



Empathy is the mediating role of the physician–patient relationship. Through this process the practitioner seeks to understand the patient's frame of reference and also to establish a relationship of openness, mutual respect, trust and deep understanding.
ObjectiveThis study aims to analyze the perceptions of medical students on the importance of empathy in the doctor–patient relationship, and to analyze the gender differences and in the different years of the course. It is also intended to identify a taxonomy of students based on their perceptions of empathy.
MethodsThis cross-sectional study was conducted on undergraduate medical students. A total of 208 medical students responded to the Jefferson Scale of Physician Empathy–Student Portuguese Version (JSPE-spv). Principal Components Analysis with varimax rotation was used to identify the number and compositions of emerged factors. The scores of the retained factors were submitted to a cluster analysis to identify different groups of students, based on the dimension of empathy. A One-way Anova analysis and post-hoc tests of Tukey supported the identified cluster.
ResultsThis study shows statistically significant differences between genders, i.e., female individuals show higher scores than male individuals. Empathy increases over the course, but with no statistically significant differences. Six factors emerged from factor analysis, and three of them are empathy dimensions found in other studies: “adoption of perspectives”, “compassionate care”, and “standing in the patients shoes”. Cluster analysis divided the students into five groups according to the dimensions of empathy identified.
ConclusionsIn this medical school in Portugal, it may be concluded that women are more empathetic than men, and empathy grows throughout the course. It is recommended to carry out a longitudinal study, in order to follow the evolution of these students, as well as to analyze factors that contribute to the increase in empathy characteristics.
La empatía es el papel mediador de la relación médico-paciente. A través de este proceso el profesional busca entender el marco de referencia del paciente y también para establecer una relación de transparencia, el respeto mutuo, la confianza y la comprensión profunda.
ObjetivoEste estudio tiene como objetivo analizar las percepciones de los estudiantes de medicina acerca de la importancia de la empatía en la relación médico-paciente y analizar la existencia de diferencias de género y en los diferentes años de la carrera. También se pretende identificar una taxonomía de los estudiantes basada en sus percepciones de la empatía.
MétodoEste estudio transversal se llevó a cabo entre los estudiantes de pregrado de medicina. Un total de 208 estudiantes de medicina respondió a la Escala Jefferson de empatía médica del estudiante versión en portugués. Se utilizó análisis de componentes principales con rotación varimax para identificar el número y composición de factores surgido. Las puntuaciones de los factores retenidos fueron sometidos a un análisis de clusters para identificar diferentes grupos de estudiantes basados en la dimensión de la empatía. Un análisis Oneway-ANOVA y los test post-hoc de Tukey han soportado la agrupación identificada.
ResultadosEste estudio presenta diferencias estadísticamente significativas entre los géneros, es decir, los individuos femeninos revelan puntuaciones más altas que los individuos de sexo masculino, la empatía aumenta durante el curso, pero sin diferencias estadísticamente significativas. Seis factores emergieron del análisis factorial y tres de ellos son dimensiones de empatía que se encuentran en otros estudios: «la adopción de perspectivas», «atención humanitaria» y «colocarse en lugar de los otros». El análisis de clusters divide a los alumnos en cinco grupos, de acuerdo con las dimensiones de la empatía identificadas.
ConclusionesEs posible concluir que, en esta escuela de medicina en Portugal, las mujeres son más empáticas que los hombres, y, a medida que atraviesan los diferentes años en el curso en general, la empatía crece. Se recomienda llevar a cabo un estudio longitudinal, con el fin de seguir la evolución de estos estudiantes y analizar los factores que contribuyen para el aumento de las características de empatía.
Empathy has been described in literature as the most frequently mentioned attribute of the humanistic physician.1 Since it is a term considered ambiguous, several attempts emerged over the time to define this concept.
Several researchers presented similar definitions for empathy. Gianakos2 described empathy as “the ability of physicians to imagine that they are the patient who has come to them for help.”
This definition includes four dimensions: emotive (ability to imagine patients’ emotions/perspectives); moral (physicians’ internal motivation to empathize); cognitive (intellectual ability to identify and understand patients’ emotions/perspectives); behavioral (ability to convey understanding of those emotions and perspectives back to the patient).3,4
Hojat5 defines empathy as one of the most important ingredients in creating a good relation between physician and patient. This author presents this concept in the context of patient care as follows: “empathy is a predominantly cognitive (rather than emotional) attribute that involves an understanding (rather than feeling) of experiences, concerns and perspectives of the patient, combined with a capacity to communicate this understanding.”
Kohut emphasizes the importance of empathy as an observational method tuned to the man's inner life and experience as close to the activity of collecting information and how powerful emotional bond between people.6 Evidence-based studies showed that effective empathetic patient care is associated with improved health care outcomes.
Empathy consists in the ability and capacity of the doctor to walk himself in the patient's shoes and see the world from their perspective and then be able to convey this understanding verbal and nonverbal, and it is important that the physician keeps track of himself, keeping an emotional distance so as not to interfere with their professional responsibilities and obligations.2
Considering empathy as a cognitive trait or attribute desirable in practitioners, we can question the desirability of making an assessment related to the existence of this construct along the learning or even implement it as an integral aspect of the admission of students to medical school. In a study by Hemmerdinger,7 where the author conducted a literature review on the application of empathy measuring tests in physicians and medical trainees, it was concluded that empathy is a quality that is relevant.
Aiming at the development of a proper assessment tool for evaluating the level of empathy in medical students, Hojat et al.,8,9 researchers at Jefferson Medical College in the United States, created the Student Version of Jefferson Scale of Physician Empathy. This scale, including 20 items to measure the three underlying constructs of empathy (compassionate care, perspective taking and standing in patient's shoes), has proven to have satisfactory psychometric properties.
Using the JSPE-sv several interesting findings have been reported, for example, it is possible to analyze scores according to gender, specialty, and evolution of empathy over the years of medical school and similarities and differences among the countries.10 The differences among the countries suggested that cultures or medical education systems influence measurements and outcomes of empathy.5
Some studies show that the empathy mean scores decline during university medical education.11–15 However, more recently, other studies present results where this decrease is not observed. For example, in Japan, Korea and Portugal the levels of empathy increase in senior students.16–18 In the study with Iranian medical students, the empathy increases from the 3rd year and there was a decrease from the 1st to the 2nd year.19 This finding seems to be the opposite of Hojat's longitudinal findings which showed that a significant decline occurs in the third year of medical school.15
All studies present the same conclusions about female and male differences of empathy mean scores. Women obtain higher scores of empathy than men.5,9,10,13,16,18,20–23
The purpose of this study was to analyze the perception of medical students about the importance of empathy in the physician–patient relationship and to verify the existence of differences in gender and the evolution over the course. It is also intended to identify a taxonomy of students based on their perceptions of empathy. In this study we tested three hypotheses: H1 – female medical students show higher scores of empathy than men. H2 – medical students scores of empathy decline over the course. H3 – based on the dimensions of empathy identified it is possible to find a taxonomy of students with different emphasis related to the empathy.
MethodsParticipants312 medical students were involved on a voluntary basis and have not been compensated for their participation, and students were assured about the confidentiality of their answers. Based on an on-line survey a total of 208 answers were returned.
InstrumentsThe instrument to measure empathy in medical students was based on the student version of the Jefferson Scale of Physician Empathy (JSPE-sv), which includes 20 items in a 7 point Likert-type scale (1 – strongly disagree, 7 – strongly agree).
The translation and adaptation of JSPE-sv was proposed in a Portuguese publication by Magalhães et al.24 There were 10 reverse items whose responses were scored accordingly, from 1 – strongly agree to 7 – strongly disagree. The total score was obtained by summing all items (maximum score=140), where higher values mean higher degrees of empathy.
Procedures and statistical analysisThe study was approved by the Dean of the Faculty of Health Sciences. The JSPE-spv was distributed to the selected population using the faculty mailing-list. The data collection was performed using a web, assuring the anonymity and confidentiality of the answers. The data was than submitted to a statistical analysis, descriptive and multivariate using the package SPSS – version 19.
The data analysis was conducted computing first the sum of the item total score of the JSPE-spv for two subsamples of female and male, calculating the mean and applying a t-test and an ANOVA Test to calculate the significance of the means of the different years students. Second, a factor analysis was performed following the next steps: (a) Bartlett's test of the sphericity and the KMO – Kaiser–Meyer–Olkin measure of sampling adequacy were determined to measure the goodness of factor analysis. (b) The principal component analysis was run to extract the number of components. (c) The retained components were submitted to a varimax rotation and following the criteria of eigenvalue >1,25 six main factors were retained. In addition, factor coefficients greater than 0.4 were used to make the interpretation of suggested components. To analyze the internal consistency of these factors the test of alpha Cronbach was used.
Third, using a cluster analysis we tried to find a taxonomy of students related with the different dimensions of empathy identified in factor analysis. To make this analysis, the scores of the retained factors are used instead of the original variables. Following the opinion of Douglas and Rhee26 this procedure was used with success in many studies. In fact, despite losing some information, however, shows the advantage of generating orthogonal dimensions for subsequent analysis. This reduces the potential problems resulting from the interdependence of the original data.
Using the method of Ward's clustering,25 we determined the number of clusters to retain, examining the dendogram and the decrease in the value of the sum of squared errors, as it passes from one group of cluster to another. Once chosen the number of groups were used as a validation, an analysis of variance Oneway-Anova, and the post-hoc tests of Tukey.
ResultsDescriptive analysisThe final sample was composed of 208 students who represent 66.6% of the population (Table 1). There were 148 females (71.2%) and 60 males (28.8%) and the age mean of the students was 21.38 years and standard deviation 2.77. Considering the years of enrollment, students are distributed as follows: 75 in the 1st year, 64 in the 3rd year and 67 in the 6th year.
In terms of comparison by gender (see Table 2) the empathy scores of female students (mean=116.41; SD=10.47) were higher than the scores of the male students (mean=109.45, SD=10.42; t=4.348, p<0.000). A statistically significant main effect for gender was found. Table 2 compares the results obtained from the demographic background of medical school year. As shown in the table, the empathy scores mean increases slowly from 112.85 in the first year, to 113.74 in the third year and to 116.78 in the sixth year. However, the Anova Test shows that there was no statistically significant effect.
Group comparison on scores of the JSPE-spv.
| Gendera | Mean | Standard deviation | Score minimum | Score maximum |
|---|---|---|---|---|
| Female (148) | 116.41 | 10.47 | 76.00 | 136.00 |
| Male (60) | 109.45 | 10.42 | 86.00 | 134.00 |
| Medical school yearb | Mean | Standard deviation | Score minimum | Score maximum |
|---|---|---|---|---|
| 1st year (144) | 112.85 | 10.46 | 86.00 | 131.00 |
| 3rd year (87) | 113.74 | 11.57 | 80.00 | 136.00 |
| 6th year (81) | 116.78 | 10.43 | 76.00 | 136.00 |
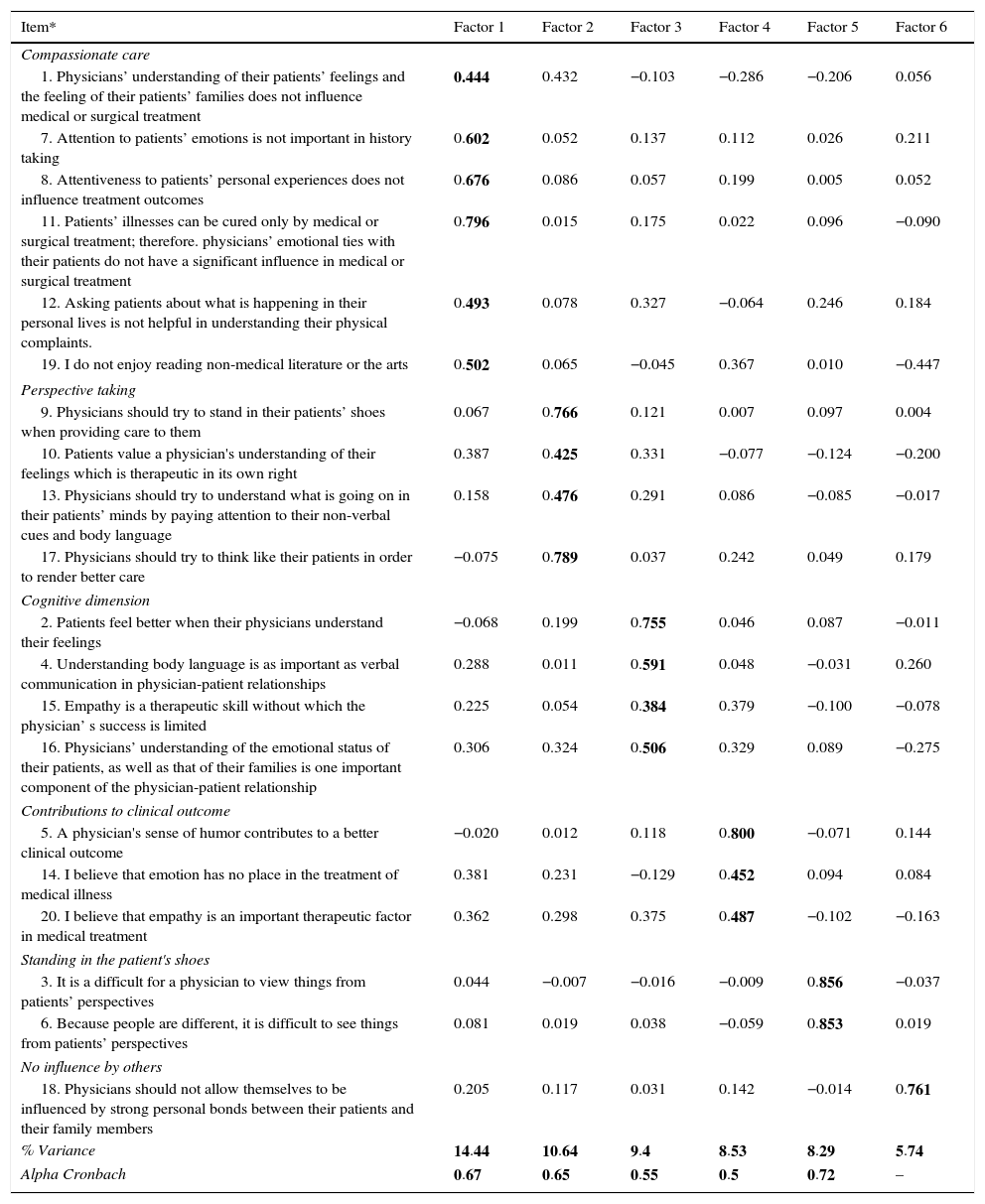
The summary results of factor analysis of data for the 20 items of JSPE-spv are reported in Table 3. As shown in Table 3 were retained six factors, each one with eigenvalue greater than 1, accounting for a total of 57.04% of a total variation before rotation. The acceptability test (KMO=0.788 and Bartlett Test=931.51, df=190, sig=0.000) proved that the factor analysis is meaningful and acceptable. On the other hand the reliability analysis of internal factors calculated by the Cronbach's alpha showed a value greater than 0.5 for all factors except factor 6, which was composed by only one item. The composition of different factors is analyzed considering the items associated, with a value greater than 0.4.
Principal components with varimax rotation solutions of JSPE-sv items.
| Item* | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 |
|---|---|---|---|---|---|---|
| Compassionate care | ||||||
| 1. Physicians’ understanding of their patients’ feelings and the feeling of their patients’ families does not influence medical or surgical treatment | 0.444 | 0.432 | −0.103 | −0.286 | −0.206 | 0.056 |
| 7. Attention to patients’ emotions is not important in history taking | 0.602 | 0.052 | 0.137 | 0.112 | 0.026 | 0.211 |
| 8. Attentiveness to patients’ personal experiences does not influence treatment outcomes | 0.676 | 0.086 | 0.057 | 0.199 | 0.005 | 0.052 |
| 11. Patients’ illnesses can be cured only by medical or surgical treatment; therefore. physicians’ emotional ties with their patients do not have a significant influence in medical or surgical treatment | 0.796 | 0.015 | 0.175 | 0.022 | 0.096 | −0.090 |
| 12. Asking patients about what is happening in their personal lives is not helpful in understanding their physical complaints. | 0.493 | 0.078 | 0.327 | −0.064 | 0.246 | 0.184 |
| 19. I do not enjoy reading non-medical literature or the arts | 0.502 | 0.065 | −0.045 | 0.367 | 0.010 | −0.447 |
| Perspective taking | ||||||
| 9. Physicians should try to stand in their patients’ shoes when providing care to them | 0.067 | 0.766 | 0.121 | 0.007 | 0.097 | 0.004 |
| 10. Patients value a physician's understanding of their feelings which is therapeutic in its own right | 0.387 | 0.425 | 0.331 | −0.077 | −0.124 | −0.200 |
| 13. Physicians should try to understand what is going on in their patients’ minds by paying attention to their non-verbal cues and body language | 0.158 | 0.476 | 0.291 | 0.086 | −0.085 | −0.017 |
| 17. Physicians should try to think like their patients in order to render better care | −0.075 | 0.789 | 0.037 | 0.242 | 0.049 | 0.179 |
| Cognitive dimension | ||||||
| 2. Patients feel better when their physicians understand their feelings | −0.068 | 0.199 | 0.755 | 0.046 | 0.087 | −0.011 |
| 4. Understanding body language is as important as verbal communication in physician-patient relationships | 0.288 | 0.011 | 0.591 | 0.048 | −0.031 | 0.260 |
| 15. Empathy is a therapeutic skill without which the physician’ s success is limited | 0.225 | 0.054 | 0.384 | 0.379 | −0.100 | −0.078 |
| 16. Physicians’ understanding of the emotional status of their patients, as well as that of their families is one important component of the physician-patient relationship | 0.306 | 0.324 | 0.506 | 0.329 | 0.089 | −0.275 |
| Contributions to clinical outcome | ||||||
| 5. A physician's sense of humor contributes to a better clinical outcome | −0.020 | 0.012 | 0.118 | 0.800 | −0.071 | 0.144 |
| 14. I believe that emotion has no place in the treatment of medical illness | 0.381 | 0.231 | −0.129 | 0.452 | 0.094 | 0.084 |
| 20. I believe that empathy is an important therapeutic factor in medical treatment | 0.362 | 0.298 | 0.375 | 0.487 | −0.102 | −0.163 |
| Standing in the patient's shoes | ||||||
| 3. It is a difficult for a physician to view things from patients’ perspectives | 0.044 | −0.007 | −0.016 | −0.009 | 0.856 | −0.037 |
| 6. Because people are different, it is difficult to see things from patients’ perspectives | 0.081 | 0.019 | 0.038 | −0.059 | 0.853 | 0.019 |
| No influence by others | ||||||
| 18. Physicians should not allow themselves to be influenced by strong personal bonds between their patients and their family members | 0.205 | 0.117 | 0.031 | 0.142 | −0.014 | 0.761 |
| % Variance | 14.44 | 10.64 | 9.4 | 8.53 | 8.29 | 5.74 |
| Alpha Cronbach | 0.67 | 0.65 | 0.55 | 0.5 | 0.72 | – |
In bold, items with eighenvalue higher than .4
The factors 1, 2 and 5 are interpreted as constructs “compassionate care”, “perspective taking” and “standing in the patient shoes”, very well supported by the literature review. The factor 1, which accounted for 14.44% of the variance, can be labeled as “compassionate care” based on the contents of the six items (1, 7, 8, 11, 12, 19). All these items also emerged as the compassionate care factor in the others studies,5,10,16,18,19 except for the item 19.
The factor 2 accounted 10.64% of the variance, a construct of “perspective taking” based on the contents of the four items (9, 10, 13, 17). All these items also emerged as perspective taking factor in the studies of Hojat,5 Alcorta-Garza10 and Kataoka16.
The construct “standing in the patient shoes” appears in factor 5 with two items (3, 6) and accounted 8.29% of the variance. The items in this construct emerged in all studies that used the JSPE-vs.5,10,16,18,19
The factor 3 which accounted 9.4% of the variance, is labeled as “Cognitive dimension” based on the contents of the four items (2, 4, 15, 16). The interpretation is based on the studies of Morse3 and Benbassat and Baumal.27
The factors 4 and 6, which do not appear in the literature review but are considered in this study having in mind the hypothesis 3, identify groups of students and explain their relation with the empathy dimension identified.
The factor 4, which accounted 8,53% of the variance, is labeled as “Clinical outcomes”, including items 5, 14 and 20. We considered that the item of this construct seems to indicate inherent characteristics that may give contribution to clinical success. The factor 6, with one item (18), “No Influence by Others” explains itself 5.74% of the variance.
Cluster analysisIn order to identify different groups of students a cluster analysis was performed using as input the values of the factors retained in the factorial analysis.
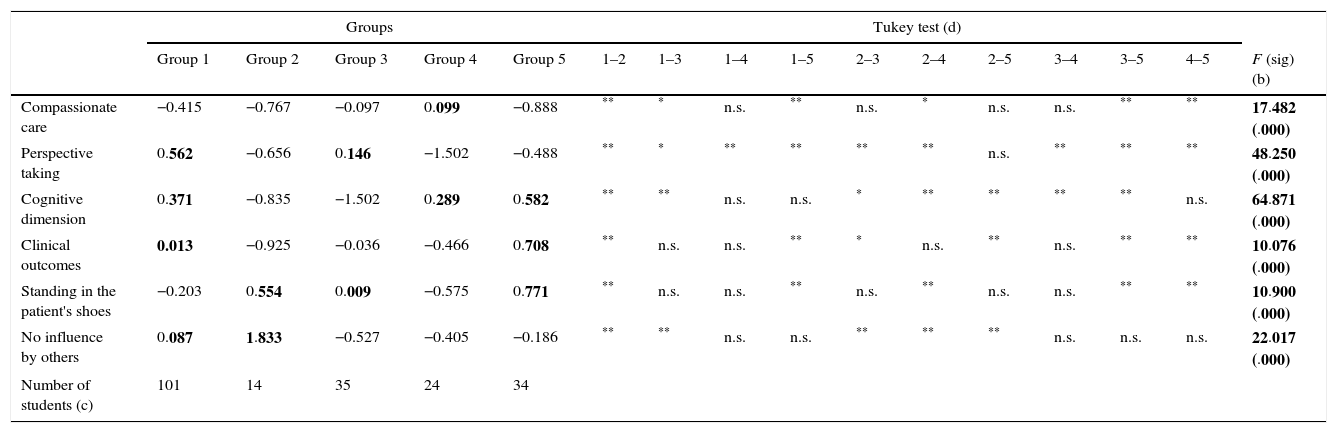
Table 4 shows the results of cluster analysis and the results of validation techniques, Oneway-Anova that supported the significance of the dimensions of empathy to include the students in identified groups (p<0.000). We can conclude that students can be grouped into five distinct groups with different perceptions of identified dimensions of empathy.
Characteristics of the five groups obtained in the cluster analysis (a).
| Groups | Tukey test (d) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | 1–2 | 1–3 | 1–4 | 1–5 | 2–3 | 2–4 | 2–5 | 3–4 | 3–5 | 4–5 | F (sig) (b) | |
| Compassionate care | −0.415 | −0.767 | −0.097 | 0.099 | −0.888 | ** | * | n.s. | ** | n.s. | * | n.s. | n.s. | ** | ** | 17.482 (.000) |
| Perspective taking | 0.562 | −0.656 | 0.146 | −1.502 | −0.488 | ** | * | ** | ** | ** | ** | n.s. | ** | ** | ** | 48.250 (.000) |
| Cognitive dimension | 0.371 | −0.835 | −1.502 | 0.289 | 0.582 | ** | ** | n.s. | n.s. | * | ** | ** | ** | ** | n.s. | 64.871 (.000) |
| Clinical outcomes | 0.013 | −0.925 | −0.036 | −0.466 | 0.708 | ** | n.s. | n.s. | ** | * | n.s. | ** | n.s. | ** | ** | 10.076 (.000) |
| Standing in the patient's shoes | −0.203 | 0.554 | 0.009 | −0.575 | 0.771 | ** | n.s. | n.s. | ** | n.s. | ** | n.s. | n.s. | ** | ** | 10.900 (.000) |
| No influence by others | 0.087 | 1.833 | −0.527 | −0.405 | −0.186 | ** | ** | n.s. | n.s. | ** | ** | ** | n.s. | n.s. | n.s. | 22.017 (.000) |
| Number of students (c) | 101 | 14 | 35 | 24 | 34 | |||||||||||
The values shown correspond to averages.
Total number of students=208.
Group 1 of the cluster analysis groups the largest number of students (101), showing a positive relationship with the dimensions “perspective taking”, “cognitive dimension”, “clinical outcomes”, “the influence by the others” and negative with dimensions “compassionate care” and “patient standing in shoes”. Group 2 of the cluster, group of 14 students, shows highly positive relationship with the dimension “no influence by others” and also positive with “standing in patient shoes” and presents negative relation with the other dimensions. Group 3 of the cluster, group of 35 students, presents positive relationship with the dimension “perspective taking” and negative or null with the others. Group 4 of the cluster, group of 24 students, shows a positive relationship with “cognitive dimension” and “compassionate care” and negative relationship with the others. Group 5 of the cluster, group of 34 students, presents a positive relationship with the “cognitive dimension”, “clinical outcomes” and “standing in patient shoes” and negative relationship with the others.
The results of post hoc Tukey, comparing the means between the different groups, give statistical support to the identified clusters.
DiscussionThe JSPE-sv is an instrument that was adapted to the Portuguese language in a study developed by Magalhães.24 According to Hojat,5 the JSPE have psychometric qualities to measure empathy in the health care setting. The aim of this cross-sectional research was to study the empathy in the context of Portuguese medical students.
The Cronbach alpha (0.77) estimated the internal consistency, for the 20 items on the JSPE-spv. In comparison, the alpha coefficient is lower than the values obtained in some studies5,16,17 and higher than the results presented in other studies.10,19,28 Curiously, this value is equal to the result obtained in study developed in other Portuguese Faculty.18Hypothesis 1 Female medical students show higher scores of empathy than do men.
In Table 2 we can see that mean females score was 116.41 and males was 109.45. The t-test of means revealed that gender difference was statistically significant (t(206)=4.348, p=0.000). This result is similar to other studies and confirms the idea that women have higher empathy when compared with men.5,9,10,13,16–18,20–23 Thus, the Hypothesis 1 is supported. According Hojat6 women showing higher levels of empathy may be due to their maternal instinct, displaying these qualities toward her infants in an eminent degree and they have a greater perception of emotions and are more receptive than more to emotional signals. Empathy is mostly a feminine trait29.Hypothesis 2 Medical students scores of empathy decline over the course.
In Table 2 we can see that the empathy scores increase from 112.85 in the 1st year to 112.74 in the 3rd year and to 116.78 in the last year of the course. No significant differences were found between the different years using an ANOVA analysis (F=2.505, p=0.084). This finding is in the same line of some studies.16–18 However, many other studies show that mean empathy scores decline during medical education.11–15 Thus, we conclude that the Hypothesis 2 is not supported by the results. According to Silver,30,31 the humanistic qualities of the medical students decline over the course, occurring as an unfortunate development of cynicism, in opposition to the results of this study.Hypothesis 3 Based on the dimensions of empathy identified it is possible to find a taxonomy of students with different emphasis related to the empathy.
After a factorial analysis it was possible to identify six different dimensions of empathy. The statistical tests support the goodness of factorial analysis (see Table 3). Three of the identified dimensions are according to the literature review: F1. compassionate care; F2. perspective taking and F5. standing in patient shoes. Two other dimensions were identified but are not supported by the literature that used the JSPE and can be characterized as, F4. clinical outcomes and F6. no influence by others. The F3. cognitive dimension, is supported by Morse3 and Benbassat and Baumal.27 These last three dimensions are retained having in mind the next research step, i.e., the cluster analysis.
According to Hypothesis 3, we tried to find different groups of students that follow the dimensions of empathy identified in the factorial analysis. Thus, using the scores of the factors retained, the data was submitted to a hierarchical method of clustering (Ward), based on the Square Euclidian Distance. This process allowed us to identify five different groups of students (see Table 4).
The F values associated to the dimensions of empathy obtained through an ANOVA analysis (p<0.000) indicate that the empathy dimensions are highly significant to include students in the groups. We use the Post Hoc Tests of Tukey to confirm that the differences between group means are significant. Thus, it is possible to say that Hypothesis 3 is supported.
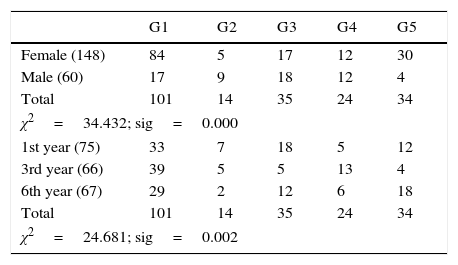
Also, we tried to find same relationships between the groups identified in cluster analysis and the characteristics of the sample of students, namely gender and year in medical school (see Table 5). It is possible to say that the distribution of students’ gender by the groups that were identified is statistically significant, as the chi-square test proves.
In the case of females, it is possible to see that they are strongly related with group 1, and this group is mainly positive related with the dimension “perspective taking”. Significant gender differences were observed in the favor of women particularly on this dimension.9 The female students also show a higher association with the group 5 characterized by its positively relation with “cognitive dimension”, “clinical outcomes” and “standing in patient shoes”.
In the case of male students, they reveal higher representation in group 2 where a positively relation with the dimensions “standing in patient shoes” and “no influence by others” exists (Tables 4 and 5). Men are more inclined to present rational solutions with low measures of emotional support and understanding.32
Taking into account the distribution of students over the course and the groups identified in the cluster analysis, it was possible to verify their distribution by various groups, supported by the chi-square analysis.
ConclusionsThe study carried out in a college of health sciences involving a sample of students from the 1st, 3rd and 6th years of medical school, sought to apply the scale JSPE-sv translated and validated in the Portuguese language, to see how medical students perceive the importance of empathy in the doctor–patient relationship.
Our results suggested that women, when compared with men, show higher values of empathy. As students progress in the course there is a greater appreciation of empathy, which contradicts some international studies, although not statistically supported. A factor analysis identifies several dimensions of empathy. A cluster analysis allowed the inclusion of students into different groups with different associations to the dimensions of empathy identified corresponding to taxonomy of students.
In the future, it will be interesting to monitorize the importance attributed to empathy by these students, through a longitudinal analysis. It will also be interesting to see whether the importance given to empathy varies according to medical specialty.
Ethical responsibilitiesProtection of human and animal subjectsThe authors state that for this investigation no experiments on humans or animals have been performed.
Confidentiality of dataThe authors declare that they have followed the ethical protocols for the data publication from patients or study participants of the Institution.
Right to privacy and informed consentThe authors state that in this paper no data from patients or participants is described. Moreover all the patients and participants were informed of the purpose of the investigation.
FundingNo financial support was provided.
Authors’ contributionMIFD contributed towards data collection, statistical processing and writing of the article. MLBR, PJFSFR and MCB were involved in the revision and correction of the article.
Conflict of interestThe authors have no conflicts of interest to declare.
Peer Review under the responsibility of Universidad Nacional Autónoma de México.