



Background/Objective: Social vulnerability refers to difficulties detecting potentially harmful interpersonal situations. Although it is an important predictor of psychosocial and interpersonal difficulties in clinical samples, research investigating this construct is scarce. We aimed to (a) develop a brief measure for assessing social vulnerability in typically developing children, the Children's Social Vulnerability Questionnaire (CSVQ) (b) examine the relationship between social vulnerability and psychosocial functioning, (c) explore age-related differences, and (d) explore levels of social vulnerability amongst children with clinical needs. Method: Data were gathered on two samples. Participants were parents (n = 790) of elementary school-aged children (3-12 years), and parents and teachers of a second sample (n = 96). Results: Results provide strong reliability and validity evidence. Social vulnerability showed moderate relationships with emotional and behavioural problems, and only a weak relationship with social skills. Parents perceived greater social vulnerability in younger than older children, and amongst children with clinical needs. Parents’ and teachers’ scores were correlated. Conclusions: Social vulnerability is not simply a lack of social skill; rather, it is a valuable construct for understanding psychosocial risk, especially for young and clinical samples of children.
Antecedentes/Objetivo: La vulnerabilidad social alude a dificultades para detectar situaciones interpersonales potencialmente dañinas. Aunque es un predictor importante de las dificultades, la investigación es escasa. Por tanto, se plantea (a) describir las propiedades psicométricas del Children's Social Vulnerability Questionnaire (CSVQ), (b) examinar la relación entre vulnerabilidad social y funcionamiento psicosocial, (c) explorar las diferencias relacionadas con la edad, y (d) explorar los niveles de vulnerabilidad social en niños con necesidades clínicas. Método: Los datos se recogieron en dos muestras. Los participantes fueron padres (n = 790) de niños de Educación Primaria, y padres y profesores de una segunda muestra (n = 96). Resultados: Se proporciona evidencia sólida acerca de la fiabilidad y validez. La vulnerabilidad social mostró relaciones moderadas con problemas emocionales y de comportamiento, y sólo una relación débil con las habilidades sociales. Los padres percibieron una mayor vulnerabilidad social en los niños más jóvenes que en los mayores, y entre niños con necesidades clínicas. Los informes de padres y profesores estaban correlacionados. Conclusiones: La vulnerabilidad social no es equivalente a las habilidades sociales, pero es un valioso constructo para la comprensión del riesgo psicosocial, especialmente en muestras clínicas y en niños de menor edad.
Effective functioning in the social world requires the ability to identify situations where involvement may lead to negative consequences (Greenspan, Loughlin, & Black, 2001). Even though a tendency to trust others is generally considered to be an adaptive attribute (Betts & Rotenberg, 2008), difficulties understanding situations that involve deception may leave an individual open to being deceived, misled, or cheated (Greenspan et al., 2001). This impaired ability to detect or avoid potentially harmful interpersonal interactions is referred to as social vulnerability (Pinsker, Stone, Pachana, & Greenspan, 2006). Theoretically, two constructs are believed to underlie social vulnerability: credulity (a tendency to believe something that is highly questionable despite limited evidence) and gullibility (a vulnerability to being tricked or manipulated) (Greenspan et al., 2001). These two constructs are thought to be closely related in that the presence of credulity invariably leads to a gullible outcome (Greenspan et al., 2001). As a result, being socially vulnerable can diminish a person's capacity to interact in social situations and contribute to negative interpersonal experiences, such as victimisation and exploitation.
Studies have indicated that individuals at social-cognitive risk display increased levels of social vulnerability. For example, older adults with a neurological condition (Pinsker, McFarland, & Stone, 2011; Pinsker et al., 2006) and children with Asperger's syndrome (Sofronoff, Dark, & Stone, 2011) are more socially vulnerable than their healthy/typically developing peers. Importantly, social vulnerability has also been linked with an increased risk of negative interpersonal outcomes. In older adolescents and adults with developmental disabilities, Fisher, Moskowitz and Hodapp (2012, 2013) identified specific facets of ‘social vulnerability’ (e. g., a decreased ability to detect risk, being perceived by others as being physically vulnerable, and having low social protection from peers) associated with each disorder that place individuals at risk for victimisation. Moreover, in children with Asperger's syndrome, social vulnerability was associated with social interaction difficulties and emotional/behavioural problems, and was a unique predictor of peer victimisation. Together, these studies demonstrate that social vulnerability is elevated in those who experience social-cognitive difficulties, and is an important predictor of psychosocial and interpersonal difficulties.
Young children who are developing typically may also be at risk for being deceived and misled in social situations. In the elementary school years, children go through a process of substantial cognitive and social development (Anderson et al., 2001). During this time, they may be socially vulnerable to interactions that are intended to harm (Greenspan, 2009; Greenspan et al., 2001). Considering social vulnerability in typically developing children may help us to understand this aspect of children's social interactions, which is not captured in current measures of social interactions, such as social skills (e. g., showing empathy for others, helping out, being kind) or social problems (e. g., aggression, bullying, being victimised). Despite the potential for social vulnerability to inform us on children who are at risk for being taken advantage of or misled in social situations, and/or victimised, there has been limited empirical research in this population. This paucity of research may, in part, be due to the lack of an appropriate measure for this population.
Existing measures of social vulnerability have been developed specifically for at-risk populations. For example, Pinsker et al. (2006) developed an informant-rated scale to measure older adults’ susceptibility to exploitation in financial situations – The Social Vulnerability Scale for Older Adults. Consistent with Greenspan et al.’s (2001) theory, Pinsker et al. (2011) found a two-factor structure: credulity and gullibility. A modified version of this scale, the Social Vulnerability Scale (SVS), was developed by Sofronoff and colleagues (2011) for children with Asperger's syndrome. Items concerning credulity, gullibility and being victimised as a result of the child's disability were included. Although a two-factor solution was found, there were notable deviations from the expected differentiation between credulity and gullibility. Specifically, the first factor (gullibility) contained victimisation items and the second factor contained both credulity and gullibility items. Consequently, these findings raise doubt as to whether the two-factor conceptualisation of social vulnerability described by Greenspan et al. (2001) is applicable to children.
One additional scale - the Social Vulnerability Rating Instrument- Children's Version (SVRI-CV) – was developed for use with children with neurological conditions and recently used with typically developing children (Bianco, 2013). The SVRI-CV is a 20-item parent-report measure of social vulnerability that assesses both credulity and gullibility, based on the Pinsker et al. (2006) scale. Bianco (2013) provided preliminary support for the SVRI-CV in a typically developing Australian elementary school-aged population (n = 232). Psychometric analysis of the SVRI-CV revealed good internal reliability for the full scale (α = .85) and high test-retest reliability at a 4-week interval (r = .93), suggesting that it is a psychometrically reliable tool for identifying children who are socially vulnerable in a typically developing population. However, Bianco (2013) identified a number of items that displayed poor item-total correlations. Furthermore, examination of the items revealed a degree of redundancy, as well as questionable face validity for some items (e.g., “resists doing things that he/she doesn’t want to do”). At 20-items, the length of the SVRI-CV is also likely to be prohibitive for research. Hence, in order to facilitate research on social vulnerability in typically developing children, a new scale is needed. The current study aimed to address this need by developing a new, brief, parent-report social vulnerability scale with strong psychometric properties suitable for use with typically developing children the Children's Social Vulnerability Questionnaire (CSVQ). This study describes the development of the CSVQ, including the construction of the scale, exploration of its factor structure, and examination of the psychometric properties. We also examine the relationship between social vulnerability and children's psychosocial functioning, using both parents and teachers as reporters. Based on the findings of Sofronoff et al. (2011), we expected that higher ratings of social vulnerability would be associated with internalising and externalising behaviour, but not social skills. Finally, we examined age-related differences in social vulnerability in typically developing children, and explored the level of social vulnerability amongst children with clinical needs.
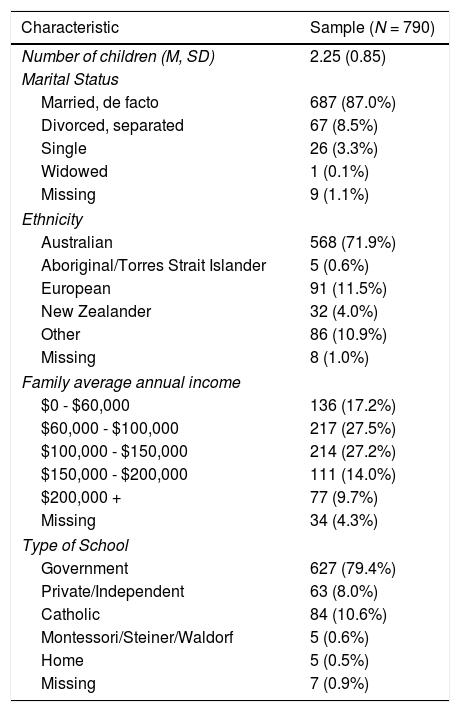
MethodParticipantsNine-hundred and two parents/guardians of elementary school-aged children (Kindergarten – Year 6) from across Australia participated in the study. Of the 902 parents, 112 reported that their child had a physical, mental or chronic illness or disability and were removed from the psychometric analysis of the scale. The data from these children were used to perform a case study analysis of the social vulnerability scores associated with different clinical groups (described later). This left data from 790 parents/guardians (93% mothers) for analysis. The sample consisted of parents of 417 girls (52.8%) and 373 boys, ranging in age from 3 years 8 months to 12 years 4 months. Additional demographic characteristics of the sample are presented in Table 1.
Demographic characteristics of the sample.
| Characteristic | Sample (N = 790) |
|---|---|
| Number of children (M, SD) | 2.25 (0.85) |
| Marital Status | |
| Married, de facto | 687 (87.0%) |
| Divorced, separated | 67 (8.5%) |
| Single | 26 (3.3%) |
| Widowed | 1 (0.1%) |
| Missing | 9 (1.1%) |
| Ethnicity | |
| Australian | 568 (71.9%) |
| Aboriginal/Torres Strait Islander | 5 (0.6%) |
| European | 91 (11.5%) |
| New Zealander | 32 (4.0%) |
| Other | 86 (10.9%) |
| Missing | 8 (1.0%) |
| Family average annual income | |
| $0 - $60,000 | 136 (17.2%) |
| $60,000 - $100,000 | 217 (27.5%) |
| $100,000 - $150,000 | 214 (27.2%) |
| $150,000 - $200,000 | 111 (14.0%) |
| $200,000 + | 77 (9.7%) |
| Missing | 34 (4.3%) |
| Type of School | |
| Government | 627 (79.4%) |
| Private/Independent | 63 (8.0%) |
| Catholic | 84 (10.6%) |
| Montessori/Steiner/Waldorf | 5 (0.6%) |
| Home | 5 (0.5%) |
| Missing | 7 (0.9%) |
A second sample of parents (84.4% mothers) as well as teachers of a local sample of children (n = 96) also participated in the study to provide further evidence for the reliability and validity of the scale. Participants were recruited through elementary schools of varying socio-economic status across the metropolitan area of a major city. The sample consisted of 45 boys (46.9%) and 51 girls, ranging in age from 6 years 1 month to 11 years 8 months.
Measures and ProcedureThis study was approved by our University's ethics committee. A web-based software program (Qualtrics) was used to conduct the survey online over a period of 14 months. Participants were recruited via advertisements placed in newsletters of schools or education associations in each state. In addition to this, the study was advertised via the media, as well as through email distribution lists. The study was introduced as an investigation into children's ability to detect or avoid potentially harmful social interactions. Parents who were interested in participating were asked to access the study via a web link given in the advertisements. Upon entering the survey website, a participant information sheet was presented along with links to follow depending on whether parents consented or declined to participate. Parents who consented to participate completed three questionnaires (described below). No monetary compensation was provided. However, upon conclusion, parents had the opportunity to enter a draw to win 1 of 10 prize vouchers.
Scale Development: Children's Social Vulnerability Questionnaire (CSVQ). The items for the CSVQ included items from the SVRI-CV (Bianco, 2013), as well as those items from the SVS (Sofronoff et al., 2011) that were deemed to be appropriate for a typically developing population. We initially sought qualitative feedback on the content of these items from a small sample of parents (n = 10) from the target population (i. e., parents of elementary school children). Qualitative feedback revealed that there was repetition within the scale (e. g., “is easily talked into handing over toys or money” and “can be talked into giving up or trading valued objects”) and that some of the items were not applicable to young children (e. g., “lent money or things to someone who is unlikely to repay them or give them back”). Based on this feedback, some items were removed and others were rewritten to be appropriate for use with 4-year-olds through to 12-year-olds. In addition, two items that targeted the construct definition (i.e., the ability to detect and/or avoid harmful interpersonal interactions) were written by the authors, as it was felt that this content was not sufficiently interrogated by the included items. Consequently, the preliminary scale used for the development of the CSVQ consisted of 11 items. Of these, 6 were hypothesised to map on to the credulity factor and 5 on to the gullibility factor. Parents were asked to rate the extent to which they agreed with the statements about their child's behaviour over the past 6 months on a 5-point Likert scale (0 = never or very rarely, 4 = very often or always).
Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997). The SDQ is a widely-used 25-item informant-rated measure of behavioural and emotional problems for children aged 3 to 16 years of age (Goodman, 1997). In the current study, scores on the internalising problems (emotional symptoms and peer relationship problems), externalising problems (conduct problems and hyperactivity/inattention), and prosocial behaviour subscales (Goodman, Lamping, & Ploubidis, 2010) were used to examine the validity of CSVQ measurements. For this study, the internal consistency was adequate for the internalising problems (α = .69), externalising problems (α = .70) and prosocial behaviour (α = .74) scales.
Demographics. Parents were asked to provide background information regarding themselves and the child being rated.
Statistical analysisCSVQ data were screened for missing values. Little's missing completely at random (MCAR) test demonstrated that data were missing completely at random, χ2 (108) = 93.24, p = .843. The proportion of missing values was 0.25%; therefore, expectation maximisation in SPSS was used to replace missing values before conducting the factor analysis.
The data were analysed in three stages. Stage 1 involved an exploratory and confirmatory factor analysis. To do this, the sample was randomly split in half within each year level, leaving 389 participants in the first sample (EFA) and 401 participants in the second sample (CFA). Stage 2 involved a series of analyses to examine the psychometric properties of the scale and year level differences in social vulnerability. Given that children's social experiences largely occur at school with peers in their year level, and because it was anticipated that exposure to social experiences and peer interactions at school would be one of the critical factors influencing changes in social vulnerability (due to the influence of peers on social development; Bagwell & Schmidt, 2014), comparisons of social vulnerability scores were based on year level at school, rather than chronological age. For these analyses, the whole sample was examined. Finally, in Stage 3, mean ratings of social vulnerability in the typically developing sample were compared to ratings of social vulnerability in the subsample of children who were identified to have a physical, mental or chronic illness or disability.
ResultsStage 1: Examining the factor structure of the CSVQExploratory factor analysis. An exploratory factor analysis using a maximum likelihood extraction and direct oblimin rotation was conducted on the CSVQ. The Kaiser-Meyer-Olkin measure of sampling adequacy was .93, and Bartlett's test of sphericity was significant, χ2 (55) = 1827.78, p < .001. To provide an indication of how many factors to extract, a parallel analysis was performed using the procedure outlined by O’Connor (2000). This revealed only one significant eigenvalue (using the 95th percentile as the criterion), suggesting that a single factor should be extracted. The eigenvalues from the exploratory factor analysis also suggested a one-factor solution with the first factor producing an eigenvalue of 5.39 and accounting for 48.9% of variance in the CSVQ, whereas the second factor had an eigenvalue less than 1 (i. e., .92). Similarly, inspection of the scree plot provided further support for a one-factor solution. Items with factor loadings above .55 were deemed to be good items (Comrey & Lee, 2013) and were retained. Consequently, item 2 (“is friends with, or plays with, kids who have been mean to him/her in the past”) was removed from the scale.
A second exploratory factor analysis of the remaining 10-items again supported a one-factor solution that accounted for 51.9% of variance in the CSVQ, with all factor loadings greater than .55. However, examination of the reproduced residuals revealed two values above .10, suggesting the presence of another factor (Tabachnick & Fidell, 2013). Consequently, another exploratory factor analysis forcing a two-factor solution was conducted. All items, apart from one (item 8) loaded onto a single factor. Thus, the two-factor solution was deemed to be invalid, and the 10-item single factor solution was endorsed.
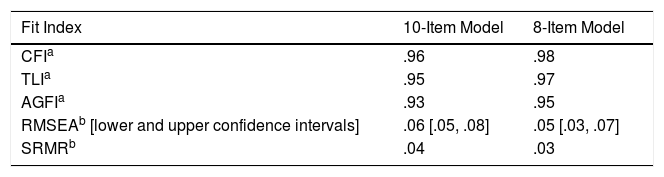
Confirmatory factor analysis. A confirmatory factor analysis using IBM SPSS AMOS version 21.0 was conducted to examine the fit of the 10-item one-factor solution identified in the exploratory factor analysis. Due to moderate levels of item skewness and the sensitivity of structural equation modelling to deviations from normality, square root transformations were conducted on each item, following which, normality was achieved with item skewness and kurtosis values below the recommended cut-off criteria (i.e., skewness ≤ 2, kurtosis ≤ 7; Cohen, Cohen, West, & Aiken, 2003). The 10-item model was estimated using maximum likelihood estimation. The fit of the model was assessed through examination of the chi-square statistic, particularly the adjusted χ2 (χ2/df) (the chi-square statistic is known to be overly sensitive in moderate to large sample sizes, so it has been argued that the model demonstrates reasonable fit if χ2/df ≤ 3; Kline, 2013). In addition, incremental model fit indices, including the Comparative Fit Index [CFI], Tucker-Lewis Index [TLI], Adjusted Goodness of Fit Index [AGFI], root mean square error of approximation [RMSEA], and standardised root mean squared residual [SRMR], were examined as the robustness of these particular indices has been demonstrated (Hu & Bentler, 1999).
Examination of the fit statistics for the 10-item solution showed that the chi-square statistic was significant, χ2 (35) = 90.37, p < .001, however the adjusted χ2 value was adequate (2.58). Further examination of the incremental fit statistics demonstrated that some did not meet recommended cut-off criteria (see Table 2), suggesting that the model did not provide a good fit to the data. Inspection of the modification indices suggested that the largest improvements to the fit of the model would be made by allowing the error variances of items 1 (“believes everything kids tell him/her”) and 3 (“is easily talked into handing over toys, valued items or money”), and 3 and 4 (“can be persuaded into doing things that he/she doesn’t want to do or things that will get them into trouble”) to correlate, suggesting some similarity among these items that is not related to the construct underlying the rest of the scale. The squared multiple correlations demonstrated that of these items, the construct explained the least variance in items 1 and 3 (.29 and .30, respectively). Therefore, items 1 and 3 were removed from the scale, and a subsequent confirmatory factor analysis was used to examine the fit of an 8-item model. For this model, the chi-square statistic was significant, χ2 (20) = 41.62, p = .003, however the adjusted χ2 was adequate (2.08). All incremental fit statistics met or exceeded recommended cut-off criteria (see Table 2), suggesting that the 8-item model provided a good fit to the data.
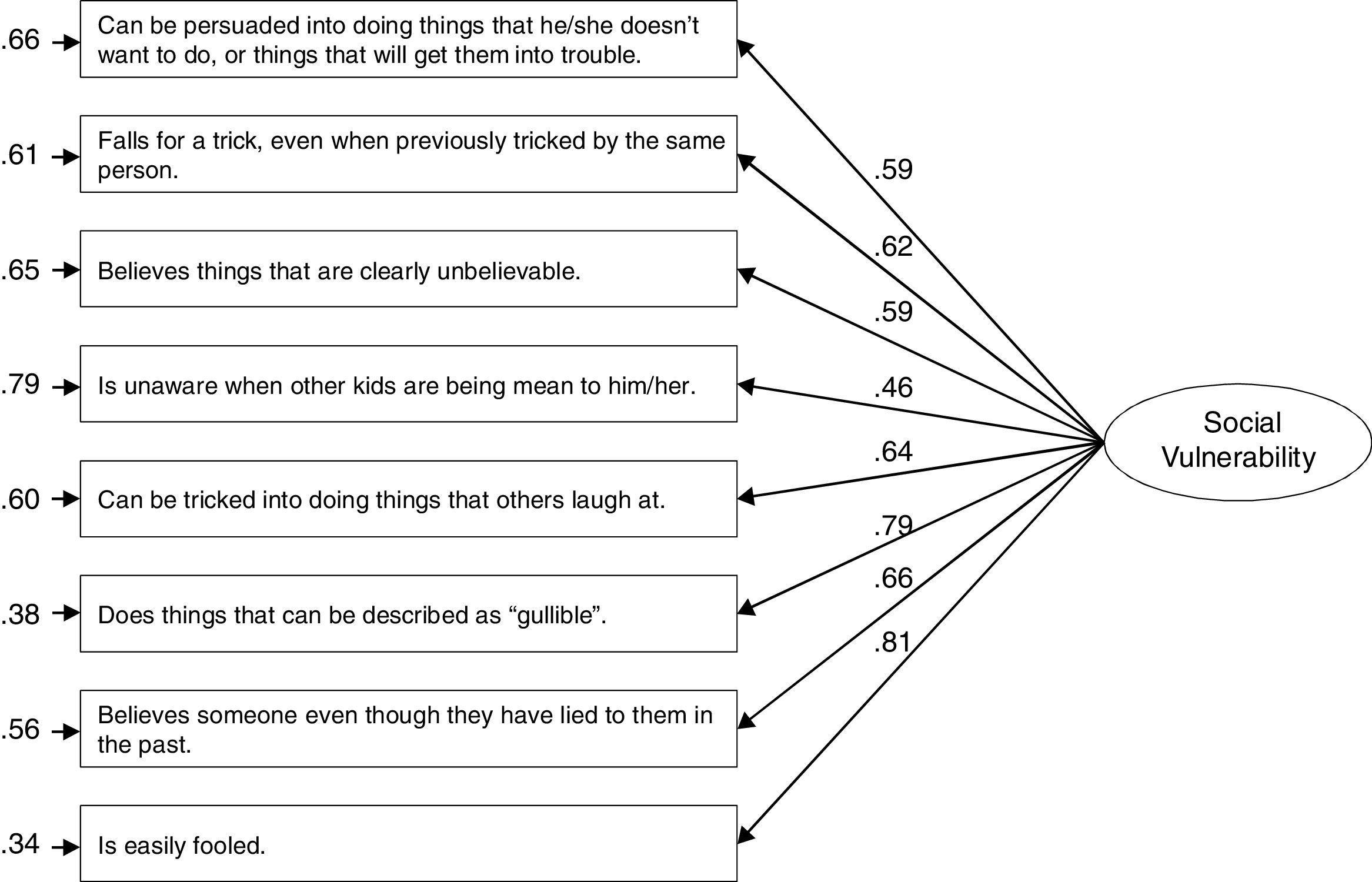
All items were found to load onto the social vulnerability factor, and all standardised loadings were above .45, with 3 gullibility items and 5 credulity items. Thus, the confirmatory factor analysis provided support for a one-factor, 8-item solution of the CSVQ. Parameter estimates are presented in Figure 1.

Parameter estimates for the CSVQ one-factor model. The numbers next to the single-headed arrows leading from the latent variable to the observed variables are the standardised factor loadings. The values next to the small single-headed arrows leading to the observed variables reflect the residual variance for each item.
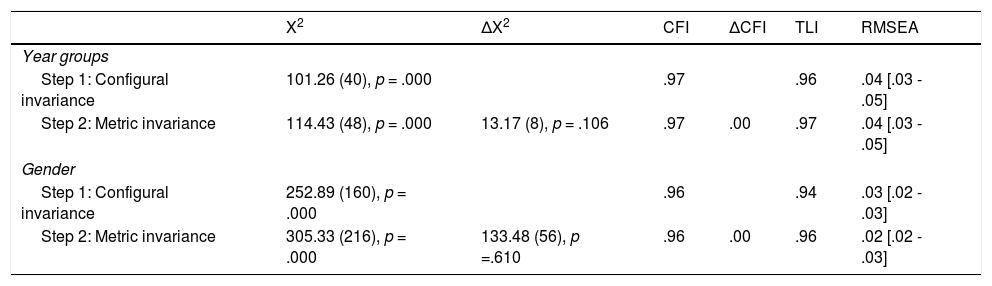
To cross-validate the one-factor solution across gender and school year level, measurement invariance was assessed. To do this, we performed multiple group confirmatory factor analyses based on the procedure recommended by Cheung and Rensvold (2002). A CFI difference criterion (ΔCFI ≤ -.01 between the configural and metric invariance models) was used to determine measurement invariance (as per Cheung & Rensvold, 2002). Results are summarised in Table 3, and indicate that the CFI difference between the configural invariance model and the metric invariance model was below this criterion for both gender and school year level. Additionally, fit indices (i. e., TLI, RMSEA) for the models demonstrated adequate goodness of fit. Therefore, it can be concluded that the factor structure does not differ between genders or across year levels, providing support for the 8-item model across groups.
Analysis of measurement invariance.
| X2 | ΔX2 | CFI | ΔCFI | TLI | RMSEA | |
|---|---|---|---|---|---|---|
| Year groups | ||||||
| Step 1: Configural invariance | 101.26 (40), p = .000 | .97 | .96 | .04 [.03 - .05] | ||
| Step 2: Metric invariance | 114.43 (48), p = .000 | 13.17 (8), p = .106 | .97 | .00 | .97 | .04 [.03 - .05] |
| Gender | ||||||
| Step 1: Configural invariance | 252.89 (160), p = .000 | .96 | .94 | .03 [.02 - .03] | ||
| Step 2: Metric invariance | 305.33 (216), p = .000 | 133.48 (56), p =.610 | .96 | .00 | .96 | .02 [.02 - .03] |
Prior to analysis, examination of the distribution of total CSVQ scores within each year level indicated that normality was achieved (i.e., skewness ≤ 2, kurtosis ≤ 7; Cohen et al., 2003). Data were also screened for univariate outliers based on children's year level; as a result, two participants were removed.
Reliability. The internal consistency of the CSVQ was good (α = .86). Corrected item-total correlations for each item ranged from .48 to .75. The test re-test reliability of the CSVQ was assessed in a small subsample of participants (n = 84) who elected to complete the questionnaires again at a 1-month interval. Test re-test reliability was strong (r(73) = .74), indicating that CSVQ scores remained relatively stable over this time period.
Validity. To assess the concurrent and discriminant validity of the scale, partial correlations between social vulnerability and subscale scores on the SDQ were examined (controlling for year level). Social vulnerability displayed moderate, positive, correlations with internalising symptoms (r(785) = .32, p < .001) and externalising symptoms (r(785) = .33, p < .001), and a weak, negative, correlation with prosocial behaviour (r(785) = -.09, p = .008).
Additional assessment of reliability and validity. To assess the inter-rater reliability of the scale we asked both parents and class teachers of a local sample of children to complete the CSVQ and SDQ, and then correlated the reports, in line with the procedure used by Achenbach, Edelbrock and Howell (1987). Ratings of social vulnerability between parents and teachers were significantly correlated (r(93) = .29, p = .004).
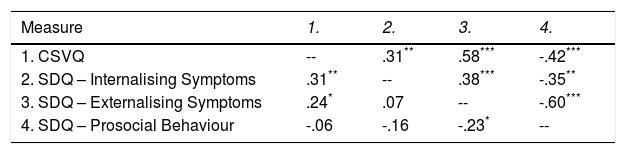
Partial correlations between social vulnerability and subscale scores on the SDQ (controlling for year level) for parents and teachers were then examined to further assess the concurrent and discriminant validity of the scale (see Table 4). For both parent and teacher reports, there was a significant, positive correlation between social vulnerability and internalising symptoms and externalising symptoms. The correlation between social vulnerability and prosocial behaviour was negative (albeit, not significant for parents). The magnitude of the parent report correlations were similar to the magnitude of correlations that emerged in the larger national sample.
Partial correlations controlling for year level between social vulnerability and internalising symptoms, externalising symptoms, and prosocial behaviour (df = 93).
| Measure | 1. | 2. | 3. | 4. |
|---|---|---|---|---|
| 1. CSVQ | -- | .31** | .58*** | -.42*** |
| 2. SDQ – Internalising Symptoms | .31** | -- | .38*** | -.35** |
| 3. SDQ – Externalising Symptoms | .24* | .07 | -- | -.60*** |
| 4. SDQ – Prosocial Behaviour | -.06 | -.16 | -.23* | -- |
Note. Teacher reports are presented above the diagonal and parent reports are presented below the diagonal.
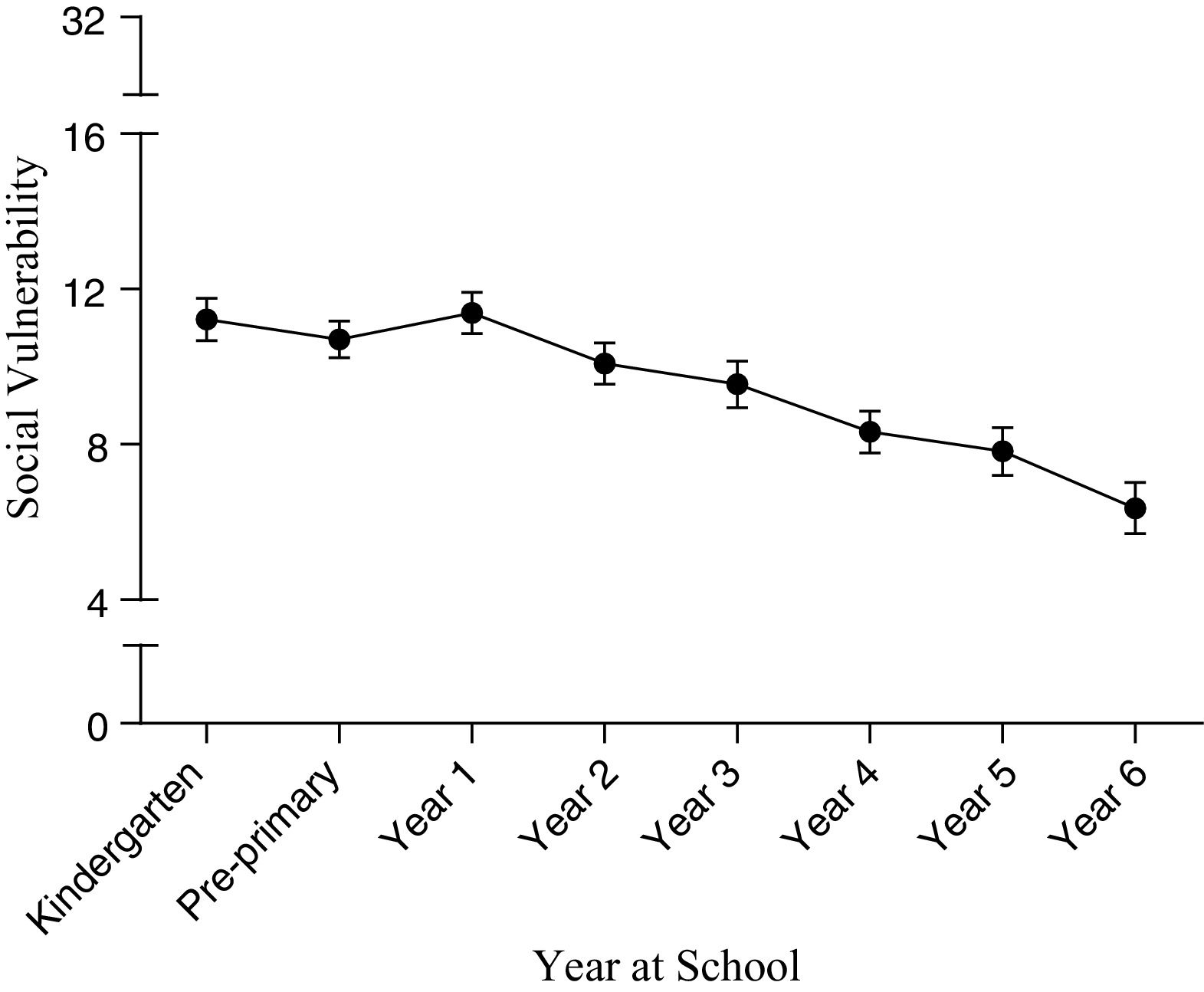
Year level differences in social vulnerability1. To examine differences in social vulnerability across year levels, mean scores for each year level and gender were compared. Mean social vulnerability scores and standard errors for each year level are presented in Figure 2.

A two-way analysis of variance with year level and gender as between-subjects factors was conducted on total scores on the CSVQ. This analysis revealed a significant, medium effect of year level, F(7, 772) = 9.27, p < .001, ηp2 = .08, with children in lower year levels rated as being more socially vulnerable than children in higher year levels, and a significant, weak effect of gender, F(1, 772) = 5.79, p = .016, ηp2 = .01, with boys (M = 9.91, SE = .29) rated as being more socially vulnerable than girls (M = 8.95, SE = .27). The interaction between year level and gender was not significant, F(7, 772) = .95, p = .470, ηp2 = .01.
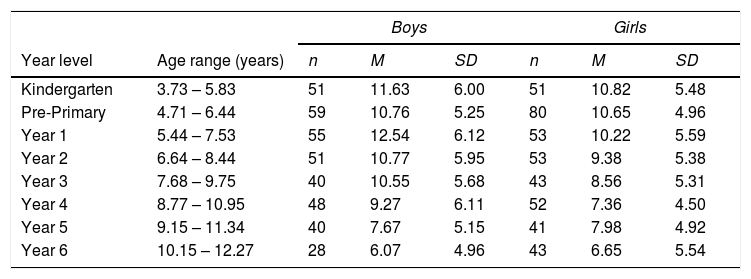
To further examine the impact of year level on social vulnerability, pairwise comparisons using a Bonferroni correction were conducted. Results demonstrated gradual reductions in parent perceptions of children's social vulnerability with increasing year level, with significant differences in social vulnerability scores between children in Year 4 and children in the first three year levels (i. e., Kindergarten, Pre-Primary, and Year 1), children in Year 5 and children in the first three year levels (i.e., Kindergarten, Pre-Primary, and Year 1), and children in Year 6 and children in the first five year levels (i. e., Kindergarten, Pre-Primary, Year 1, Year, 2, and Year 3) (all p < .05). Means and standard deviations for the sample by year level and gender are presented in Table 5.
Means and standard deviations of social vulnerability across year level and gender.
| Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|
| Year level | Age range (years) | n | M | SD | n | M | SD |
| Kindergarten | 3.73 – 5.83 | 51 | 11.63 | 6.00 | 51 | 10.82 | 5.48 |
| Pre-Primary | 4.71 – 6.44 | 59 | 10.76 | 5.25 | 80 | 10.65 | 4.96 |
| Year 1 | 5.44 – 7.53 | 55 | 12.54 | 6.12 | 53 | 10.22 | 5.59 |
| Year 2 | 6.64 – 8.44 | 51 | 10.77 | 5.95 | 53 | 9.38 | 5.38 |
| Year 3 | 7.68 – 9.75 | 40 | 10.55 | 5.68 | 43 | 8.56 | 5.31 |
| Year 4 | 8.77 – 10.95 | 48 | 9.27 | 6.11 | 52 | 7.36 | 4.50 |
| Year 5 | 9.15 – 11.34 | 40 | 7.67 | 5.15 | 41 | 7.98 | 4.92 |
| Year 6 | 10.15 – 12.27 | 28 | 6.07 | 4.96 | 43 | 6.65 | 5.54 |
To explore the potential clinical utility of the scale, a case study analysis was performed on scores for children whose parents indicated that they had a physical, mental or chronic illness or disability. To do this, CSVQ scores for each child were compared with the corresponding mean score and standard deviation for the child's year level and gender derived from the sample of typically developing children, and a z-score was calculated. Clinical groups that had a small number of cases (n < 10) were combined into an ‘other’ category, which included children indicated to have an intellectual disability, motor dyspraxia and sensory processing difficulties.
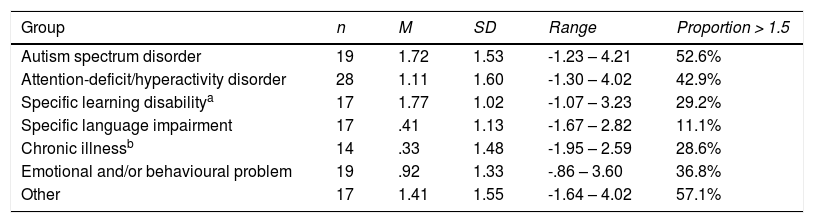
For each clinical group, the proportion of children with a CSVQ rating at least 1.5 standard deviations above the typically developing year level and gender mean is presented in Table 6, alongside descriptive information. Social vulnerability scores were elevated across all clinical groups, but were particularly elevated in children with an autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and children classified in the ‘other’ category, with mean z-scores for each of these groups greater than 1, and at least 40% of children in each group with a total social vulnerability rating greater than 1.5 times their year level and gender mean.
Mean, standard deviation and range of standardised scores, and proportion of children with a standardised score above 1.5 for each clinical group.
| Group | n | M | SD | Range | Proportion > 1.5 |
|---|---|---|---|---|---|
| Autism spectrum disorder | 19 | 1.72 | 1.53 | -1.23 – 4.21 | 52.6% |
| Attention-deficit/hyperactivity disorder | 28 | 1.11 | 1.60 | -1.30 – 4.02 | 42.9% |
| Specific learning disabilitya | 17 | 1.77 | 1.02 | -1.07 – 3.23 | 29.2% |
| Specific language impairment | 17 | .41 | 1.13 | -1.67 – 2.82 | 11.1% |
| Chronic illnessb | 14 | .33 | 1.48 | -1.95 – 2.59 | 28.6% |
| Emotional and/or behavioural problem | 19 | .92 | 1.33 | -.86 – 3.60 | 36.8% |
| Other | 17 | 1.41 | 1.55 | -1.64 – 4.02 | 57.1% |
Note.
The aim of this research was to create a reliable and valid parent-report measure of social vulnerability suitable for use with typically developing children and to examine the utility of the scale. The CSVQ demonstrated strong psychometric properties, including very good internal consistency, good test re-test reliability and sound inter-rater agreement. Having developed a psychometrically sound instrument of social vulnerability, we then examined the relationship between social vulnerability and psychosocial functioning in children. In three samples (two parent and one teacher), reports of social vulnerability were associated with both internalising and externalising problems; that is, children who were rated as being socially vulnerable were likely to display higher levels of emotional and behavioural difficulties. This is consistent with results from children with Asperger's syndrome (Sofronoff et al., 2011), and provides support for the concurrent validity of the CSVQ. Furthermore, the weak negative relationship between parent reports of social vulnerability and prosocial behaviour indicates that being socially vulnerable is not simply having a lack of social skills, providing support for discriminant validity. This is consistent with Greenspan et al. (2001) who suggested that poor social skills are likely to contribute to (but are not the same thing as) being deceived or cheated. Finally, the moderate level of agreement on CSVQ scores between parents and teachers in this sample is consistent with levels of inter-rater agreement reported between parents and teachers on other measures of child psychopathology (Achenbach et al., 1987), providing support for the inter-rater reliability of the CSVQ. Taken together, these findings suggest that the CSVQ is a reliable and valid measure of social vulnerability in children. Moreover, they indicate that social vulnerability is a discrete construct that is not simply indicative of general psychosocial difficulties, but is potentially important for understanding emotional and behavioural difficulties in children.
Another important finding was that parents perceived children in younger years as more socially vulnerable than children in older years. The overall pattern suggests a progressive decline in social vulnerability throughout elementary school, consistent with the hypothesis of Greenspan et al. (2001) that social vulnerability decreases with age, and with research in the critical stance field that indicates that children's ability to critically evaluate information improves with age (Mills, 2013). It is possible that increased social exposure throughout school and the influence of peers on social interactions may explain this pattern, whereby children learn to independently navigate social interactions and learn through exposure to situations in which social vulnerability may result in negative outcomes. Alternatively, this developmental trend could be explained by advances in cognitive functioning (Mills, 2013).
Finally, we identified that social vulnerability may be an issue for many clinical groups; most notably, children with ADHD and ASD (the latter of which has previously been documented; Sofronoff et al., 2011). There is a plethora of research on the negative social interactions experienced by children with ADHD and ASD, but only one study (i. e., Sofronoff et al., 2011) has considered the potential for social vulnerability to explain at least some of this phenomenon. The results from our study suggest that perhaps some of the social problems that have been documented for these populations may be better understood by assessing social vulnerability. However, these results should be interpreted with caution as this was not intended to be a clinical study. Rather, by looking at the small samples provided within the broader national sample, the results indicate the potential clinical application of social vulnerability to understanding the social risk associated with a range of developmental and clinical disorders. Further research is required to determine whether social vulnerability can help explain social difficulties evident within these populations. The scale and normative data presented in this study will help to facilitate such research.
The current results also have theoretical implications, namely, that social vulnerability in elementary-school children is best represented by a single factor. The two-factor conceptualisation of social vulnerability (i.e., credulity and gullibility) proposed by Greenspan et al. (2001) did not emerge in the current study, even when a two-factor solution was forced, despite having items clearly representing both credulity and gullibility and a large sample with considerable variability. Rather, our results indicate that credulity and gullibility are part of the same factor, suggesting that the theoretical conceptualisation of social vulnerability described by Greenspan et al. (2001) is not applicable to children. It is possible that, for children, social vulnerability is a unitary construct, and that as individuals develop, the construct becomes more complex and delineates into two factors (credulity and gullibility) as seen in older adults (Pinsker et al., 2011). Further research conducted across the lifespan will be required to determine if this is in fact the case.
There are some limitations to the current study. Foremost, we had a low proportion of fathers in the study, and as such, the views expressed largely represent those of mothers. However, given that mothers are more commonly the primary caregiver (Australian Bureau of Statistics, 2013), we do not see this to be a major limitation. Additionally, although the study provides support for a relationship between social vulnerability and psychosocial functioning using both parent and teacher reports, future research would benefit from assessing a broader range of psychosocial functioning. Given that peer relationships are associated with children's quality of life (Huang, Wang, Tang, Chen, & Yu, 2017), studies incorporating measures of this construct would also be beneficial. This would to enable us to gain a more comprehensive understanding of the relationship between social vulnerability and specific aspects of children's psychosocial functioning and their quality of life more broadly.
Additionally, parents’ reports of social vulnerability and other behaviours were largely relied on in the current study. Whilst preliminary support was provided for the teacher rating form of the CSVQ, further evaluation of this form would be beneficial to enable a multi-informant approach to assessing social vulnerability, as well as the identification of socially vulnerable children within the school setting and implementation of protective strategies to reduce risk for them.
ConclusionsBeing vulnerable to deception has been hypothesised to play an important role in children's daily social interchanges. The results of this study support the use of the CSVQ as a brief and psychometrically sound instrument for measuring perceptions of social vulnerability in children. Importantly, the results indicate that social vulnerability is a psychosocial construct that is distinct from other aspects of children's emotional and behavioural adjustment, and their social skills. Furthermore, the results highlight the potential for the CSVQ to provide us with greater insight into the social exchanges of both typically developing and clinical groups of children who are known to experience social problems. The current study contributes to a developing body of knowledge about social vulnerability during childhood. Comprehensive and reliable normative data are provided, which will enable professionals working within clinical psychology and education to assess a child's level of social vulnerability, and identify at-risk children. In doing so, strategies could be implemented to protect these children from potentially harmful social interactions.
FundingThis work was supported by the School of Psychology, The University of Western Australia, Crawley, Western Australia, Australia.
To assess whether additional demographic variables needed to serve as covariates, relationships between the demographic variables (i.e., number of children, marital status, ethnicity, average annual income, school type) and social vulnerability were explored. ANOVA's demonstrated that there was no main effect of any of these demographic variables on social vulnerability scores (all ps > .05).
