, which forms the basis of mediation and moderation models, a sample size of at least 15 individuals per predictor is generally considered adequate for obtaining reliable results (Pituch & Stevens, 2016). Considering the number of variables and effects in the estimated model, the sample size of 351 participants in our study appears to be sufficient for this type of study.
ResultsParticipantsThe study included a total of 351 participants, with a mean age of 46.2 years (SD = 10.5). Among the participants, 224 were female and 127 were male. The average time since diagnosis was 11.1 years (SD = 7.5). The participants had an average physical activity level of 19.8 units (SD = 20.7). In terms of educational level, 67 participants had primary/vocational education, 141 had secondary education, and 143 had higher education. Regarding the diagnosed types of MS, there were 196 participants with relapsing-remitting MS, 68 with primary progressive MS, 70 with secondary progressive MS, 11 with progressive-relapsing MS, and 6 participants who were unsure of their MS type. The disability subgroups based on the EDSS level were as follows: EDSS ≤ 3.5 (participants), 3.5 < EDSS ≤ 6.5 (175 participants), and EDSS > 6.5 (23 participants).
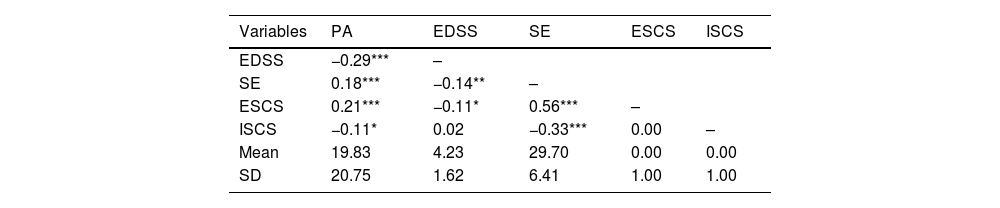
Descriptive statistics and correlations between the main studied variablesIn Table 1, we presented descriptive statistics and correlations among the main variables under study. Almost all correlations were found to be statistically significant. However, the correlations between EDSS and ineffective coping strategies, as well as between effective and ineffective coping strategies, did not reach statistical significance.
Descriptive statistics and correlations between the studied variables.
| Variables | PA | EDSS | SE | ESCS | ISCS |
|---|---|---|---|---|---|
| EDSS | −0.29*** | – | |||
| SE | 0.18*** | −0.14** | – | ||
| ESCS | 0.21*** | −0.11* | 0.56*** | – | |
| ISCS | −0.11* | 0.02 | −0.33*** | 0.00 | – |
| Mean | 19.83 | 4.23 | 29.70 | 0.00 | 0.00 |
| SD | 20.75 | 1.62 | 6.41 | 1.00 | 1.00 |
Note. * p < 0.05, ** p < 0.01, *** p < 0.001.
PA- physical activity, EDSS- Expanded Disability Status, SE- self-efficacy.
ESCS- effective stress-coping strategies, ISCS- ineffective stress-coping strategies.
To address the first research question, we validated a moderated mediation analysis using effective stress-coping strategies as the dependent variable. We observed a significant interaction effect between physical activity and the level of disability on self-efficacy (b = 0.0254, 95 % CI [0.0079, 0.0438]). This suggests that the relationship between physical activity and self-efficacy is contingent upon the level of disability, indicating conditional mediation effects (Table 2).
Effects of interaction-moderation taking into account the relations of the mediation model.
PA- physical activity, EDSS- expanded disability status, SE- self-efficacy, ESCS- effective stress-coping strategies.
*95 % Confidence interval.
Source: Jamovi Software.
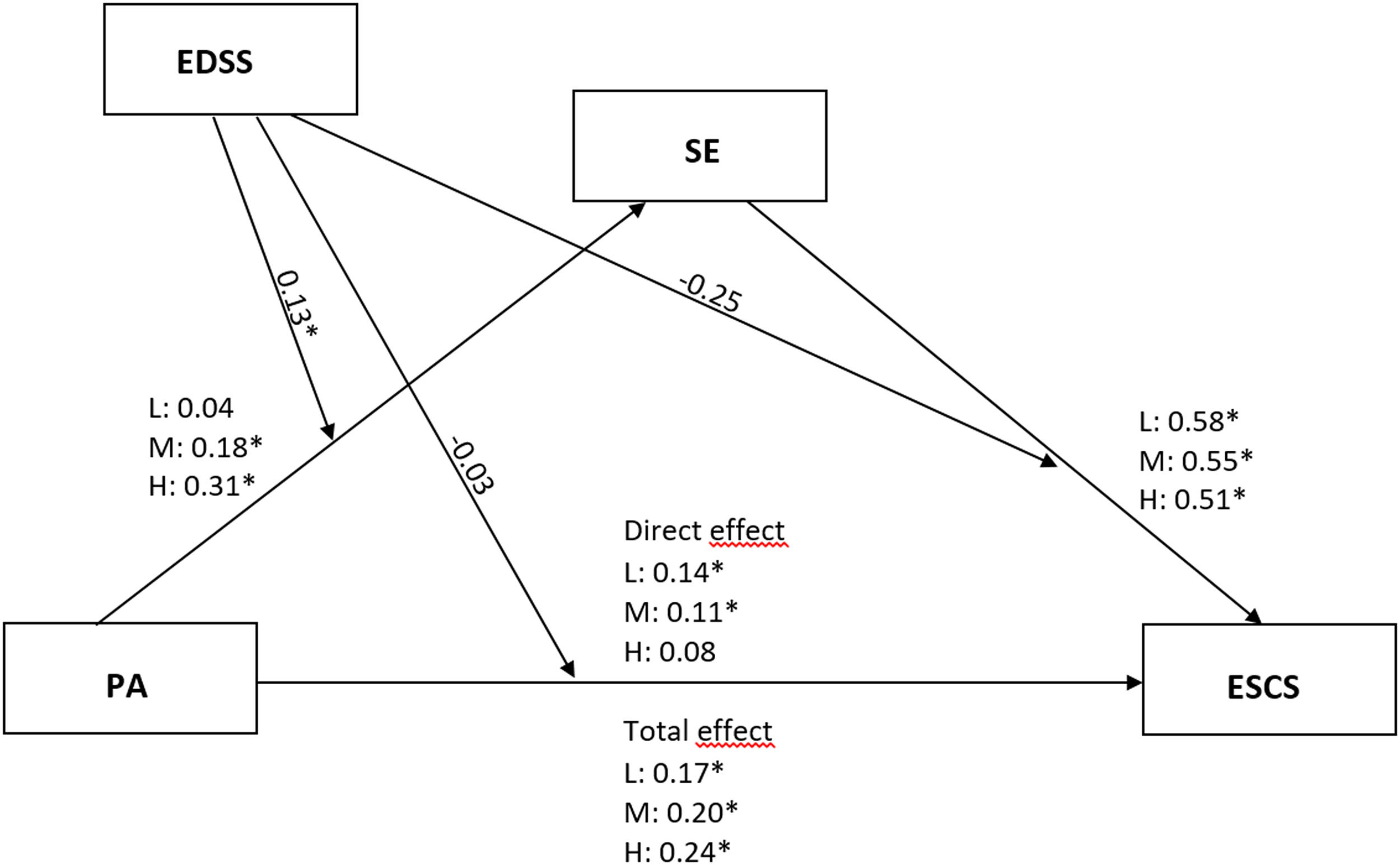
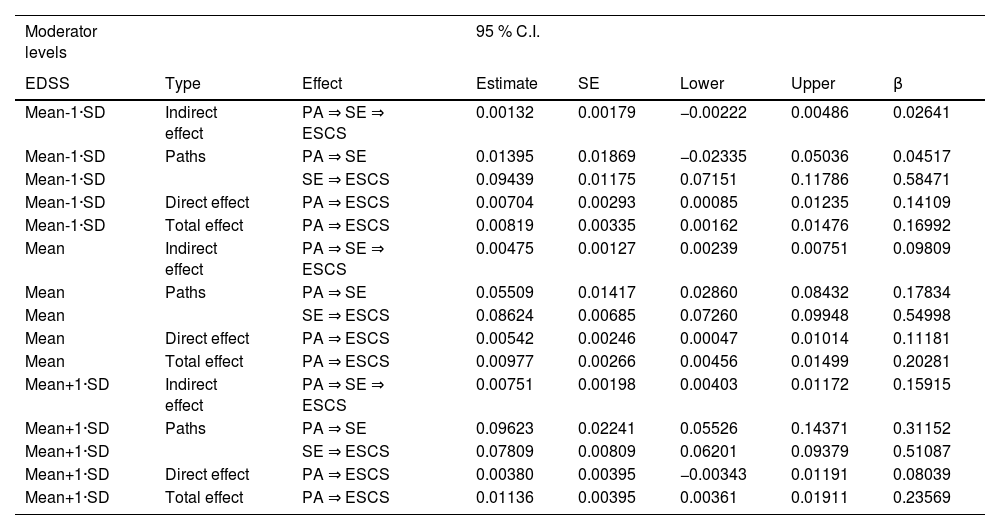
The indirect (mediation) effect of the relationship “undertaking physical activity—self-efficacy—effective coping with stress” was found to be statistically significant for the medium (Table 3, EDSS score: Mean) and high levels of disability (Table 3, EDSS score: mean + 1 SD). In these cases, engaging in physical activity was positively associated with self-efficacy, which in turn was positively associated with effective coping with stress. The indirect effect (β = 0.16) and the relationship between physical activity and self-efficacy (β = 0.31) were largest for individuals with a high level of disability. However, for individuals with a low level of disability (EDSS score: mean −1 SD), the relationship did not reach statistical significance. Similarly, the mediating (indirect) effect of the relationship “physical activity—a sense of self-efficacy—effective coping with stress” was not significant for individuals with a low level of disability (EDSS score: mean −1 SD). In contrast, a strong positive relationship between self-efficacy and effective coping with stress was observed regardless of the disability level. The standardized values for the individual paths of the moderated mediation model can be seen in Fig. 1.
Mediation effects for different EDSS moderator levels.
PA- physical activity, EDSS- expanded disability status, SE- self-efficacy, ESCS- effective stress-coping strategies.
β-standardized coefficient.
Source: Jamovi Software.
 as a mediator in the relationship between physical activity (PA) and effective stress coping strategies (ESCS) for low (L), medium (M), and high (H) EDSS levels (moderator variable) in patients with multiple sclerosis. *p < 0.05; # standardized values are provided.")
Self-efficacy (SE) as a mediator in the relationship between physical activity (PA) and effective stress coping strategies (ESCS) for low (L), medium (M), and high (H) EDSS levels (moderator variable) in patients with multiple sclerosis. *p < 0.05; # standardized values are provided.
To address the second research question, we validated a moderated mediation model involving ineffective stress-coping strategies as the dependent variable. The analysis revealed a significant interaction effect between physical activity and disability level on self-efficacy. This indicates that the relationship between physical activity and self-efficacy is associated with the level of disability (Table 4).
Effects of interaction-moderation taking into account the relations of the mediation model.
PA- physical activity, EDSS- expanded disability status, SE- self-efficacy, ISCS- ineffective stress-coping strategies.
*95 % Confidence interval.
Source: Jamovi Software.
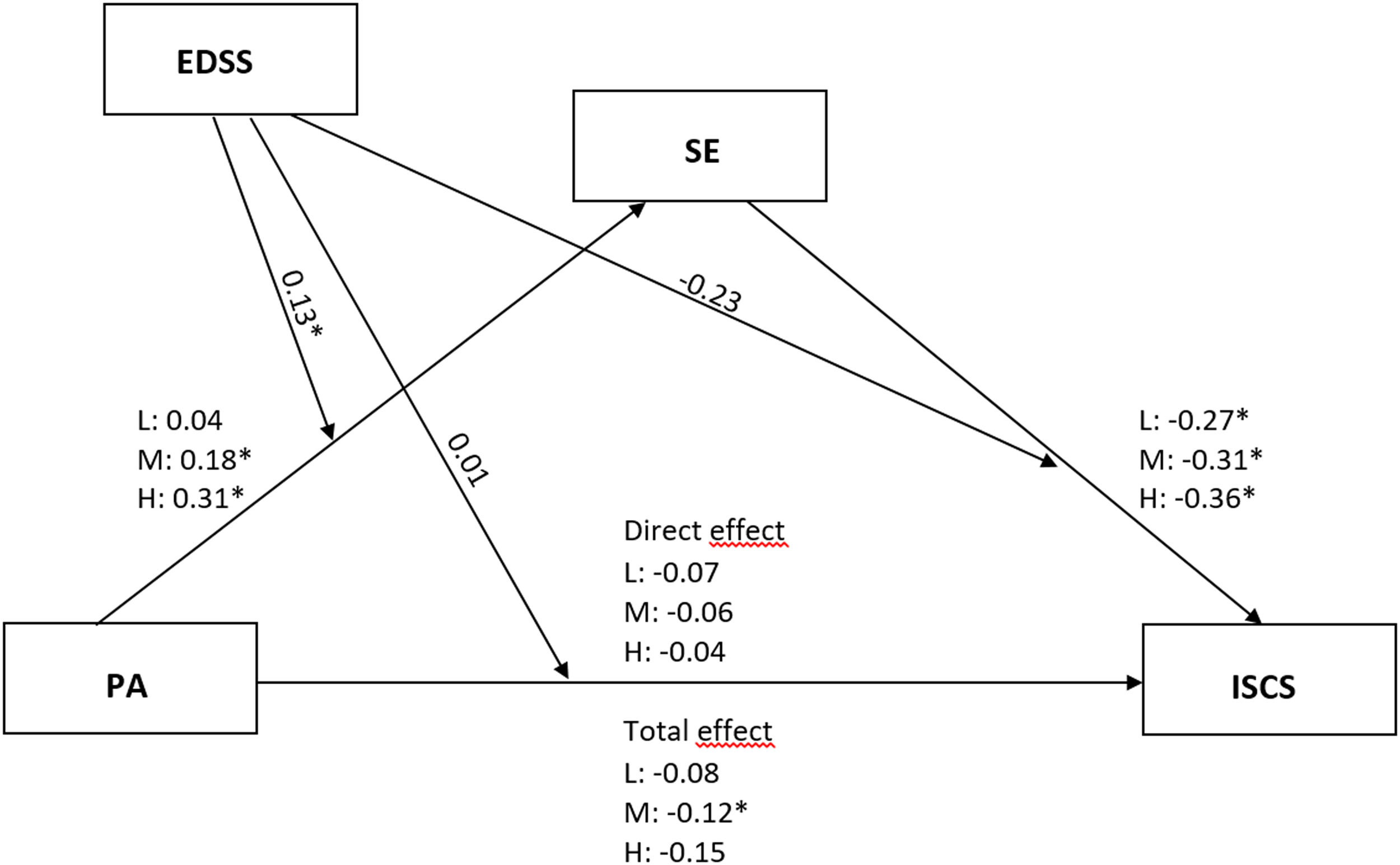
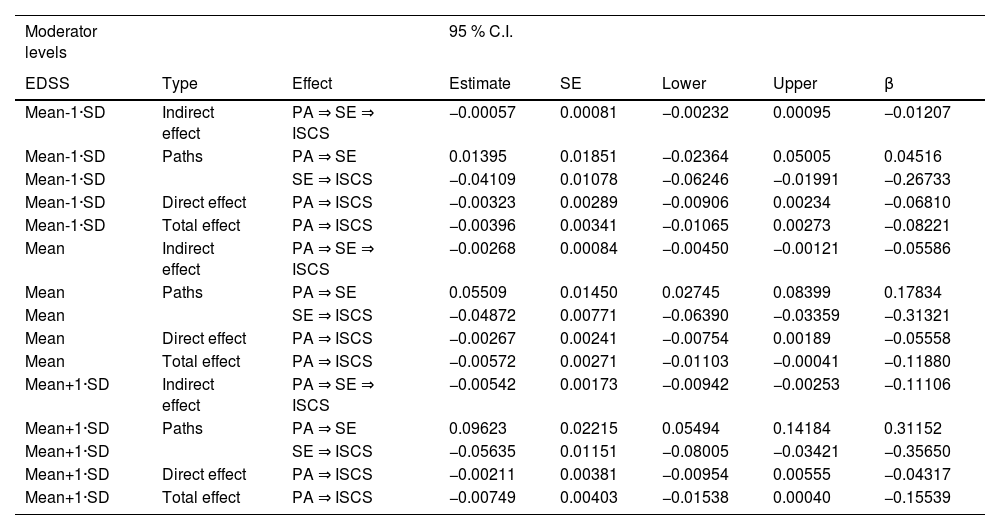
Similarly to the effective coping strategies, the indirect effect of the relationship “undertaking physical activity—self-efficacy—ineffective coping with stress” was found to be statistically significant for medium (EDSS score: mean) and high levels of disability (EDSS score: mean +1 SD). However, the effect was not significant for the low level of disability (EDSS score: mean –1 SD). The mediation effect was largest for the high level of disability (β = −0.11). In the case of medium and high disability levels, physical activity showed a positive association with self-efficacy. Conversely, this relationship was not significant for the low disability level. Additionally, self-efficacy demonstrated a negative association with ineffective stress coping across all levels of disability (Table 5). Fig. 2 presents the standardized values for the individual paths of the moderated mediation model.
Mediation effects for different EDSS moderator levels.
PA- physical activity, EDSS- expanded disability status, SE- self-efficacy, ISCS- ineffective stress-coping strategies.
β-standardized coefficient.
Source: Jamovi Software.
 as a mediator in the relationship between physical activity (PA) and ineffective stress coping strategies (ISCS) for low (L), medium (M), and high (H) EDSS levels (moderator variable) in patients with multiple sclerosis. *p < 0.05; # standardized values are provided.")
Self-efficacy (SE) as a mediator in the relationship between physical activity (PA) and ineffective stress coping strategies (ISCS) for low (L), medium (M), and high (H) EDSS levels (moderator variable) in patients with multiple sclerosis. *p < 0.05; # standardized values are provided.
The main objective of our study was to determine whether self-efficacy mediates the association between physical activity and coping efficacy in people with MS at different levels of disability (moderating variable). To investigate the factor structure of stress coping in our sample, we conducted a PCA with varimax rotation. The results of the analysis allowed us to condense the 14 coping strategies into two main factors, which can be categorized as effective and ineffective strategies based on their content. Our findings supported the assumption of a mediating role for self-efficacy, aligning with previous studies conducted on diverse populations (Wang et al., 2019; Xu & Zhang, 2020) and the social-cognitive theory, which emphasizes the influence of self-efficacy on an individual's coping style (Bandura, 2001).
Physical activity, as a measure of motor task performance, is recognized as important for enhancing self-efficacy (Rollo et al., 2016; Szczuka et al., 2021; Wijndaele et al., 2007), and it has been previously investigated in people with MS (Motl et al., 2007). Higher levels of self-efficacy are associated with reduced negative effects and an increased likelihood of adopting active problem-solving attitudes (Xu & Zhang, 2020). Previous studies with preadolescents have demonstrated that individuals with low self-efficacy tend to employ negative coping strategies during stressful situations (D'Amico et al., 2013). Our results partially support this relationship within our sample of people with MS, with the moderating effect of disability level (as measured by EDSS) being a crucial factor. Specifically, among participants with medium and high levels of disability, physical activity exhibited a positive association with self-efficacy, which, in turn, was positively associated with effective stress-coping strategies and negatively associated with ineffective strategies. Thus, among participants with a moderate and severe physical disability (medium and high EDSS scores), engaging in physical activity was linked to better stress coping through increased self-efficacy. Importantly, the relationship between physical activity and self-efficacy was strongest in participants with high disability, moderately significant in participants with moderate disability, and not statistically significant in participants with low disability.
Our findings are consistent with the observations of other researchers in the field. For example, Snook and Motl (2008) reported that MS patients with higher disability levels, characterized by more frequent motor symptoms, demonstrated lower levels of physical activity. This relationship was partially mediated by self-efficacy. Similarly, Casey et al. (2018) found that MS symptoms moderated the relationship between physical activity and self-efficacy. Individuals with poorer health conditions and limited functionality faced greater challenges in engaging in regular physical activity, but when they were able to participate successfully, it had a stronger impact on their self-efficacy. Our results align with these observations, highlighting the increasing importance of self-efficacy as disability levels rise.
The findings of our study have practical implications for people with MS and health professionals working with this group. These professionals should consider focusing on physical activity as a tool to improve coping with stress. The link between physical activity and the use of more effective coping strategies suggests a potential mechanism through which physical activity can positively impact stress management and psychological health.
Promoting physical activity in individuals with MS, especially those with more physical impairment, is crucial despite the associated challenges. To encourage physical activity, it is important to create an environment that is conducive to the needs of individuals with MS, ensuring comfort and an enjoyable experience. Providing positive motivation and building a support network both within and outside the physical activity environment can also be helpful. Healthcare professionals should focus on designing physical activity programs that maximize improvements in self-efficacy, as regular participation in physical activity can enhance one's self-efficacy. This can be achieved by promoting opportunities for success and accomplishment, creating vicarious experiences, and utilizing verbal persuasion. The development of self-efficacy through these means can translate into the application of more effective coping strategies, thereby contributing to the enhancement of mental health in people with MS.
It is important to acknowledge the limitations of our study when interpreting the results. The cross-sectional design of the study restricts our ability to conclude causal relationships among the variables. While our assumptions are based on theories from the literature, indicating that leisure-time physical activity contributes to the use of coping strategies through improved self-efficacy, it is worth noting that several studies suggest bidirectional relationships between these variables. For example, the selection of appropriate coping strategies may promote better well-being and motivate individuals to engage in higher levels of physical activity, thus increasing their sense of self-efficacy. Moreover, higher levels of generalized self-efficacy may also lead to increased involvement in physical activity, as supported by previous studies (Motl et al., 2010, 2013). These findings align with the concept of reciprocal determinism (Bandura, 2012), which highlights the mutual influence of behavior (such as physical activity and coping) and personal factors (i.e., self-efficacy). There may exist alternative models that offer different yet equally valid explanations for the relationships between these variables. Future research should consider analyzing reciprocal relationships among the variables discussed, using a prospective or experimental design.
Because we excluded individuals with cognitive disorders, a fairly common condition in MS, the results presented here should be generalized with caution. Moreover, the study did not employ objective measurement tools for diagnosing cognitive disorders and relied solely on the assessment of a neurologist. Additionally, we did not collect information from the participants about their use of symptomatic medications, disease-modifying drugs, or steroids that might influence their motor function and physical activity behavior. Finally, the study lacked an objective marker for physical activity, relying solely on self-reported measures, potentially introducing bias into the findings.
ConclusionIn summary, our studies reinforce previous findings that highlight the significant role of self-efficacy in the relationship between physical activity and coping with stress. A novel aspect of our study is the identification of the moderating effect of disability level in people with MS. Our results indicate that among people with higher levels of disability, engaging in physical activity is linked to more effective stress coping through enhanced self-efficacy. However, this effect was not observed among people with low levels of disability. Therefore, engagement in physical activity is significantly associated with the psychosocial functioning of people with a high level of disability, whereas the relationship is less pronounced among people with a low level of disability.
Consent to participateInformed consent was obtained from all individual participants included in the study.
