



Background/Objective: It is essential to carry out a diagnosis of people’s healthy lifestyles, in order to apply strategies to improve them. The aim of the study was to validate the Healthy Lifestyles Questionnaire (CEVS-II), collecting all factors that make up the concept of a healthy lifestyle, such as a balanced diet, respect for mealtimes, tobacco consumption, rest habits, alcohol consumption, other drug use and physical activity. Method: The questionnaire was completed by 1,132 people between 18 and 89 (M = 42.43; SD = 18.69) years from different parts of Spain. Results: The seven-factor model proposed by the Confirmatory Factor Analysis, according to the goodness indices, presented an acceptable fit (SRMR = .059; CFI = .973; RMSEA = .049; 90% CI [.046, .052]; χ2/df = 3.76), also presented good reliability indices and was endowed with concurrent validity. Conclusions: The results of the present study proved the validity and reliability of the Healthy Lifestyles Questionnaire in a Spanish population, which is an adequate instrument for the diagnosis of a healthy lifestyles in the Spanish population.
Antecedentes/Objetivo: Resulta primordial realizar un diagnóstico de los estilos de vida saludables de las personas, con el fin de aplicar estrategias para la mejora de estos. El objetivo del estudio fue validar el Cuestionario de Estilos de Vida Saludables (CEVS-II), recogiendo todos los factores que componen el concepto de estilo de vida saludable como son la alimentación equilibrada, el respeto al horario de las comidas, el consumo de tabaco, los hábitos de descanso, el consumo de alcohol, el consumo de otras drogas y la práctica de actividad física. Método: El cuestionario fue cumplimentado por 1.132 personas de 18-89 (M = 42,43; DT = 18,69) años de diferentes partes de España. Resultados: El modelo de siete factores propuesto por el Análisis Factorial Confirmatorio presentó un ajuste aceptable (SRMR = 0,059; CFI = 0,973; RMSEA = 0,049; 90% CI [0,046 - 0,052]; χ2/df = 3,76), buenos índices de fiabilidad y de validez concurrente. Conclusiones: Los resultados del presente estudio probaron la validez y fiabilidad del Cuestionario de Estilos de Vida Saludables en una muestra española, dando lugar a un instrumento adecuado para la medición de estilos de vida saludables en la población española.
It is a well-established fact that living a healthy lifestyle (HLS) is important from an early age (Arriscado et al., 2017). This includes engaging in habits related to balanced nutrition (balanced diet and respect for meal schedules) (Aparicio-Ugarriza et al., 2019), practice of physical exercise (Jakicic et al., 2018), and optimal rest (Onambele-Pearson et al., 2019) and, in contrast, avoiding a sedentary lifestyle, lack of rest, smoking, drug use and excessive alcohol intake (Meredith et al., 2018). Harmful lifestyle habits such as a sedentary lifestyle, unbalanced diet, lack of rest, and the use of harmful substances are, in the long term, associated with diseases such as obesity, type II diabetes, hypercholesterol, and even cancer, thus leading to a premature increase in morbidity (Dunton, 2018; Ezzati & Riboli, 2013). Growing evidence from studies has found that a combination of these positive health-related behaviors decreases the risk of mortality from all causes (Olds et al., 2018), as healthy behaviors, such as physical activity, are shown to be associated with other behaviors such as eating a balanced diet and appropriate resting habits (Olds et al., 2018).
It is necessary, and increasingly incipient, for different health promoters such as doctors, physiotherapists, physical activity professionals, and social agents to be able to measure HLS given an increasingly large number of studies advocate the need to describe and improve the HLS of the population in its different stages (Arriscado et al., 2017; Llorent-Bedmar & Cobano-Delgado, 2019). Therefore, developing affordable and easy-to-apply instruments for health workers and social actors to measure HLSs across the population is vitally important, as these will enable problems to be diagnosed and individualized and/or collective programs to be created to improve healthy behaviors.
Several questionnaires have been developed in Spain to measure specific behaviors associated with an HLS. However, at the national level, a questionnaire that measures all associated factors (balanced diet, physical activity practice, rest habits, tobacco, alcohol, and other drugs), which would be useful for programs that assess multiple factors included in a global HLS, is lacking. As such, most recent studies have used multiple questionnaires to measure the various factors of an HLS (García-Hermoso et al., 2020; Gil-Madrona et al., 2019; Saavedra et al., 2014), which requires longer intervention times.
Most past research considers motivation as a key element in achieving adherence to an HLS . Self-Determination Theory (SDT; Deci & Ryan, 1980, 1985, 1991, 2012; Ryan & Deci, 2020) is used as a theoretical model for explaining this adherence. SDT proposes that motivation is framed along a continuum with three levels (Vansteenkiste et al., 2006, 2010): intrinsic motivation (the most self-determined, performing an activity for its own sake), extrinsic motivation (from more to less self-determined includes integrated, identified, introjected and external regulation, and are determined by external rewards or recognitions) and amotivation (the least self-determined, lack of intent to act) (Deci & Ryan, 2000).
Research has shown that an intrinsic motivation towards the practice of physical activity will maintain the intention to continue practicing for longer (Kang et al., 2019; Lee, 2018), and that, in turn, practice of physical activity will trigger the acquisition of other healthy habits (Carbó-Carreté et al., 2016; Chacón-Cuberos et al., 2018; Rodrigues et al., 2018). Studies such as those of Leyton et al. (2020), Scoffier-Mériaux et al. (2020), and Vancampfort et al. (2018) have assessed motivation, measured using the Behavioural Regulation in Exercise Questionnaire (BREQ-3) (Wilson et al., 2006), and tested its association with health behaviors such as the intention to be physically active, eating habits, and consumption of harmful substances, respectively. Leyton et al. (2020), for example, found relationships between motivation and intention to be physically active (IPA) via structural equation modelling of the BREQ-3 questionnaire and a Measure of the Intentionality of Being Physically Active (MIBPA; Hein et al., 2004).
Identifying individuals’ level of motivation and determining the influence of the context associated with their behaviors and choices, can improve interventions aimed at changing lifestyles, as suggested by the results of studies using SDT in relation to health (Silva et al., 2015).
In sum, according to the literature reviewed, it is necessary to develop an easy to apply questionnaire that measures all the dimensions of an HLS. The objective of this study was to validate, for the Spanish context, the Healthy Lifestyle Questionnaire (Cuestionario de Estilos de Vida Saludables, CEVS-II), which measures eating habits, rest habits, tobacco, alcohol and other drug use, and practice of physical activity. In addition, evidence of validity will be assessed based on the relationship between CEVS-II scores and other theoretically related variables, such as the different types of self-determined motivation and the intention to be physically active. Several hypotheses were made: (1) the CEVS-II will present adequate goodness-of-fit indices and reliability, (2) the eating habits, practice of physical activity, and rest habits dimensions will be positively and significantly linked to the most self-determined form of motivation towards physical activity and intention to be physically active; and (3) the consumption of tobacco, alcohol and other drugs dimensions will be negatively and significantly related to the most self-determined form of motivation towards physical activity and intention to be physically active.
MethodParticipantsThe sample comprised 1,132 individuals (54.90% male and 45.10% female) from various regions in Spain. These individuals were recruited using intentional sampling. The sample had an age range of 18 to 89 years (M = 42.43, SD = 18.69). Overall, 663 individuals were from urban regions and 469 were from rural regions (with rural regions defined as those with populations of 2,500 inhabitants or fewer, and urban zones with populations greater than 2,500 inhabitants). To be eligible for the study participants had to be adults, Spanish by nationality and could not have any form of physical or mental disability.
InstrumentsThe Healthy Lifestyle Questionnaire (Cuestionario de Estilos de Vida Saludables; CEVS-II). The 27 items of this instrument are grouped into seven factors: Balanced diet (3 items; e.g., "I normally eat fish 2 or more times a week"), Respect for meal schedules (3 items; e.g., "I usually respect the schedule of the main meals of the day"); Rest habits (3 items; e.g., "I usually sleep 7 or 8 hours a day"); Tobacco consumption (3 items; e.g., "I feel good when I smoke"); Alcohol consumption (5 items; e.g., "I think alcohol makes me feel good"); Consumption of other drugs (5 items; e.g., "I find it easy to get some drugs") and Physical activity (5 items; e.g., "I consider myself a physically active person").
To measure the level of self-determined motivation we used the Behavioral Regulation in Exercise Questionnaire (BREQ-3); Wilson et al., 2006), which was validated for the Spanish context by González-Cutre et al. (2010). This questionnaire consists of an introductory phrase "I exercise physically…", followed by 23 items that capture different types of motivation: Intrinsic Regulation (4 items; e.g., "…because I think physical exercise or sport is fun"), Integrated regulation (4 items; e.g., "…because I consider physical exercise or sport to be part of me"), Identified regulation (3 items; e.g., "…because I value the benefits of physical exercise or sport"), Introjected regulation (4 items; e.g. "…because I feel guilty when I don't practice it"), External regulation (4 items; e.g. "…because others tell me I should do it") and Amotivation (4 items; e.g., "…I don't see why I have to). This factor structure was shown to have adequate fit: SRMR = .06; CFI = .91; RMSEA = .06; χ2/df = 3.20.
To measure intention to be physically active we used the Measure of the Intentionality of Being Physically Active (MIBPA), which was developed by Hein et al. (2004) and validated in Spanish by Moreno-Murcia et al. (2007). This questionnaire is formed of five items that load on a single factor: intention to be physically active (e.g., “I am interested in developing my physical form”). This factor structure was shown to have good fit: SRMR = .04; CFI = .97; RMSEA = .08; χ2/df = 1.80.
Responses to the questionnaires were recorded on a five-point Likert-type scale that ranged from 1 (Totally disagree) to 5 (Totally agree) with the formulation of the item.
ProcedureThe study was granted approval by the Commission of Bioethics and Biosafety of the University of Extremadura (Spain), following the recommendations from the Helsinki declaration. All participants were treated in accordance with the American Psychological Association's ethical guidelines regarding participant consent, confidentiality, and anonymity.
Once the objectives of the study and measures were defined; the main instrument, the CEVS-II, was developed following the recommendations of Muñiz and Fonseca-Pedrero (2019). This instrument comprised the 12 items for the factors of the Leyton et al. (2018) questionnaire and additional items to measure the dimensions alcohol consumption, consumption of other drugs, and practice of physical exercise. For each of these new factors we proposed an initial six items, which were then analyzed by a group of five experts in Physical Activity and Sport Sciences, and two Psychologists, resulting in five items per new factor. Ultimately, the CEVS-II questionnaire comprised a total of 27 items.
Finally, a battery of the different questionnaires was prepared, including additional measures of sociodemographic variables such as gender, age, and region. The battery of questionnaires was then uploaded to the Google Form platform. Participants completed the battery of questionnaires individually online, accessed through different mediums (WhatsApp, Facebook, Twitter, and email). It took approximately 10-15 minutes to complete all questionnaires. The online form also included information about the investigation, informed consent, and instructions on how to respond to the questionnaire. It also included a contact phone number and email address to resolve any questions. No doubts or missing values were reported.
Statistical analysisFirst, we used confirmatory factor analysis (CFA) to test structural validity. Because the endogenous variables were ordinal, we used a robust weighted least squares estimators (WLSMV), which is designed specifically for ordinal data (Li, 2016). For each latent factor, the loading of the first element was restricted to 1. We report standardized estimates despite using unstandardized parameters in the model. To evaluate the goodness of fit of this model we used (a) the χ2/df ratio, which is recommended to be ≤ 5 (Schumaker & Lomax, 2010); the comparative fit index (CFI), which is recommended to be ≥ .95 (Cangur & Ercan, 2015); (c) the root mean square error of approximation (RMSEA), for which values < .08 indicate acceptable fit (Browne & Cudeck, 1992); and (d) the standardized root mean square residual (SRMR), for which values < .08 indicate acceptable fit and < .05 indicate good fit (Schermelleh-Engel et al., 2003). We used a multigroup CFA approach to test the psychometric equivalence of EVS across (a) gender, and (b) age group. For age group we split the sample into two groups representing older (> 40 years) and younger (≤ 40 years) participants using a median split method. For this analysis we used the MLR estimator. In this approach, testing nested models with increasing numbers of parameter restrictions allows for an assessment of configural, metric, and scalar invariance. Configural invariance tests the extent to which the model fits across the global sample. Metric invariance (with loadings constrained across groups) tests the extent to which items load on the factors similarly across groups. Finally, scalar invariance (with loadings and intercepts constrained across groups) tests whether sample means can be meaningfully compared across groups. We determined invariance by examining changes in various alternative fit indices because these are typically less sensitive to sample size (Putnick & Bornstein, 2016). Typically, a criterion of a -.01 change in CFI paired with change in RMSEA of .015 and SRMR of .030 for metric invariance or .015 for scalar invariance is used as an indication of invariance (Chen, 2007).
We performed a descriptive analysis of scale means, skew, and kurtosis, as well as an analysis of internal consistency via the calculation of omega coefficients (McDonald, 1999). Finally, to determine concurrent validity, we calculated bivariate Pearson’s correlations between the factors of the CEVS-II and those of the BREQ-3 and MIBPA.
We conducted the CFA analyses using the lavaan package (Rosseel, 2012) in R. MPlus 7.11 (Muthén & Muthén, 2014) was used to test the seven-factor model. We used SPSS 21.0 (IBM-SPSS Inc, Chicago, IL) to perform descriptive analysis and calculate correlations.
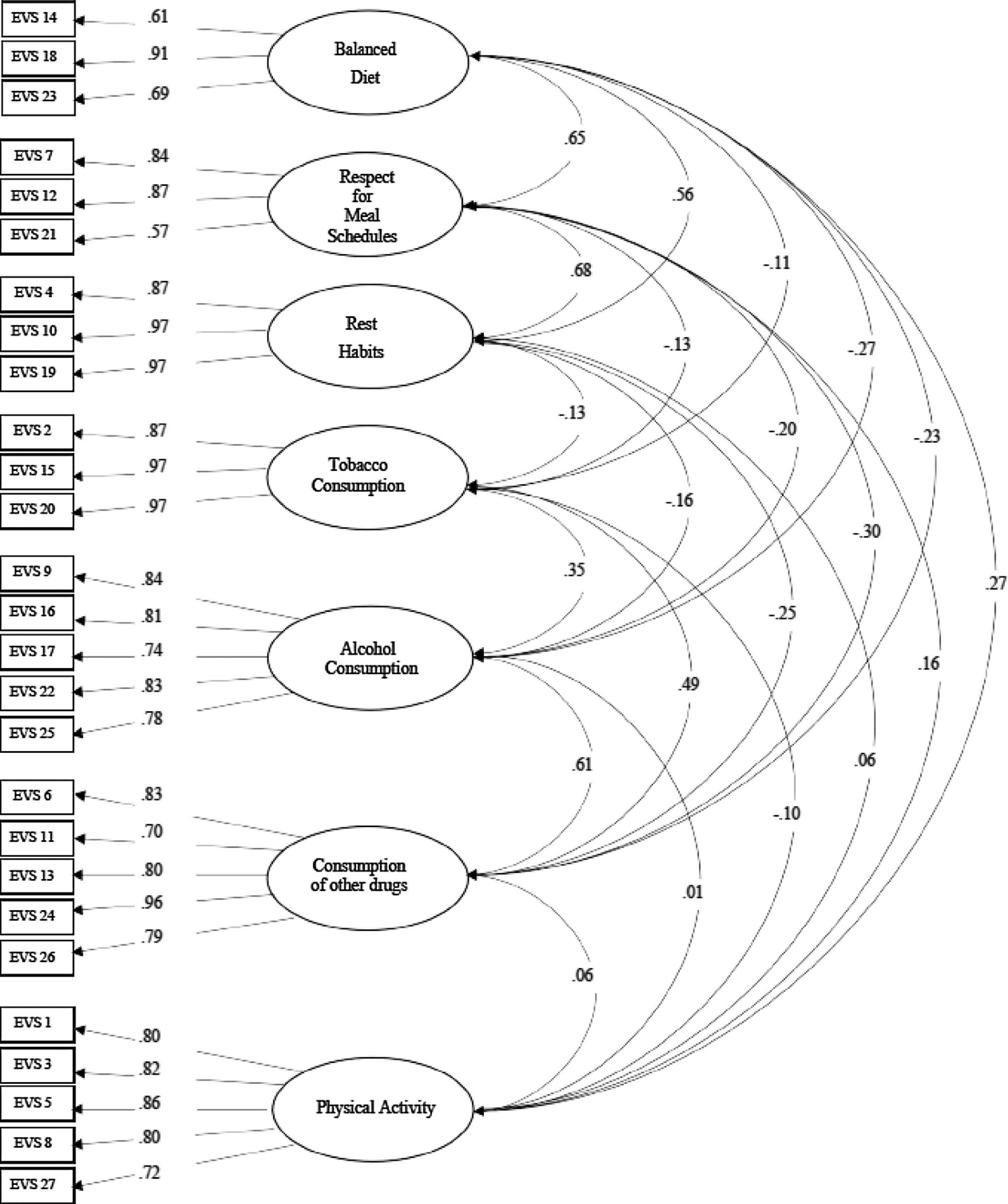
ResultsConfirmatory Factor AnalysisAccording to fit indices, the correlated six-factor model had acceptable fit: SRMR = .059; CFI = .973; RMSEA = .049; 90% CI [.046 - .052]; χ2/df = 3.76. As can be seen in Fig. 1, the standardized factor loadings had moderate to strong values, ranging from .57 to .97. Most of the latent factor correlations were weak, with the exceptions of Balanced diet with Respect for meal schedules (.65), Balanced diet and Rest habits (.56), Respect for meal schedules and Rest habits (.68), and Alcohol consumption and Consumption of other drugs (.61).
Measurement invariance and rectangles represent indicators (items).")
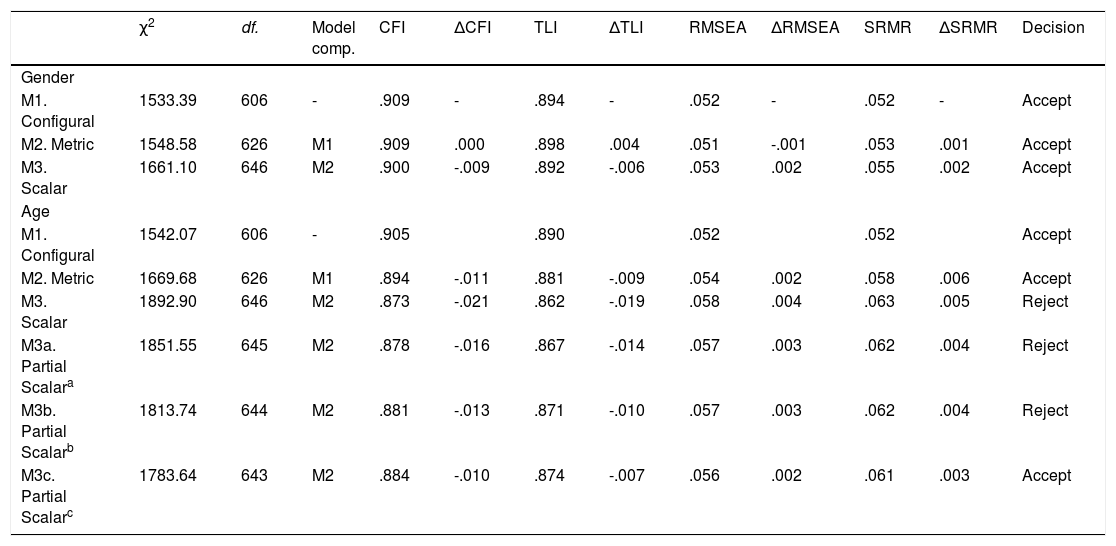
Values for the fit indices in each of the multigroup models are shown in Table 1. Overall, the changes observed for CFI, TLI, RMSEA, and SRMR across models supported scalar invariance in males and females. Scalar measurement invariance in older and younger participants was only supported partially after freeing the constraints on intercepts for items 3, 17, and 22.
Fit indices for configural, metric, and scalar models testing measurement invariance of the CEVS-II
| χ2 | df. | Model comp. | CFI | ΔCFI | TLI | ΔTLI | RMSEA | ΔRMSEA | SRMR | ΔSRMR | Decision | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||||||
| M1. Configural | 1533.39 | 606 | - | .909 | - | .894 | - | .052 | - | .052 | - | Accept |
| M2. Metric | 1548.58 | 626 | M1 | .909 | .000 | .898 | .004 | .051 | -.001 | .053 | .001 | Accept |
| M3. Scalar | 1661.10 | 646 | M2 | .900 | -.009 | .892 | -.006 | .053 | .002 | .055 | .002 | Accept |
| Age | ||||||||||||
| M1. Configural | 1542.07 | 606 | - | .905 | .890 | .052 | .052 | Accept | ||||
| M2. Metric | 1669.68 | 626 | M1 | .894 | -.011 | .881 | -.009 | .054 | .002 | .058 | .006 | Accept |
| M3. Scalar | 1892.90 | 646 | M2 | .873 | -.021 | .862 | -.019 | .058 | .004 | .063 | .005 | Reject |
| M3a. Partial Scalara | 1851.55 | 645 | M2 | .878 | -.016 | .867 | -.014 | .057 | .003 | .062 | .004 | Reject |
| M3b. Partial Scalarb | 1813.74 | 644 | M2 | .881 | -.013 | .871 | -.010 | .057 | .003 | .062 | .004 | Reject |
| M3c. Partial Scalarc | 1783.64 | 643 | M2 | .884 | -.010 | .874 | -.007 | .056 | .002 | .061 | .003 | Accept |
Nota. df= degrees of freedom; aFree intercept for item 17;bFree intercepts for items 17 and 22; cFree intercepts for items 17, 22, and 3.
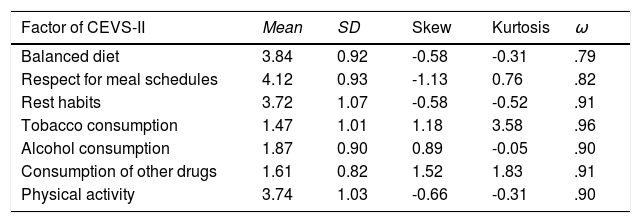
According to the rules of normality proposed by Curran et al. (1996), all the variables had univariate normality, as shown by skew values < 2 and kurtosis values < 7. McDonald’s omega coefficients are shown in Table 2.
Descriptive statistics and reliability analysis of CEVS-II factors.
| Factor of CEVS-II | Mean | SD | Skew | Kurtosis | ω |
|---|---|---|---|---|---|
| Balanced diet | 3.84 | 0.92 | -0.58 | -0.31 | .79 |
| Respect for meal schedules | 4.12 | 0.93 | -1.13 | 0.76 | .82 |
| Rest habits | 3.72 | 1.07 | -0.58 | -0.52 | .91 |
| Tobacco consumption | 1.47 | 1.01 | 1.18 | 3.58 | .96 |
| Alcohol consumption | 1.87 | 0.90 | 0.89 | -0.05 | .90 |
| Consumption of other drugs | 1.61 | 0.82 | 1.52 | 1.83 | .91 |
| Physical activity | 3.74 | 1.03 | -0.66 | -0.31 | .90 |
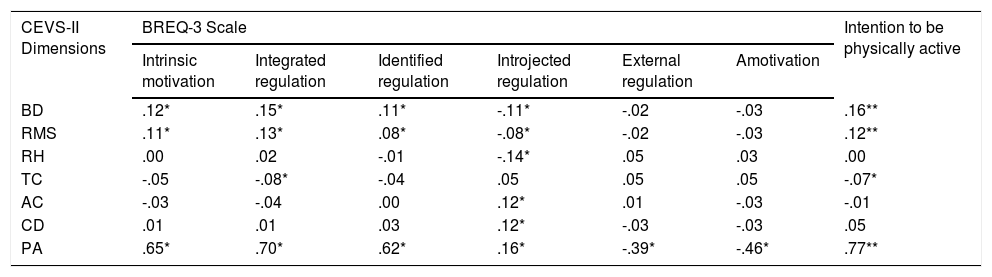
The output of the correlational analysis is shown in Table 3.
Pearson correlations between factors of the CEVS-II, BREQ-3 and MIBPA.
| CEVS-II Dimensions | BREQ-3 Scale | Intention to be physically active | |||||
|---|---|---|---|---|---|---|---|
| Intrinsic motivation | Integrated regulation | Identified regulation | Introjected regulation | External regulation | Amotivation | ||
| BD | .12* | .15* | .11* | -.11* | -.02 | -.03 | .16** |
| RMS | .11* | .13* | .08* | -.08* | -.02 | -.03 | .12** |
| RH | .00 | .02 | -.01 | -.14* | .05 | .03 | .00 |
| TC | -.05 | -.08* | -.04 | .05 | .05 | .05 | -.07* |
| AC | -.03 | -.04 | .00 | .12* | .01 | -.03 | -.01 |
| CD | .01 | .01 | .03 | .12* | -.03 | -.03 | .05 |
| PA | .65* | .70* | .62* | .16* | -.39* | -.46* | .77** |
This study analyzed the validity of the Healthy Lifestyle Questionnaire (CEVS-II), which itself was based on a measure presented by Leyton et al. (2018). Our first hypothesis was supported, as the factorial structure and validity of the questionnaire was satisfactory. Specifically, the results of the CFA revealed that the structure was adequate, as shown by acceptable fit indices and McDonald's omega coefficients showed high levels of internal consistency. Such findings confirm that a questionnaire has been developed for the Spanish population that includes all the essential dimensions that make up a healthy lifestyle (Aparicio-Ugarriza et al., 2019; Jakicic et al., 2018; Meredith et al., 2018; Onambele-Pearson et al., 2019).
The second study hypothesis was partially met. In accordance with expectation, the Balanced diet, Respect for meal schedules, and Practice of physical activity dimensions were positively and significantly correlated with the most self-determined forms of motivation towards the practice of physical activity and intention to be physically active. However, the same was not true of the Rest habits factor. Recent studies, such as those of Monteiro et al. (2019) and Onambele-Pearson et al. (2019), reflect the close relationship observed between the practice of physical activity and healthy eating habits. Intrinsic motivation towards is an important factor towards the practice of physical activity (Rodrigues et al., 2018), and it is therefore important that people have high level of self-determined motivation towards such practice as this will lead them to adopt other habits, such as eating a balanced diet (Durocher & Gauvin, 2020; Teixeira et al., 2020). Similarly, as demonstrated by studies such as Wheatley et al. (2020), the practice of physical activity appeared to be positively correlated with intention to be physically active. The Rest Habits dimension was not significantly correlated with the most self-determined forms of motivation toward physical activity practice or intention to be physically active. Other studies, however, have demonstrated, in contrast to our results, that these variables are related. Leyton et al.'s study (2020), for example, found that intrinsic motivation predicts health-related lifestyle-related variables, such as proper rest habits. As for the relationship between rest and the intention to be physically active, positive relationships have also been found between the practice of physical activity, measured through the IPAQ Questionnaire (Roman et al., 2010), and adequate resting habits (Leyton et al., 2020), unlike in this study.
We conclude that the third hypothesis was not confirmed, as only tobacco consumption displayed significant negative correlations with integrated regulation and intention to be physically active, and even these correlations were weak. However, this contrasts with studies such as Mora et al. (2019) that found a relationship between being physically active and lower alcohol consumption, and Castro-Sánchez et al. (2017) that found a relationship between being physically active and not being a smoker.
Although the CEVS-II was validated for a population with a wide age range, in the future it could be applied to groups of people with specific pathologies to (a) determine the validity of the questionnaire in these groups, and (b) whether it might be useful for assessing the type of lifestyle held by these groups after an intervention program, after surgery, or even as a diagnosis tool for patients. It would be interesting to see if CEVS-II dimensions predict other psychological variables to generate strategies that can help people lead healthier lifestyles. One possible limitation of the results is the observed weak correlations between the CEVS-II dimensions (apart from physical activity) and the most self-determined motivation and intention to by physically active. The failure to achieve full scalar invariance across the two age groups may also be a limitation. Another limitation is the use of an online questionnaire and the lack of standardization of the sample reflected in the plurality of zones and ages of the participants. As such, it would be interesting to determine the psychometric properties of the questionnaire in specific region and with distinct age groups, as well as in other countries.
In conclusion, the results of this study tested the validity and reliability of CEVS-II (see Appendix A) in a Spanish population of 18 to 89 years.
FundingThis study was conducted through the contribution of the Ministry of Economy and Infrastructure of the Junta de Extremadura, through the European Regional Development Fund. A way to do Europe (GR18129). This financial aid was received by Ruth Jiménez Castuera, the only author from the University of Extremadura.
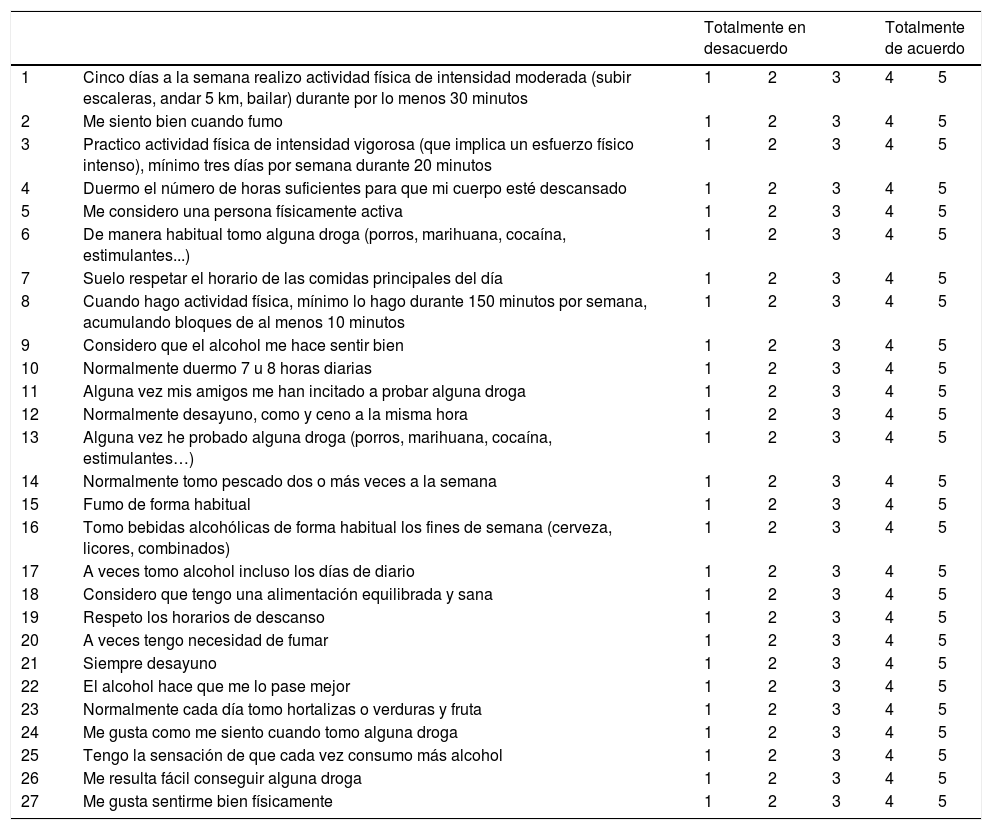
| Totalmente en desacuerdo | Totalmente de acuerdo | |||||
|---|---|---|---|---|---|---|
| 1 | Cinco días a la semana realizo actividad física de intensidad moderada (subir escaleras, andar 5 km, bailar) durante por lo menos 30 minutos | 1 | 2 | 3 | 4 | 5 |
| 2 | Me siento bien cuando fumo | 1 | 2 | 3 | 4 | 5 |
| 3 | Practico actividad física de intensidad vigorosa (que implica un esfuerzo físico intenso), mínimo tres días por semana durante 20 minutos | 1 | 2 | 3 | 4 | 5 |
| 4 | Duermo el número de horas suficientes para que mi cuerpo esté descansado | 1 | 2 | 3 | 4 | 5 |
| 5 | Me considero una persona físicamente activa | 1 | 2 | 3 | 4 | 5 |
| 6 | De manera habitual tomo alguna droga (porros, marihuana, cocaína, estimulantes...) | 1 | 2 | 3 | 4 | 5 |
| 7 | Suelo respetar el horario de las comidas principales del día | 1 | 2 | 3 | 4 | 5 |
| 8 | Cuando hago actividad física, mínimo lo hago durante 150 minutos por semana, acumulando bloques de al menos 10 minutos | 1 | 2 | 3 | 4 | 5 |
| 9 | Considero que el alcohol me hace sentir bien | 1 | 2 | 3 | 4 | 5 |
| 10 | Normalmente duermo 7 u 8 horas diarias | 1 | 2 | 3 | 4 | 5 |
| 11 | Alguna vez mis amigos me han incitado a probar alguna droga | 1 | 2 | 3 | 4 | 5 |
| 12 | Normalmente desayuno, como y ceno a la misma hora | 1 | 2 | 3 | 4 | 5 |
| 13 | Alguna vez he probado alguna droga (porros, marihuana, cocaína, estimulantes…) | 1 | 2 | 3 | 4 | 5 |
| 14 | Normalmente tomo pescado dos o más veces a la semana | 1 | 2 | 3 | 4 | 5 |
| 15 | Fumo de forma habitual | 1 | 2 | 3 | 4 | 5 |
| 16 | Tomo bebidas alcohólicas de forma habitual los fines de semana (cerveza, licores, combinados) | 1 | 2 | 3 | 4 | 5 |
| 17 | A veces tomo alcohol incluso los días de diario | 1 | 2 | 3 | 4 | 5 |
| 18 | Considero que tengo una alimentación equilibrada y sana | 1 | 2 | 3 | 4 | 5 |
| 19 | Respeto los horarios de descanso | 1 | 2 | 3 | 4 | 5 |
| 20 | A veces tengo necesidad de fumar | 1 | 2 | 3 | 4 | 5 |
| 21 | Siempre desayuno | 1 | 2 | 3 | 4 | 5 |
| 22 | El alcohol hace que me lo pase mejor | 1 | 2 | 3 | 4 | 5 |
| 23 | Normalmente cada día tomo hortalizas o verduras y fruta | 1 | 2 | 3 | 4 | 5 |
| 24 | Me gusta como me siento cuando tomo alguna droga | 1 | 2 | 3 | 4 | 5 |
| 25 | Tengo la sensación de que cada vez consumo más alcohol | 1 | 2 | 3 | 4 | 5 |
| 26 | Me resulta fácil conseguir alguna droga | 1 | 2 | 3 | 4 | 5 |
| 27 | Me gusta sentirme bien físicamente | 1 | 2 | 3 | 4 | 5 |
Note. Blanced meal (items 14, 18, 23), Respect for meal schedules (items 7, 12, 21), Rest habits (items 4, 10, 19), Tobacco consumption (items 2, 15, 20), Alcohol consumption (items 9, 16, 17, 22, 25), Consumption of other drugs (items 6, 11, 13, 24, 26) y Physical activity (items 1, 3, 5, 8, 27).
